Today is Labor Day, and I was looking at some of my old blog posts from my previous blog The Practical Psychosomaticist. I found one that I think I haven’t reposted on my current blog called “Going from Plan to Dirt.”
It’s a funny post, at least I think so. It draws a comparison between blue collar and white collar work, similar to what I did the other day (“Why Can’t I Wear Blue After Labor Day?”).
I wrote it in 2011, when I was on a hospital committee to improve detection and prevention of delirium in the general hospital.
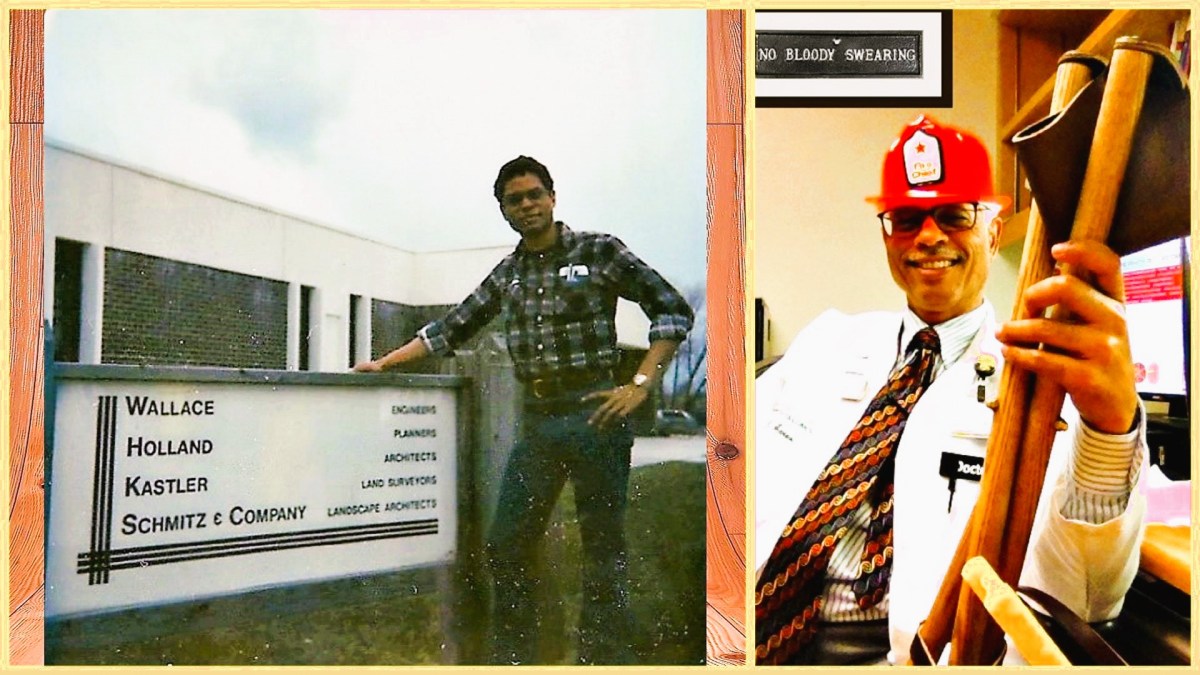
“Our work on the Delirium Early Detection and Prevention Project reminds me of my early formative experiences working as a draftsman and land survey technician starting in 1971 with an engineering company, Wallace Holland Kastler Schmitz & Co. (WHKS & Co.) in Mason City, Iowa. I remember being amazed at how a drawing on paper could be turned into a city street, highway, bridge, or airport runway. They have a website now. I can now find written there what was modeled for me then:
“WHKS & Co. is committed to the continuous improvement of the quality of service provided to our clients.”
Then and now WHKS & Co. worked hard to create the infrastructure that we depend on and then put it into the world in a “safe, functional, and sustainable” way. Out in the field we sometimes joked about how a designer’s drawing was flawed if we couldn’t go from plan to dirt.
It’s common to believe that engineers and land surveyors deal with complex mathematical formulas, structural materials, things instead of people—an applied science in which the emotions and motivations of people play a small role. Nothing could be further from the truth.
I was 16 years old when WHKS & Co. hired me. I had no idea what engineers and land surveyors did, had no experience, and I was at a crossroads in my life. They didn’t hire me because I had any talent or asset they needed. They hired me because they were as committed to the people in the community, not just to things.
And if you think land surveying doesn’t have anything to do with people’s emotions, consider property line disputes. The survey crew I was attached to had been sent out to find the property corners of two neighbors. This involves locating iron pins that mark the corners of the lots that houses sit on. Little maps or “plats” are used as guides and let me tell you, often enough we found the map is not the territory.
Anyway, while we were out there in the back yard of one of the neighbors, they both came outside. One of them was a diminutive elderly lady and the other was a tall, big-boned elderly man. They started arguing about the boundaries of their lots and it got pretty heated. Pretty soon they were yelling in each other’s faces and the lady reached down in the garden in which we were all standing. She picked up the biggest, juiciest rotten tomato she could find and it was clear to us what she planned to do with it. They were both pretty old and neither one of them could move very fast. My crew chief, sensing that something violent was about to happen, moved in between them (a decision I still can’t fathom to this day).
What followed seemed to happen in slow motion, in part because the combatants were so old. The man could see the lady was about to hurl the rotten tomato at him. Ducking must have been beyond his power, probably because of a stiff back. He bent his knees and leaned forward. She cocked the tomato as far back as she could and let fly, screeching, “You’re nothing but an old Norwegian!” My crew chief probably caught a seed or two. Amazingly, the tomato only grazed the top of the man’s head.
I think the altercation took a lot of both of them. They both went back in their houses after that.
It’s not hard for me to see the connection between my past and the present. WHKS & Co. was and still is committed to continuous improvement. And they were and still are all about finding a practical way to do it. If we’re going to improve the quality of care we provide patients and we propose to do it by preventing delirium, we’re going to have to use the same principles that my first employer used. And we’re going to have to be just as practical about how to go from plan to dirt.
We’re still trying to refine the charter for our delirium detection and prevention project, which is a kind of map, really. And even though the map is not the territory, it’s still a necessary guide to remind us of the goal.”