We finally started making a video of us playing CrossCribb. It took a while, partly because it takes more time to finish a game than we thought it would. If we’re playing it right, each hand or round takes about 8-10 minutes including scoring. We figure you’re supposed to play to 31, according to the rules. We played and filmed 6 rounds before our camera’s battery had to be recharged. We were 30-29 at that point with me leading.
Later when the battery was recharged, we played the 7th round. I won by a nose.
I’m not sure that making an hour long CrossCribb video will win any academy awards so I might plan this as a series of videos, one per round.
Playing it is a lot of fun! No wonder it has won awards. Knowing how to count cribbage points in cards gives you a leg up on playing and scoring.
I’ve seen several articles on Medscape about how to convince doctors to retire or even force them to retire when they’re too old to practice. The articles are titled, “How Old Is Too Old to Work as a Doctor?”; “Are Aging Physicians a Burden?”; and “When Should Psychiatrists Retire?”
The Great Resignation almost makes the debates about this moot. Doctors, including psychiatrists, are retiring or quitting in droves because of burnout, largely related to the stress of the Covid-19 pandemic in the last two years. However, a lot of physicians were quitting medicine even prior to the pandemic.
The same arguments get trotted out. Doctors often lack insight into their failing cognition and physical health as they age. How do we respectfully assess and inform them of their deficits? Are there gentle ways to move them away from active medical, surgical, and psychiatric practice and into mentoring roles to capitalize on their strengths in judgment and experience?
The decision to persuade some doctors to retire, not so much because of advancing chronological age but because of dwindling cognitive capacity and other essential skills, needs to be handled with empathy and wisdom, especially if this is going to increase the workload for the rest of the doctors holding the fort.
Like the song says, “Break it to Me Gently.”
And speaking of songs, this doctor retirement discussion reminded me of a song I heard on TV when I was a kid. I could remember just one line, “Your Love is Like Butter Gone Rancid.”
I thought I heard it on an episode of an old TV sitcom, The Real McCoys. In fact, it was from a 1968 episode of the Doris Day Show called The Songwriter. Hey, we watched what my mom wanted to watch.
The song’s awful lyrics, which Doris Day “wrote” (only as part of the show; it was actually written by Joseph Bonaduce) were tied to the melody of “My Bonnie Lies Over the Ocean”:
Your love is like butter gone rancid,
It’s no good now, it’s started to turn,
I pray that it’s just like the man said,
You can’t put it back in the churn
Can’t put
Can’t put
Can’t put it back in the churn
Oh, durn!
You can’t put it back…in the churn
The context here is that another character (Leroy) in the show had previously submitted the lyrics of a similarly bad song (“Weeds in the Garden of My Heart”) to a crooked music publishing company that lavishly praised the song and promised to publish it—at Leroy’s expense.
Leroy was clueless about getting cheated. He was too dumb to know how bad the song was, but his feelings would have been badly hurt if the family just flatly told him that. They had to figure out a way to break it to him gently. So, Doris wrote the equally terrible “Your Love is Like Butter Gone Rancid,” and performed it for Leroy and the rest of the family. Leroy thought Doris Day’s song was garbage but didn’t know how to tell her without hurting her feelings.
Doris then told Leroy she was also going to submit her rancid song to the crooked publishing company.
After Doris got the exact same letter the crooked company sent to Leroy—he learned his lesson and felt supported, gosh darn.
Anyway, I was moved to write a short song about the doctor retirement issue, “When Doctors Are Too Old to Practice,” sung to the tune of “My Bonnie Lies Over the Ocean” of course:
When doctors are too old to practice
And can’t tell your elbows from knees
When they sing old songs to distract us
It’s high time we tell them to leave
High time
High time
It’s high time we tell them to leave
Oh, beans!
It’s high time we tell them…to leave
I’ve received hundreds of billions of requests for a sing-a-long version of “My Bonnie Lies Over the Ocean” because you can’t sing the parodies unless you know the original tune.
We’ve been practicing CrossCribb and Kings Cribbage. They don’t play anything like regular cribbage, but they’re both really fun.
CrossCribb plays faster than Kings Cribbage so we played it first. Although we weren’t sure what the rule meant by saying one way to win is by “15 points or less” in a game that goes only to 31 points, we still thought it made us think about our strategy—for blocking each other.
What confused us at first is which side of the board each of is supposed to play on. In the two-player version, you sort of sit kitty corner, catty corner, or kattywumpus to each other, depending on what part of the United States you’re from. This is because one person faces the columns marked with circles and the other faces the columns marked with diamonds. That’s what the instructions tell you.
Like in regular cribbage, you choose the dealer by cutting the deck and low card gets the deal. Deal 14 cards each face down and no peeking. Non-dealer cuts and dealer turns over the cut card as usual, but places it in the center of the board.
Non-dealer leads by playing a card to anywhere on the board, which is divided into 5×5 grid, which will give 5 hands to each player to score after cards are played to each rectangular spot. You alternate play but you have to remember to toss two of your cards to the dealer’s crib, which are placed under the very handsome Dealer’s Crib chip, which reminds you of Las Vegas.
The idea is to strategically place your cards to build high scoring cribbage hands while blocking your opponent from doing the same.
The center row and column will score the Nob Jack point for you if you play a card on one of those spots. Remember, the cut card is in the center and if it’s a Jack, the dealer scores two points. However, these are not scored until after all the hands are formed on the board.
You win if you get to 31 first, which is marked in a little schematic of a cribbage scoring board on the scoresheet. However, you also win if:
You win by 15 points or less (we confess we’re not sure yet how that works)
You win by 16 points or more, which is a skunk
You win by 31 points, which is a double skunk
We each won a game, if we played it right. We’ll get this sorted out before we make a video—we hope.
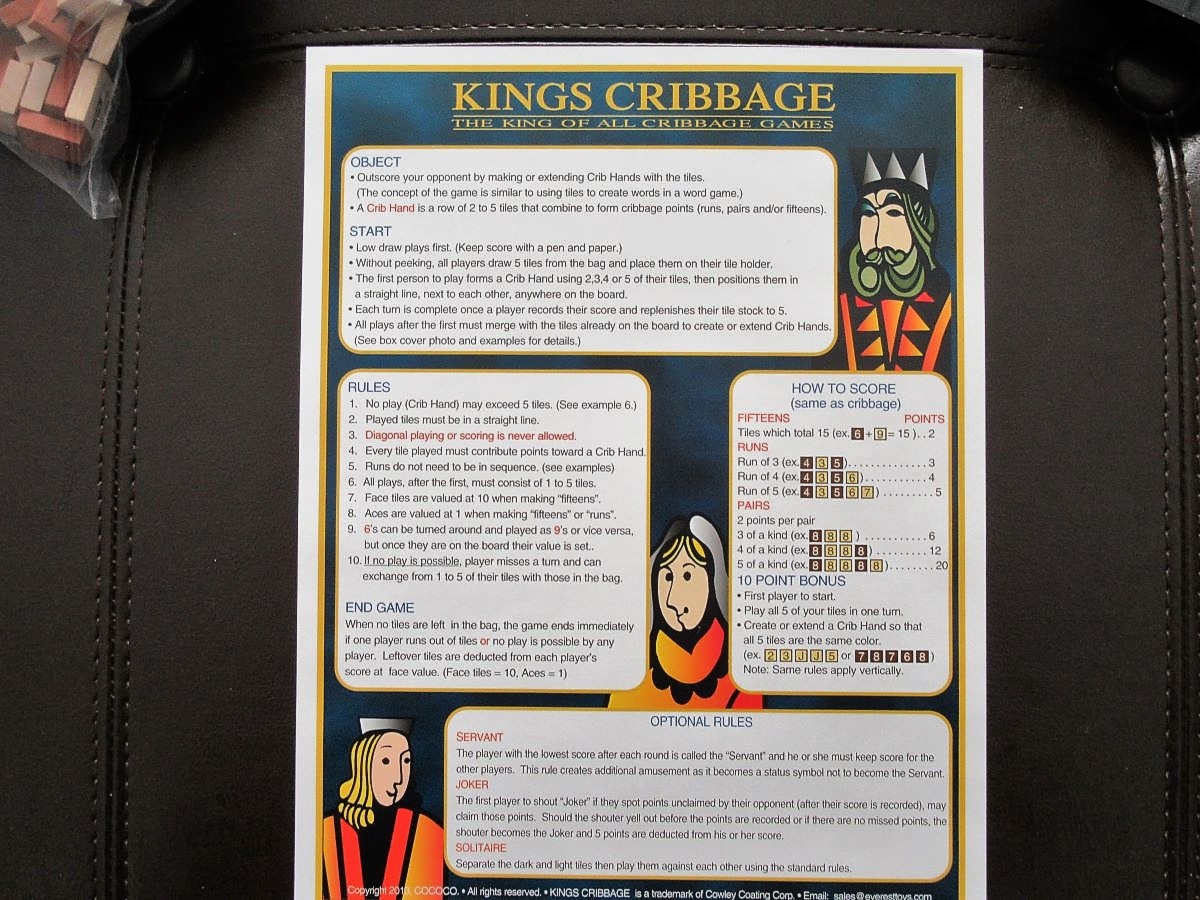
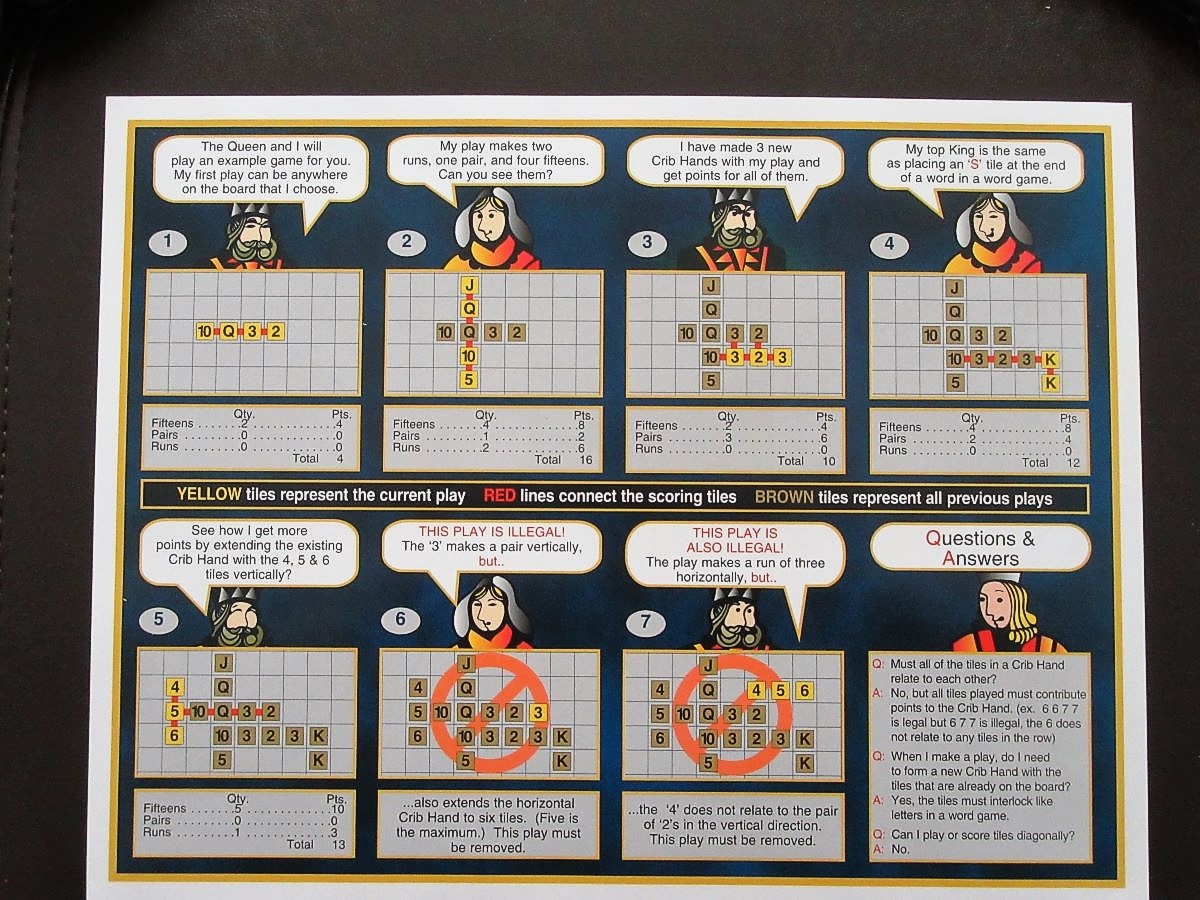
Kings Cribbage is a slower game. We played for what felt like almost an hour and a half. It seemed a little more difficult to get the hang of it, even though we play Scrabble, and Kings Cribbage is a marriage of Scrabble and Cribbage. You form cribbage hands instead of words.
The tiles are made of wood, with two different colors to represent two different suits so you can’t peek when you pick your five tiles. The tiles represent cards. First you each pick tiles to see who plays first. Low tile gets first play and can play two to five tiles anywhere on the board as long as they make valid cribbage hands. After that you can play from one to five tiles, replenishing after each play.
The board rotates so you can see what you’re doing. The first player gets a 10-point bonus right off the bat—which helped me. Normally, I lose about every Scrabble game we play, but I won this time, even without the bonus. You can only play cribbage hands that are at most five tiles long.
Those of you who know how to play each of these games can check our work. We’d appreciate it if you commented on any mistakes you find.
I ran across this article in the Portland Press Herald the other day about the renaissance of cribbage since the pandemic began a couple of years ago. It was about that time that Sena and I began again to play cribbage (in November of 2019 to be exact) after about 20 years hiatus.
We picked up the basic rules fairly quickly. It takes a while to master the game though. We are by no means masters.
In the story there is speculation that they can tell that there has been about a 20% increase in interest in cribbage because that’s about the rate at which new cribbage boards are being purchased. It’s assumed that once you have a cribbage board you don’t really want or need another one.
That’s not the case with me and Sena. We’ve purchased about a half a dozen over the last two years. To be sure, they’re not all boards. The Chicago Cribbage game variant doesn’t have a board with it but has several modifications of the rules as well as handsome cards. And we’re going to get a couple of cribbage board games, Kings Cribbage and CrossCribb.
The comments are very interesting below the story. One person claimed that his grandfather abruptly stopped teaching him cribbage when he got 29 scores in both the hand and the crib. Another commenter pointed out that this was mathematically impossible since you’d have to have more than 7 fives in the deck. Another commenter indicated that it was possible. I’m not sure what to say about the knowledge base of some cribbage players.
The story quotes David Aiken, a board member of the American Cribbage Congress (ACC) and editor of Cribbage World. He said that cribbage has been an older person’s game, for the most part. A lot of the cribbage clubs that had sponsored tournaments stopped hosting them. But that’s starting to turn around.
The story also says that cribbage takes a long time to learn and that it’s about equal parts luck and skill.
That got me to searching around on the web for other stories about cribbage and it finally led me to a story about a guy named Rollie Heath.
Rollie says the game is about 90% luck and about 15 percent skill. That’s pretty darn close to what another cribbage master said about the breakdown of luck and skill, Frank Lake. Rally mentioned the Theory of 26. This was invented by another cribbage master named DeLynn Colvert. I have Colvert’s book but have not read the chapter on the Theory of 26. Nor do I plan to, anytime soon. The gist of it is that luck controls most of the game and skill revolves around each player fighting over the 10 or so points that can actually be controlled by how you play the cards you’re dealt—I think.
Okay, okay, so I’ll read a little bit about Colvert’s 26 Theory to you. Colvert says, per hand that the non-dealer will peg on average 10.2 points. The dealer will peg 16.2 points per hand on average. Every two deals the average points add up to 26.4. Colvert goes on to say:
“The cribbage law of averages dictates that the dealer will win the game by scoring his crib hand on the 9th deal. The non-dealer will be about five (5.2) points short after counting first on the ninth hand. And this crucial five points will, on the average, caused the non-dealer to lose 56 games of 100 (skill levels being equal, of course). These averages are the foundation of the “Twenty Six Theory.”
I could probably sound real smart here by saying that nobody plays a purely statistical average game. But I’m not going to cop out. I’m just not smart enough to use the 26 Theory. More than anything, Sena and I play cribbage just for fun. I think that’s what most of us do.
On the other hand, Rollie Heath has been inducted into the ACC Hall of Fame. Maybe we should ask Rollie whether you can have 29 scores in both your hand and your crib.
Remember the Zinus platform bed and mattress (bed in a box) story? The mattress was a little on the firm side for Sena, so she ordered a Lucid 3-inch gel foam topper for it.
We got it. It’s a memory foam mattress topper, with cooling gel and aloe infused with a plush cover. It was coiled up in box, and exploded like a nuclear bomb after we opened it. We’ll have to replace the bedroom wall, but otherwise it’s a pretty nice little topper.
Just kidding.
Lucid gives you a handy little knife to cut the plastic, which worked pretty slick. The memory foam has ventilation holes to release the heat that can build up, create a 4 alarm fire, burn down your house, make you homeless for a couple years, living in a refrigerator carton over a sidewalk sewer grate which on average allows one person to fall through every 20 months in case you’re wondering, leading to meeting new people occasionally who report you to the police, who arrest you for vagrancy, though most judges are lenient, resulting in a 3 day stay hotel voucher where you can pick up a few square meals and a dozen or so bedbugs, sending you the hospital ER for treatment, after which a social worker arranges for you to move into a low budget condo with a Home Owners Association with rules against platform beds with memory foam toppers, protecting you for life as long as you don’t plant creeping charley in your side yard.
The topper flattened out in about half an hour. Sena was having to sort of jump up to get on the bed before, so now she’ll need a stepladder or a jet pack.
We finally got a sunny break yesterday and headed out to the Terry Trueblood Trail for a walk. It was good to stretch our legs. The spring birds are back. The Tree Swallow nest boxes are installed, although one of them was upside down. I’m not sure how that happens. A sparrow chased one of the swallows off, probably staking a claim on one of the nest boxes. Lucky break for the sparrow. Lucky for all that the nest boxes were available; unlucky if some are upside down, though.
The great weather was a lucky break, actually. Rain is in the forecast for the next couple of days. Talk about luck. We both got lucky playing cribbage the other day. Sena got a double run of 2 through 5 counting the cut card—and so did I. We both got 12 points. I had the crib, and got 12 more. Neither of us can recall what we threw to my crib.
Luck is important in cribbage. An expert player, Frank Lake, once said that cribbage is 85% luck and 15% skill. Others back him up.
I told the little story about a postop nurse asking me a CAM-ICU question (Will a stone float on water?) after I got back to the recovery room following my retinal detachment surgery last week. I got that one right by answering “No.” But for a split second—I had to think about it.
Sena was there and remembers the nurse also asking me if I knew the day of the week. I don’t remember that question, although Sena says I got it right.
I think I was a little hazy and probably was less than fully attentive because I got some sedation during the procedure (thank goodness).
Sena found a couple of videos that challenge the notion that the answer to the question about whether or not a stone floats on water has an obvious answer. It turns out that it all depends—on what kind of rock we’re talking about and whether a scientist is answering the question.
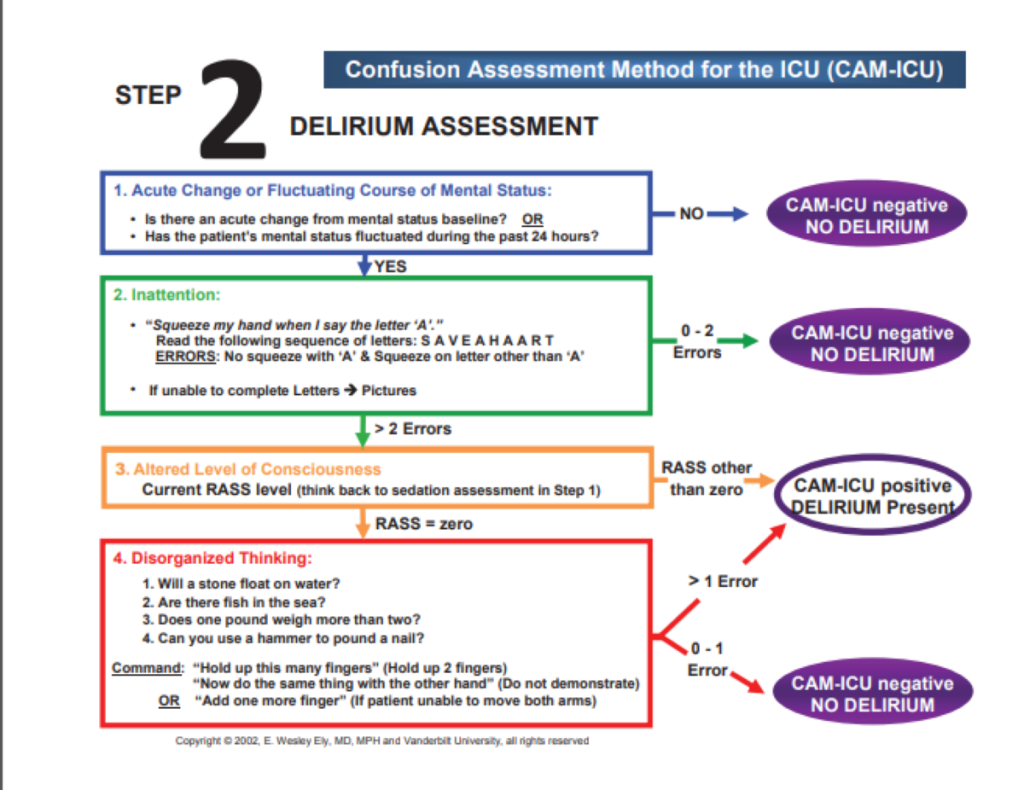
The CAM-ICU questions about thought disorganization have been outlined thoroughly, as in the picture below:
They’re in section 4: Disorganized Thinking, where you’ll see the question, “Will a stone float on water?” and others. According to the directions, you could make one “error” here and be judged not delirious.
Sena found a couple of YouTube videos that showed some rocks will, in fact, float on water. Volcanic rocks like pumice will float.
And then there are scientists like Neil deGrasse Tyson who can talk circles around you about this issue of why some kinds of rocks can float under certain conditions.
I think I was mildly delirious. But everybody took really good care of me.
Here’s another oldie but goodie blog post, “It’s Survey Time.” It’s a blast from the past (May of 2011) but it needs a short introduction on why I’m reposting it.
So, I’m about a week out from my surgery for a detached retina. I’m doing pretty well. I keep thinking about a question a nurse asked me right after I was taken to the recovery room from the operating room. I was a little hazy because I’m pretty sure I got some sedation medication, although I was definitely mostly awake for the procedure. The nurse asked me, “Well, can you answer a question for me; will a stone float on water?”
First of all, I gave the right answer, “No.” More importantly, I was momentarily stunned because I recognized the question is from the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). And I told the nurse that. It reminded me of my early career as a general hospital consultation-liaison psychiatrist.
Most of my old blog posts from The Practical Psychosomaticist are about my frustration over what seemed to be my fruitless efforts to teach nurses and physicians about how to prevent, assess, and manage delirium.
I can’t tell you how happy I was that my recovery room nurse asked me a CAM-ICU delirium screening question.
I mentioned the American Delirium Society (ADS) in the post and also found a fairly recent article on the CAM ICU. Among the authors were those I met at one of t he first ADS meetings: Malaz Boustani and Babar Kahn.
“It’s Survey Time!”:
“I know, I know, I can hear it out there, “Doesn’t Dr. Amos ever learn? Nobody does surveys and polls!” Hey, that’s OK; I have so much fun doing them anyway. Of course, it would be nice to get some responses… I’ve talked to you and I’ve talked to you, and I’m done talkin’ to you! Come back here, I’m not done talkin’ to you!
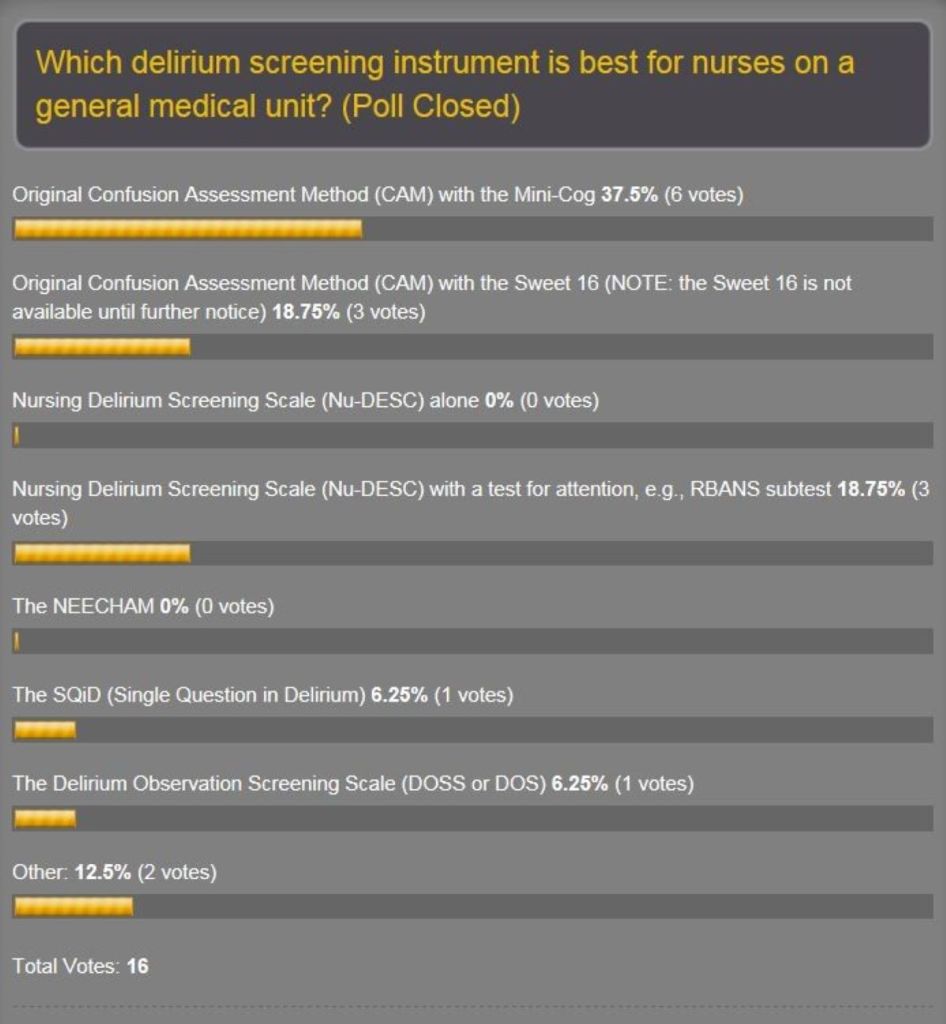
Anyway, the new poll for what’s hot and what’s not about delirium screening scales is up on the home page. The original one was partly to help our delirium prevention project committee to decide on which one to use. Well, the original got only 16 responses…but they were great responses! The amazing thing was that, despite the paucity of votes, the results were plausible. See the results:
Recall that at our 7th project meeting we selected the DOSS. What? There is good literature supporting all of these scales and a lot of factors influence selection of any tool, not the least of which is feasibility, which is mainly ease of use. That means it’s quick and doesn’t require a lot of training or additional assessments. And you should use a tool that’s validated for the patient population you want to protect from delirium. I probably got a lot of questioning looks at the screen when this poll came out because the Confusion Assessment Method-Intensive Care Unit (CAM-ICU) was not on the list. Well, you heard it from one of the main dudes on the team that developed the CAM-ICU that it’s probably not appropriate for use on general medical units…Dr. E. Wesley Ely himself (see post April 29, 2011). Hey, as far as the ICU patient population goes, the CAM-ICU is the holy grail. We need to keep looking for a sensitive and specific tool which is quick and easy for nurses to administer on general medical units.
We’re going with the DOSS. And one of my neuropsychologists, John, is offering to run neuropsychology test batteries on the patients that nurses screen with the DOSS. Atta boy, John! Neuropsychologists are going to be indispensable in this area. I remember pushing for the addition of subtests of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS), especially the Coding test in order to detect delirium early as possible. It didn’t make it, but it was close. This has been advanced by another one of our neuropsychologists here who’s done some delirium research in the bone marrow transplant unit with delirious patients. Hey, I still wonder what we could accomplish if the Coding test were added to the DOSS or even the Nursing Delirium Screening Scale (Nu-DESC). Maybe there’s already somebody out there putting a practical implementation plan for that into the real world.
So why do the poll again? Because I’d like to see if I could persuade nurses from large American and world organizations to put the nickel down and vote. And if I keep shoving this thing out there, maybe somebody will let us know that, hey, we’re not in this alone and offer to collaborate.
And I stole a couple of survey questions from our group to see what physicians and nurses think about how they manage delirium. It’s a way to take a snapshot of the culture of how docs and nurses work together on delirium recognition and interventions. And hey, why am I doing that? Because I’m a thief…no, no, I mean the reason is delirium is a medical emergency and we all need to work together to find ways to understand it better in order to prevent it. The American Delirium Society (ADS) tell you why delirium prevention is critical in the endless search to find ways to deliver high-quality medical care to patients:
Delirium Simple Facts:
More than 7 million hospitalized Americans suffer from delirium each year.
Among hospitalized patients who survived their delirium episode, the rates of persistent delirium at discharge, 1, 3 and 6 months are 45%, 33%, 26%, and 21% respectively.
More than 60% of patients with delirium are not recognized by the health care system.
Compared to hospitalized patients with no delirium and after adjusting for age, gender, race, and comorbidity, delirious patients suffer from:
Higher mortality rates at one month (14% vs. 5%), at six months (22% vs. 11%), and 23 months (38% vs. 28%);
Hospital stay is longer (21 vs. 9 days); Receive more care in long-term care setting at discharge (47% vs. 18%), at 6 months (43% vs. 8%) and at 15 months (33% vs. 11%); and
Have higher probability of developing dementia at 48 months (63% vs. 8%).
And have you registered for the ADS inaugural conference on June 5-7 in Indianapolis? Good for you! And are you going to bring back something from that conference for The Practical Psychosomaticist, and I don’t mean doughnuts? That’s the spirit! The surveys have spaces for free-text comments as well, which I want to hear!”
I heard “Oh Mary Don’t You Weep” by the Swan Silvertones for the first time earlier this evening. It kicked off ‘da Friday Night Blues with John Heim. on Jazz 88.3 KCCK. Every Friday night, Big Mo says something that sounds like, “KCCK, your blues prophylactic protecting you from the demon seeds of life.” Don’t believe me? Listen on Friday nights starting at 6:00 PM.
This song reminds me of some people I used to know.
Below is an old post from a previous blog that I published on June 6, 2010. Although the title in my record is simply PM Handbook Blog, there must have been another title. Maybe it should have been more like The Chicken Has Finally Laid an Egg (you’ll get the joke later).
There are two reasons for posting it today. One is to illustrate how the Windows voice recognition dictation app works. It’s a little better than I thought it would be. The last time I used it, it was ugly. I’m using it now because I thought it might be a little easier than trying to type it since I still have problems with vision in my right eye because of the recent retinal tear injury repair. So, instead of doing copy paste, what you’re seeing is a dictation—for the most part.
On the other hand, I’m still having to proofread what I dictate. And I still find a few mistakes, though much fewer than I expected.
The other reason for this post is to help me reflect on how far the fellowship has come since that time. It did eventually attract the first fellow under a different leader. That was shortly after I retired. It was a great step forward for the department of psychiatry:
“Here is one definition of a classic:
“Classic: A book which people praise but don’t read.” Mark Twain.
When I announced the publishing of our book, Psychosomatic Medicine, An Introduction to Consultation Liaison Psychiatry, someone said that it’s good to finally get a book into print and out of one’s head. The book in earlier years found other ways out of my head, mainly in stapled, paperclipped, spiral bound, dog eared, pages of homemade manuals, for use on our consultation service.
It’s a handbook and meant to be read, of course, but quickly and on the run. As I’ve said in a previous blog, it makes no pretension to being the Tour de Force textbook in America that inspired it. However, any textbook can evolve into an example of Twain’s definition of a classic. The handbook writer is a faithful and humble steward who can keep the spirit of the classic lively.
We must have a textbook as a marker of Psychosomatic Medicine’s place in medicine as a subspecialty. It’s like a Bible, meant to be read reverently, venerated, and quoted by scholars. But the ark of this covenant tends to be a dusty bookshelf that bows under the tome’s weight. A handbook is like the Sunday School lesson plan for spreading the scholar’s wisdom in the big book.
Over the long haul, the goal of any books should mean something other than royalties or an iconic place in history. No preacher ever read a sermon to our congregation straight out of the Bible. It was long ago observed by George Henry that there will never be enough psychiatric consultants. This prompts the question of who will come after me to do this work. My former legacy was to be the Director of a Psychosomatic Medicine Fellowship in an academic department in the not-so-distant past. Ironically, though there will never be enough psychiatric consultants, there were evidently too many fellowships from which to choose. I had to let the fellowship go. My legacy then became this book, not just for Psychosomatic Medicine fellows, but medical students, residents, and maybe even for those who see most of the patients suffering from mental illness—dedicated primary care physicians.
My wife gave me a birthday card once which read: “Getting older: May each year be a feather on the glorious Chicken of Life as it Soars UNTAMED and BEAUTIFUL towards the golden sun.” My gifts included among the obligatory neckties, a couple of books on preparing for retirement.
Before I retire, I would like to do all I can to ensure that the next generation of doctors learn to respect the importance of care for both body and mind of each and every one of their patients. That’s the goal of our book. And may the glorious chicken of life lay a golden egg within its pages to protect it from becoming a classic.”