We both heard a barred owl last night. This was a line of thunderstorms rolled through the area. Sena thought it was in the front yard, but there are no trees out there and it’s more likely it was in the back yard.
I searched my photo files and couldn’t find one of a barred owl, although I remarked on seeing one about 11 years ago. It was on top of a street sign and I found an old blog post about it that I wrote about on the same day. I’ll repost it below.
I found a YouTube of a barred owl making typical calls. It might have been calling for a mate. Most articles will point out that this sounds like “Who cooks for you?”
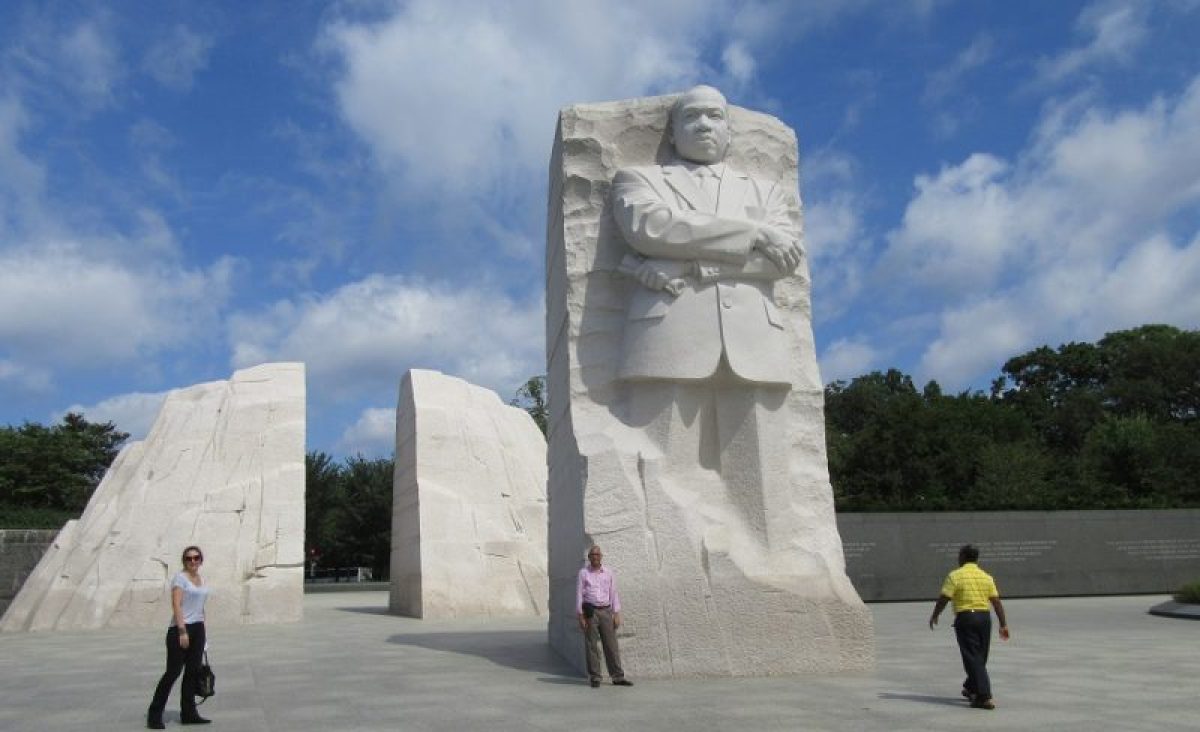
I did a google search about barred owls. When a barred owl visits you, it could mean you’re in a transition in your life. About the time I saw it in 2015, I was a couple of years away from entering the phased retirement transition of my career as a consultation-liaison psychiatrist at University of Iowa Health Care.
I’ve been retired for six years now. I wonder why a barred owl would be visiting now?
Barred Owl Visit Post 2015:
So, the other day as my wife and I were out driving we saw this owl sitting on top of a street sign on the intersection not far from our house.
He looked straight at me. I remember thinking, “Where were you when the voles were gorging on our lawn?”
I’ve never seen an owl up that close, especially roosting on a street sign at a crossroads. Of course, it got me to musing on the crossroads in which we often find ourselves at different times in our careers and at pivotal moments in our lives.
There are big and little stages, the minor and major crossroads we navigate every day and at other transitions: childhood, adolescence, college, medical school, residency, graduation, marriage, divorce, and the birth of children, the death of parents, retirement, and our own approaching death.
Recently I got a funny and thought-provoking essay about this from a former resident who is now an attending herself staffing a psychiatry consultation service at a big university hospital in Cleveland. The title of Dr. Jeanne Lackamp’s perspective article is “The Stages of Consultation-Liaison Psychiatry.” In it she describes the stages, the crossroads if you will, of the psychiatric resident in a large general hospital from the perspective of an experienced teacher [1].
I was going to say she does it with the wisdom of a wise owl, but then I thought of the owl sitting on the street sign, whose wisdom I doubted. The owl’s eyesight is keen but there was nothing but concrete on the roads leading away from its perch.
There aren’t any voles out there.
Anyway, short excerpts (which I hope are considered fair use) from Dr. Lackamp’s stages are:
Anticipation: “As though hypomanic, you will eagerly accept the CL challenge….” This is it—Your Big Chance.”
Initiation: “Coping with patient death will become real…and will make you feel sad.” You will wonder how you can possibly do multiple months of this.”
Mastery: “Cockiness may backfire…errors still occur.” “…you feel confident that No One Else could have done better given the circumstances.” “This feeling lasts; until it does not.”
Anger: “Anger will manifest in several ways…” “…it will be tempting to start second-guessing your life choice of going into medicine in general, and Psychiatry in specific.” “Sleep will be rare now too…”
Acceptance: “…you will know what you are doing—but more importantly you will realize that what you know is not everything. “…you will know that you have endured something intense and were changed by it.”
I thought of this as I listened to one of our current senior residents talk about her approaching crossroads. She’ll be a consulting psychiatrist at a private hospital.
She’s excited about it and also wanted to know that her old teacher (which is me, the wise old owl) will be available for collaboration if she needs it.
I suddenly have this craving for voles.
Reference:
- Lackamp, J. M. (2015). “The stages of consultation-liaison psychiatry.” Acad Psychiatry 39(2): 217-219.