
-
Hit Them Back with Love
I didn’t get to listen to the Friday blues with Big Mo last Friday because my little Sony Dream Machine radio audio kept cutting out. But on the Friday blues of August 9, 2024, I heard a tune I liked. It was “Hit ‘Em Back” by Kenny Wayne Shepherd and Shemekia Copeland. Some blues songs…
-
Thoughts on the Homeless Mentally Ill
The homeless man who lives on the sidewalk outside our hotel reminds me of a couple of things. One is Dr. Gerard Clancy, MD who is University of Iowa Health Care Professor of Psychiatry, Professor of Emergency Medicine, and Senior Associate Dean of External Affairs. I remember Gerry, who was in the department of psychiatry…
-

The Cat is a Witness?
I have watched the Men in Black movies dozens of times, and I still get a little puzzled at the scene in which Agent J ask the deputy medical examiner (Laurel) where the cat Orion is. Orion is carrying a tiny galaxy on its collar. You’ll have to see the movie to get the context…
-

Alcohol is Bad for Old Guys
I took a quick peek at the study published recently in the Journal of the American Medical Association (JAMA) that a few news agencies are reporting on which says alcohol in moderation is bad for older persons. So much for moderation. Actually, the full abstract is: Ortolá R, Sotos-Prieto M, García-Esquinas E, Galán I, Rodríguez-Artalejo F. Alcohol Consumption Patterns…
-

Bird Watching Stories Are Like Fishing Tales
We finally got a couple of videos of a goldfinch! It has been years since I’ve been able to catch a brilliant male goldenrod and it happened last week on the Clear Creek Trail. In fact, we saw a few birds with the usual idiosyncratic behavior. Goldfinch are rocket fast and hate getting caught on…
-

Practicing the Reverse Cascade Juggling Pattern
I’ve been practicing the reverse cascade lately. It’s slow progress but faster than the shower pattern. You start with the regular cascade pattern and gradually work into making every throw over the top instead of under. I still do a lot of windmilling. I’ll get there-I think.
-
Excelsior!
The health benefits of climbing stairs are well known and I’ve talked about them before. However, you haven’t really seen stair climbing in action until you’ve watched Sena ascend the stairs in our hotel. There are 4 flights of 10 steps each. Doing it just once can puff you out. The keyword for this is…
-
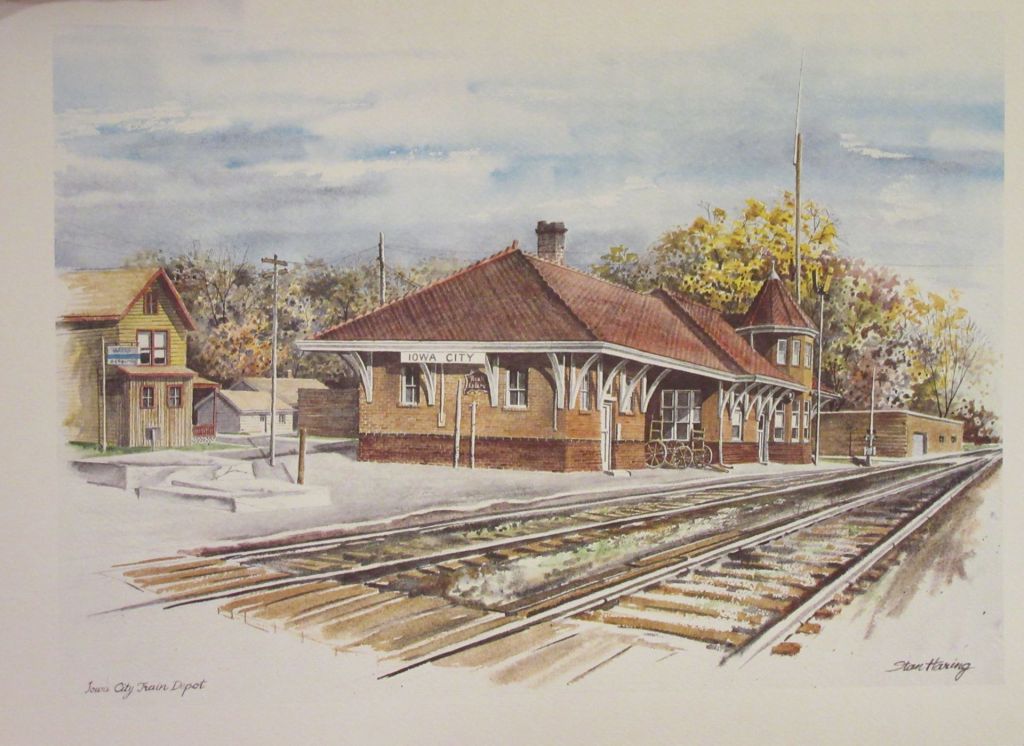
Historic Rock Island Line Depot in Iowa City
Last week while on our way to the Stanley Museum of Art, we saw the Rock Island depot at 115 Wright St in Iowa City. We’ve lived here 36 years and never visited this historic landmark before. It has interesting architecture and there is even a passenger bench inside. It was built in 1898 and…
-

Iowa City Sculptors Showcase 2024
Right on time, the Iowa City Sculptors Showcase is out in the parks. The featured pieces all have a plate on the showcase pad with a QR Code you can scan to learn more about the works. They’ll be up for two years. Tim Adams: “Exuberance” at Mercer Park, Bradford Dr; “Poppy” at Scott Park…
-
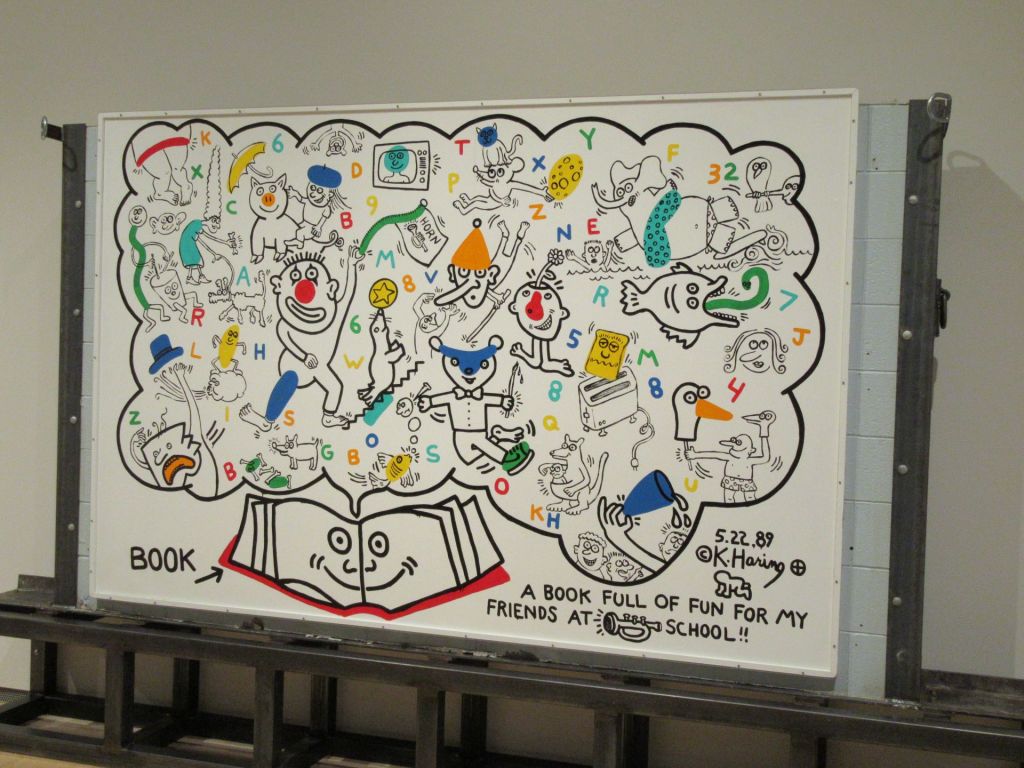
Back to the Stanley Museum of Art
We went for a return visit to the Stanley Museum of Art the other day. It’s been a couple of years. There were a couple of head sculptures outside in the front of the building. They were in honor of one of my former medical school teachers, Dr. Richard Kerber. And the Keith Haring exhibit…
