


Last night Sena and I watched a YouTube video walking tour of Boston, Massachusetts. It brought back memories of a trip we made there about 16 years ago. The main reason for the journey was a November teaching conference (sponsored by the Academy of C-L Psychiatry, back then called the Academy of Psychosomatic Medicine) on consultation-liaison (C-L) psychiatry I enrolled in, presented by the Mass General Hospital C-L psychiatry division. Funny, I don’t recall much about the details of the conference itself. Maybe that was because I got distracted by a bird pooping on me early on the first day.
I was on a break between programs and sitting outside the Boston Marriott at Copley Place. Suddenly I saw something white and gooey plummet inside the left cuff of my pants. It turned out to be bird poop, which led to my frantically racing back into the building to clean up.
I don’t know what kind of bird dropped that load of poop on me. It was probably a sparrow—but it could have been a seagull or even a duck, which reminds me of the highlight I can manage to remember about the trip, which was the Boston Duck Tour. I guess that means that the old story about a bird pooping on you bringing good luck might be true.
Anyway, while we didn’t have a chance to walk the Freedom Trail, we got tickets for the Duck Tour on a very chilly day. Remember, it was November. Because the annual meetings of the Academy of C-L Psychiatry were held in November, they were usually in warmer parts of the country. The Boston location was a real outlier.
We were lucky (because of the bird poop, no doubt) to find the Boston Duck Tours station at the Prudential Center on Boylston Street, practically right across the street from our hotel.
We were pretty impressed by the versatility of the Duck Tour bus, which converts readily into a boat because it’s a replica World War II amphibious DUKW vehicle.
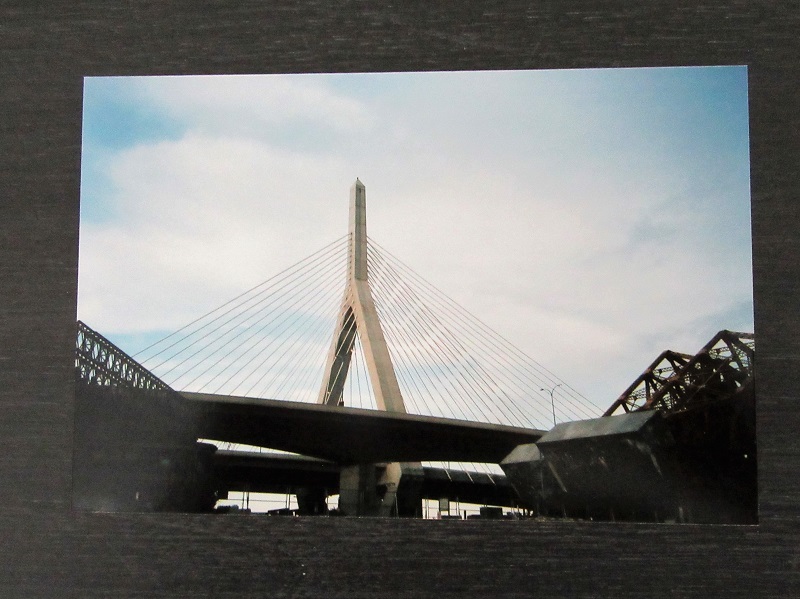
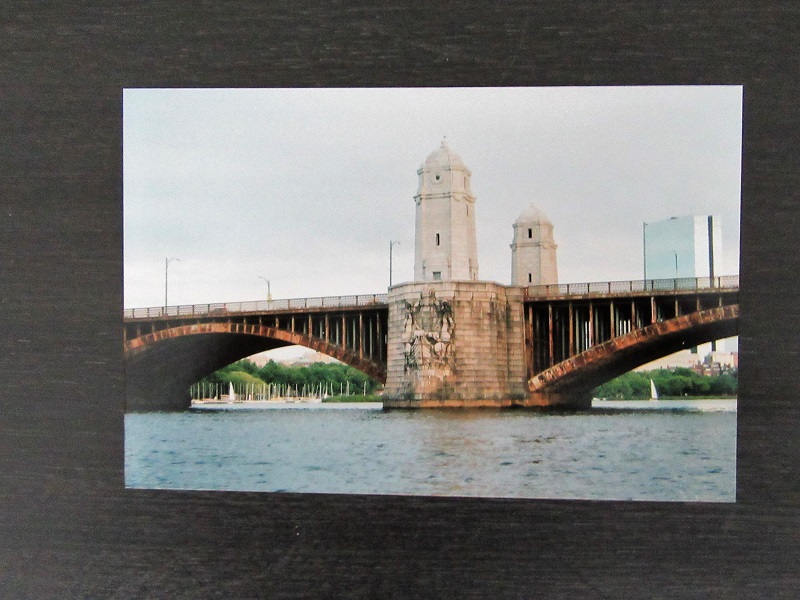
It was a fantastic sightseeing tour. I remember the Leonard P. Zakim Bunker Hill Bridge and only now do I compare it to the Longfellow Bridge (also known as the Salt & Pepper Bridge). The Zakim cost a $100 million or so new, but the repair of the much older Longfellow Bridge cost over $300 million. I’m not knocking old stuff; just sayin’.
Leonard Zakim was a famous civil rights leader whose courage and respect for the dignity and rights of others seemed to get stronger after his bout with bone marrow cancer, the pain and depression from which he dealt with by using both medical and complementary therapies.
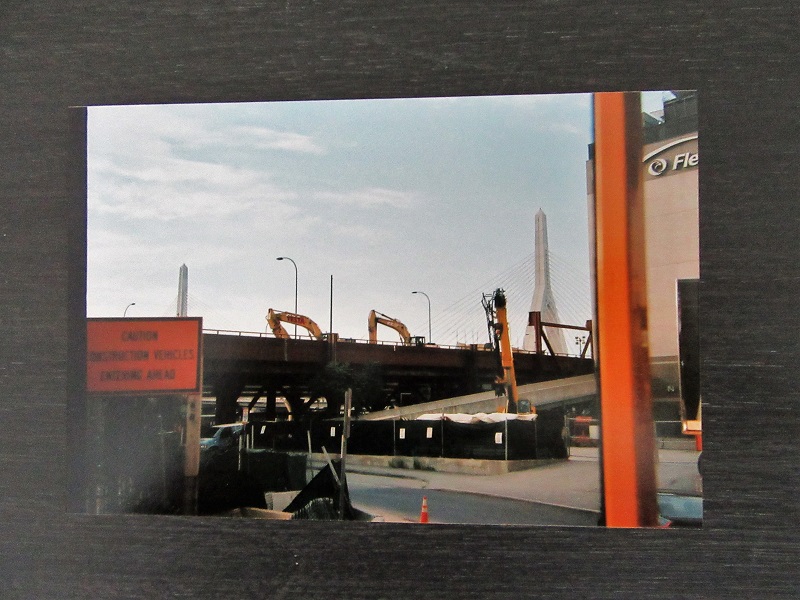
The Zakim Bridge was a part of the “Big Dig” which was a major $22 billion reroute of the main highway running through Boston and which was basically done by the time of our visit in 2004. It cost a lot of money and there has been some controversy about it.
There was also some controversy about whether the Duck Tours driver let Sena drive the vehicle while we were either crossing the Charles River or the Boston Harbor, I can’t recall which. He asked for volunteers to pilot the craft, but there were no immediate takers. He asked again and Sena spoke right up and took the driver’s seat. She’s modest about whether she actually drove the Duck.


Then again, maybe that bird poop luck kept us on course.










