
-

Testament to Testiness on Liaison Psychiatry
The other day, I got an email message from the Academy of Consultation-Liaison Psychiatry (ACLP). It was from the Med-Psych Special Interest Group (SIG). It was an intriguing question about a paper somebody was looking for and having trouble getting it through the usual channels. The paper was “The Liaison Psychiatrist as Busybody” by somebody…
-

An Old Blog Post About My College Days in Texas
There’s something embarrassing yet fascinating about reading my old blog posts from years ago. The one I read yesterday is titled simply “I Remember HT Heroes.” I make connections between my undergraduate college days at Huston-Tillotson College (now Huston-Tillotson University (an HBCU in Austin, Texas) and my early career as a consultation psychiatrist at The…
-
Another Look at an Old Blog Post on Psychiatric Case Formulation
I just had a look at a blog post on case formulation I wrote about 12 years ago. Aside from sounding a little pompous, I decided to check on the title I gave it back then: “What Kind of Disease Does the Person Have And What Kind of Person Has the Disease?” I looked at…
-

Shout Out to the European Delirium Association
I just want to give an enthusiastic shout out to the European Delirium Association (EDA). I rediscovered the website. It’s updated and an extremely helpful organization in the study of delirium. It provides excellent education about the disorder. I met one of the past presidents of the EDA, Alasdair MacLullich back in the early 2010s.…
-
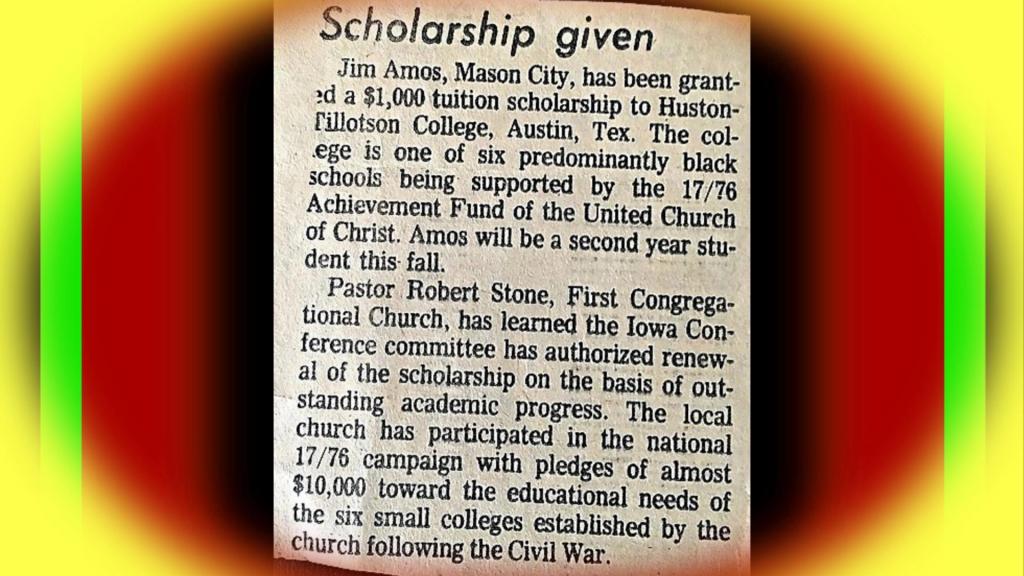
Gratitude to Pastor Robert Stone
I came across a couple of items that prompted my renewed gratitude. One of them was an article in Bloomberg on the web, “US Medical Schools Grapple With First Admissions Since End of Affirmative Action” by Richard Abbey, Ilena Peng, and Marie Patino, published on December 14, 2023. It’s about how hard it is for…
-
Time for Another Blast from the Past
I found an interesting blog post from my previous blog, The Practical Psychosomaticist. I wrote it in 2011 and it’s about the patient experience of delirium. I was delirious briefly after a colonoscopy many years ago. I don’t remember much about it. But from what Sena tells me about it, it was similar to other…
-

Rearranging My Books
The other day, I finally rearranged my bookshelf. I’ve put it off for a long time. While I was doing it, I remembered where I spend the most time in my thoughts. I don’t have a very broad library, which probably illustrates where my mind wanders. It has changed very little over the years. Retirement…
-

A Study Shows Mindfulness Is Non-Inferior to SSRI for Anxiety Disorders And What the Heck Does That Mean?
I ran across this study showing Mindfulness Based Stress Reduction (MBSR) is “noninferior” to escitalopram in the treatment of adults with anxiety disorders. I passed my Biostatistics course in medical school—barely. I have been practicing MBSR daily (for the most part) since 2014 when I really needed to address my struggle with burnout. I’m probably…
-

When Should Psychiatrists Retire?
In answer to the question in the title, I’ll confess right away I don’t know the answer. The impetus for my writing this post is the Medscape article about an 84-year-old physician who was forced to take a cognitive test required by her employer as a way of gauging her ability to continue working as…
-
On Retiring from Psychiatry
I found this very uplifting and thought-provoking article on retiring from psychiatry by Juan C. Corvalan. He sounds like he’s successfully navigating his retirement. On the few occasions I’ve felt compelled to make a remark about my own retirement, I typically say something like “It’s a mixed blessing.” My retirement is a process, unfolding as…
