I had my regular visit to the dentist at The University of Iowa Health Care (UIHC) today, and it was a good thing I did. For the past couple of weeks or so I’ve had cold and hot sensitivity in a couple of teeth. No surprise, the dentist found 3 teeth that needed a little work.
The dental hygienist also suggested I try using a tongue cleaner and gave me a free one. I’d never heard of a tongue cleaner before. The package advertisement (in English, French, and Spanish) says it’s for combatting bad breath, although the dental hygienist assured me in 6 different languages that she didn’t detect that problem in me.

I was there for my annual teeth cleaning but now I had 3 teeth needing work. Luckily, the dentist had an appointment in the early afternoon. It was a 3 hour wait, but I thought it was better to get it done sooner rather than later. Anticipating a visit with a dentist is sometimes almost as bad as getting in the chair and exercising my ability to refrain from flinching as the high-speed instruments whine in my ear while the dentist and the assistant do their level best to see that I gag several times in at least 9 different languages, including Klingon.
It’s hard to explain why I was having tooth sensitivity because, according to the dentist, the damage was not that severe. It wasn’t until I wandered around the hospital while waiting for the 2nd appointment that I realized I had never visited the Medical Museum on the 8th floor. And that’s where I found a possible explanation that made more sense than the modern one. It’s probably toothworms.
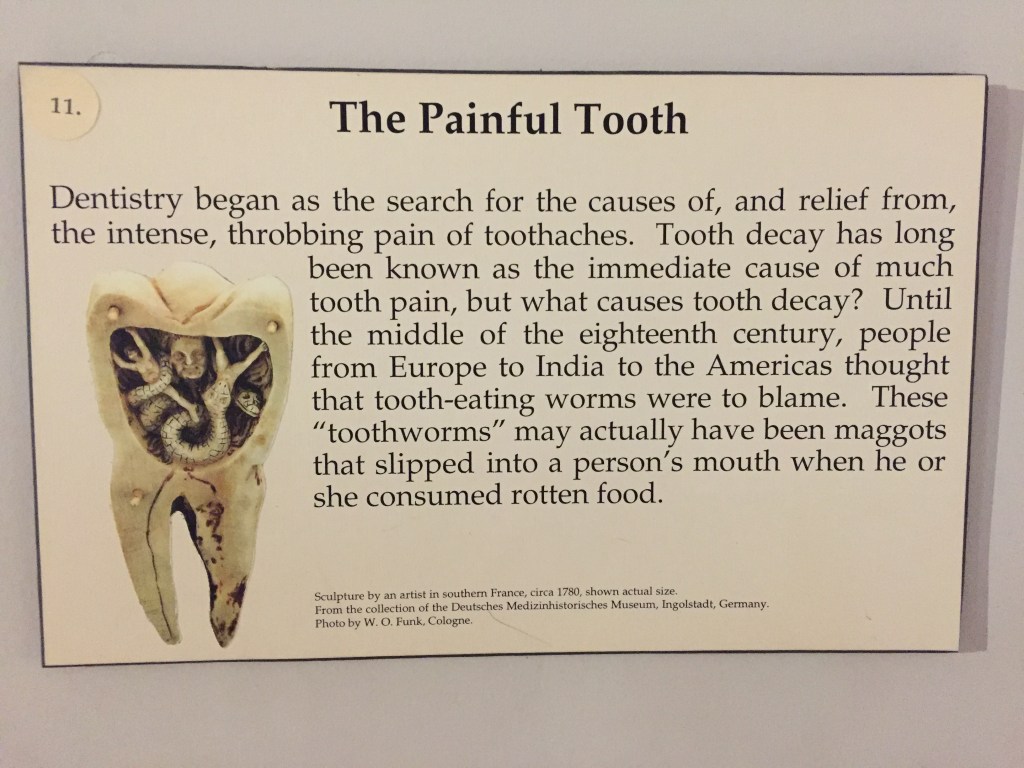
No kidding, back in the 18th century, a lot of people thought worms caused tooth decay by eating them from the inside out. There was also a College of Dentistry display in the Medical Museum featuring a typical dentist chair and samples of rusty tools, which made wonder if I should put off the filling work until, say, after my next ten reincarnations.
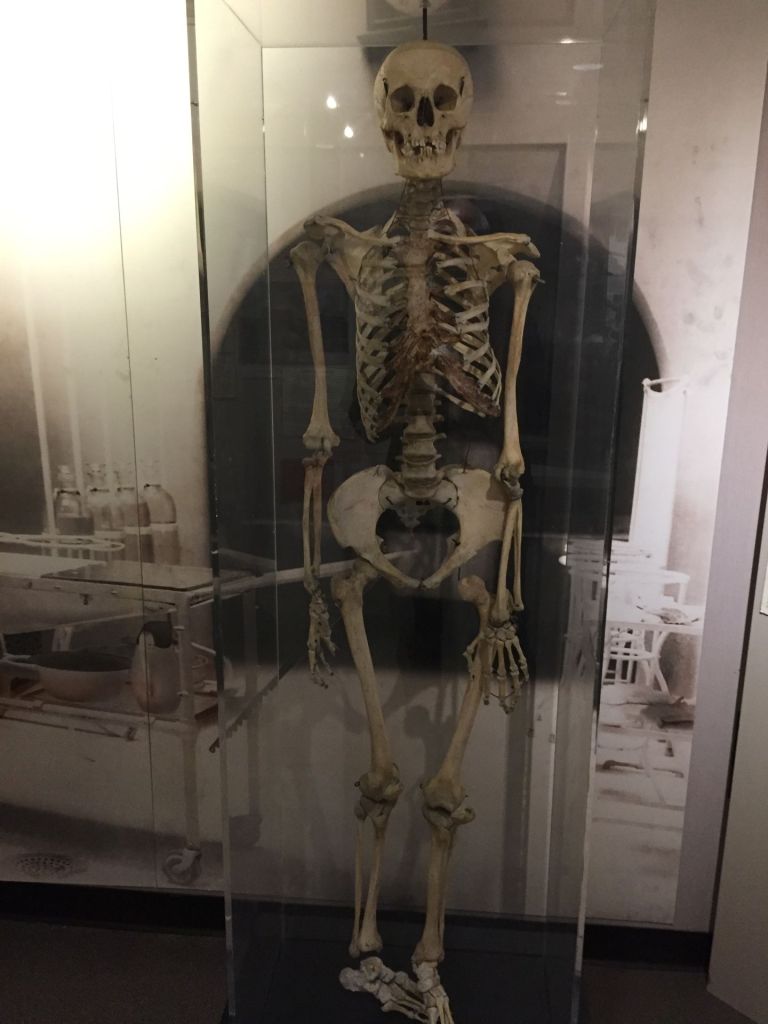
There’s a human skeleton in the museum which is affectionately called Gertie. The historical note on Gertie is very interesting in that it was thought to be a male when Ottumwa Regional Health Center donated it to UIHC in 2013. It turns out he is actually a she and the “…two symmetrical holes in the upper jaw are the result of large dental abscesses.” Just what I wanted to learn on a day when I’m anticipating dental work.
Anyway, my teeth got repaired. I would say that the UIHC dental clinic has come a long way from 1904. You don’t turn and spit in a bowl anymore. They just siphon the toothworms out with a suction wand nowadays.