
-
Whatever Happened to the Janus Head Logo for ACLP?
I got an email from Don R. Lipsitt, MD yesterday which reminded me of the Janus Head logo for the Academy of Consultation-Liaison Psychiatry (ACLP). It was changed to another sort of nondescript logo several years ago for reasons I didn’t understand. Dr. Lipsitt is a luminary in C-L Psychiatry and recently published a definitive…
-

Hoofing it Around the Hospital
Again today, I hoofed it around the hospital. I put 43 floors and a little over 4 miles on my step counter. I don’t like waiting for elevators so I take the stairs. And a Consult-Liaison Psychiatrist is like a fireman, running all over putting out fires. I did other things today. I gave the…
-

Back in the Saddle
Well, I’m pretty tapped out, so it’ll be a short post today. I’m back in the saddle, running around the hospital on the psychiatry consult service. This is my last year of phased retirement and in 11 months—I’ll be fully retired. I put 36 floors and 3 miles on the step counter. I’m feeling every…
-
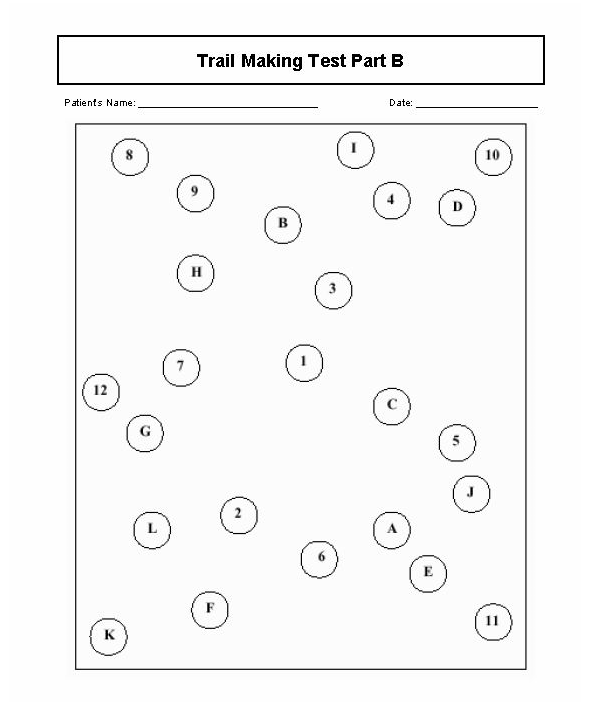
Informal Bedside Tests for Delirium
Most of this post is an updated redux from years ago about an informal bedside test for delirium called the oral trails test. I learned about it from my senior resident when I was a junior psychiatry resident in training at the VA Medical Center. There was an elderly patient admitted to the psychiatry unit…
-
Coach’s Corner: Somatoform Illness
This is a short Coach’s Corner video on somatoform and related abnormal illness behaviors which prompt physicians to request psychiatric consultation. Medically unexplained physical symptoms are not rare in the hospital and in medical clinics. The general idea is to remember Stephen Covey’s caution about effectiveness and efficiency, which is that you have a lot…
-

Just an Introduction
Well, it has been about 3 months since I opened this blog. My YouTube channel needed an updated channel trailer, so I’m posting it here as well. Why not? I was surprised at how long a minute and a half channel trailer took to make, even with the aid of video editing software (maybe because…
-
Coach’s Corner On Delirium
I’m anticipating a busy time next month on the psychiatry consultation service. I suspect delirium will be the main event, as it is most of the time. So I made a very short YouTube video on delirium. It’s cast in the style of a coach’s corner because I was one of the many clinicians who…
-
Time for July Psychiatry Consults
It’s getting close to the busiest time of the academic year in a teaching hospital–July. The residents have a steep learning curve during that month. Some hospitals have a sort of boot camp to get the upcoming first year internal medicine residents prepared for July. I’m looking at my retirement countdown timer and it’s showing…
-

The Medical-Psychiatry Unit
I guess I’m incorrigible; there are now 4 eggs in the robins’ nest. Progress there reminded me of another kind of progress–in integrated health care. On that note, this is just a brief update on the Medical-Psychiatry Unit (MPU). I thought it would be a good time to do this since a hard-working Pennsylvania psychiatrist…
-
Organ Transplant Overview
Occasionally, despite my being in phased retirement, I get a reminder that my colleagues may need some advice about an issue for which I might be a useful source of institutional memory. One of them is the psychiatric consultation for assessment of candidates for organ transplant. I have a slide set and a YouTube video…
