
Most of this post is an updated redux from years ago about an informal bedside test for delirium called the oral trails test. I learned about it from my senior resident when I was a junior psychiatry resident in training at the VA Medical Center.
There was an elderly patient admitted to the psychiatry unit who was thought to be psychiatrically ill but who actually seemed confused to me and the senior resident. We consulted medicine in order to get him transferred to the general medicine unit but it was tough going. I think the medicine resident disagreed with our clinical impression that he was confused and didn’t think medical transfer was necessary.
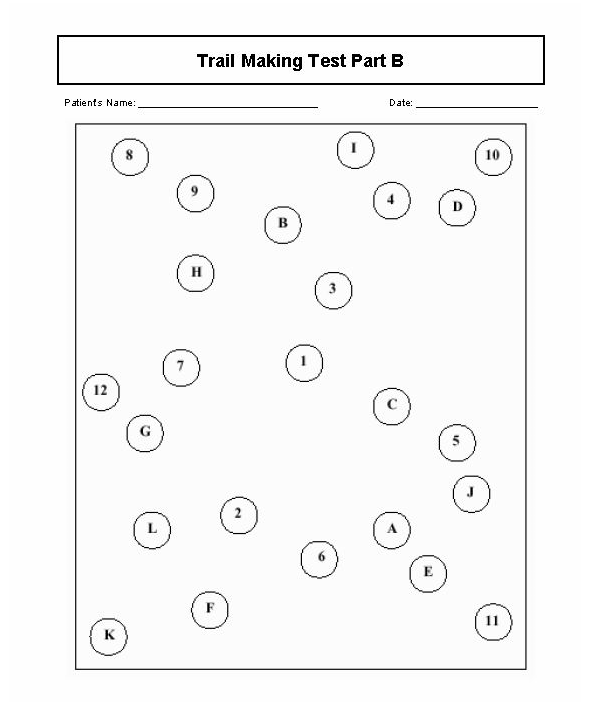
Anyway, my senior resident showed me her version of the oral version of the mixed Trails A and B Test for executive function. There is a written form which is part of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). First, she asked him to count from 1 to 7; then she asked him to recite the letters of the alphabet from A to J. She then asked him to try reciting those letters in alternating sequence. Of course, he failed miserably and was eventually transferred to internal medicine. The Trails actually is a paper and pencil test and it looks like a dot to dot game, like the example below:
My senior resident told me she learned the oral Trails test from her senior resident and couldn’t remember anything else about it. I used the test for years but a neuropsychologist criticized the practice, questioning the test’s validity, and rightly so.
Of course, I’d been doing it wrong. You’re supposed to have the patient count to 25, then recite the letters of the alphabet, then recite the numbers and letters in alternating sequence from 1 to 13 and A to M. More than two errors in pairings indicate cognitive impairment.
There are limitations to the verbal Trails and caution is advised in more recent literature, indicating that there are moderate education effects in older patients and that it may be wiser to use both paper and pencil and oral versions together.
Still the search goes on for quick and dirty ways to screen for cognitive impairment in the elderly because this and advanced age are two main risk factors for delirium.
Nowadays, I do the Mini-Cog or the Single Question in Delirium (SQiD) test, which just involves asking a family member if the patient seems confused lately.
References:
Mrazik, M., Millis, S., & Drane, D. L. (2010). The oral trail making test: effects of age and concurrent validity. Archives of clinical neuropsychology: the official journal of the National Academy of Neuropsychologists, 25(3), 236–243. doi:10.1093/arclin/acq006
Ricker, J. H., & Axelrod, B. N. (1994). Analysis of an Oral Paradigm for the Trail Making Test. Assessment, 1(1), 47–51. https://doi.org/10.1177/1073191194001001007
Sands, M., Dantoc, B., Hartshorn, A., Ryan, C., & Lujic, S. (2010). Single Question in Delirium (SQiD): testing its efficacy against psychiatrist interview, the Confusion Assessment Method and the Memorial Delirium Assessment Scale. Palliative Medicine, 24(6), 561–565. https://doi.org/10.1177/0269216310371556







Leave a comment