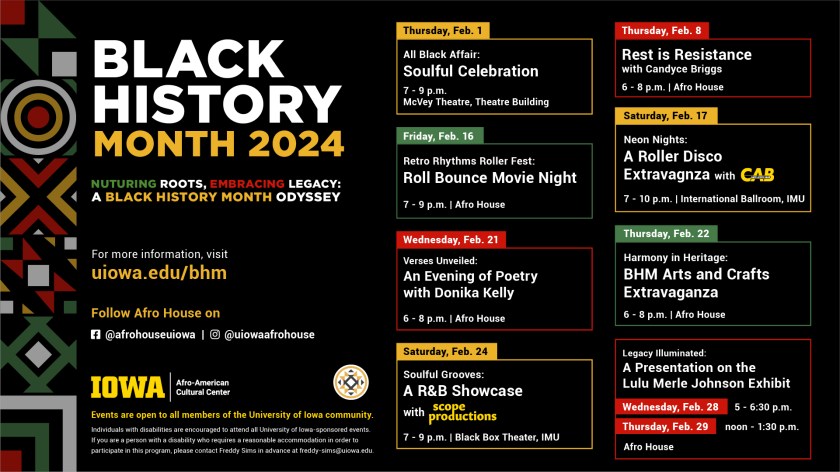
The Afro-American Cultural Center in Iowa City has many activities scheduled for Black History Month 2024. Check it out!

Sena and I viewed a recording of the Dr. Martin Luther King, Jr Distinguished Lecture given by Michele Norris on January 23, 2023. It was not available to the general public, about which I have inquired. It was a very interesting, informative, and entertaining presentation. It was about her 14-year Race Card Project which led to her new book, “Our Hidden Conversations: What Americans Really Think About Race and Identity.”
Michele opened with a little information about Bayard Rustin, which we didn’t know. There’s a film titled “Rustin,” available on Netflix which is about him and Dr. King and their complicated relationship. He was a gay black man, which was difficult for the civil rights movement leaders to accept. He was the key organizer for the 1963 March on Washington for Jobs and Freedom.
In her own words, Ms. Norris created the Race Card Project because she thought no one wanted to talk about race. She found out she was wrong because there was an avalanche of response to her request that people write something about race on a small postcard (6 words) and send it back. Interesting examples:
“Father was racist. I’M NOT. Progress!”
“Did my Southern Grandpa attend lynchings?” (This card came from Iowa.)
“Married a white girl. Now what?” (The girl thought of the guy as an “assimilated” brown man.)
“Alabama. MLK assassinated. Students cheered. Horrified.” (This was in a college classroom.)
“We aren’t all strong, black women.” (Norris’s comment was that it makes black women seem more like a weed and not a flower).
“Two white dads. Three black kids.” (Adorable photo included of gay married men with three adopted black children.)
“Can someone help me find my privilege?” (Photo of a white man included. Ms. Norris said that most of the cards are from white people, which surprised her.)
“My name is Jamaal. I’m white.” (Include a picture of a white guy. This was a story about Iowa. The guy showed up for a job interview, and the receptionist says “I thought you would be taller.”)
“Vote for Obama. Look like me.” (White guy married to white gal; they adopted black girl. I think he meant, in the abstract, that no matter what color you or the candidate are you should vote based on whether the person is qualified for the job. It’s funny that his very young daughter commented on it in a predictably concrete way given her age. She said she lived in Iowa and didn’t see too many people who looked like her. Ms. Norris said this story would be included in the book.)
It’s tough to express complicated ideas in just six words.
Ms. Norris says it’s unlikely that we’re going to agree with each other. She wants to build bridges across the chasm which divides us and she is hopeful about our ability to do that. We ordered her book.
I ran across a recently published web article that originated from the Wall Street Journal (WSJ), to which I don’t have access because I’m not a subscriber. The title is “Do Younger or Older Doctors Get Better Results?” and it’s in the form of an essay by Pete Ryan.
It’s been picked up by over 130 news outlets and is actually based on an open access study published in the British Medical Journal (BMJ) in 2017, (BMJ 2017;357:j1797): Tsugawa Y, Newhouse J P, Zaslavsky A M, Blumenthal D M, Jena A B. Physician age and outcomes in elderly patients in hospital in the US: observational study BMJ 2017; 357:j1797 doi:10.1136/bmj. j1797.
I had a quick look at the rapid response comments. A couple resonated with me. One was from a retired person:
“I did not see specific patient age statistics vs physician age groupings. Wouldn’t older patients, whose risk of dying soon was higher, want to see their own older doctors? Lots of uncontrolled variables in this study… I also agree with one of the other comments that a patient who knew the end of their life was near would seek care from an older physician that would tend to be more empathetic with a patient of their own age.”
Another was from an emergency room physician, Dr. Cloyd B. Gatrell, who entered the comment on June 8, 2017. Part of it echoed my sentiments exactly:
“The authors’ own statements call their conclusion into question: “Our findings might just as likely reflect cohort effects rather than declining clinical performance associated with greater age….”
I suspect most of the web articles spawned by the study didn’t really talk about the study itself. They probably were mainly about your attitude if the doctor who entered the exam room had gray hair or not.
The study involved internal medicine hospitalists and measured mortality rates comparing physicians were in different age ranges from less than 40 years to over 60.
It got me wondering if you could do a similar study of younger and older psychiatrists. Maybe something like it has been done. I’m not sure what an appropriate outcome measure might be. If you focus on bad outcomes, completed suicides are probably too rare and can involve psychiatrists of any age. The quote that comes to mind:
“There are two kinds of psychiatrists—those who have had a patient die by suicide, and those who will.”
Robert Simon, MD, forensic psychiatrist
I doubt they would fall into any particular age category more often than any other.
Anyway, on the subject of physicians who are getting older and required to retire at a specific age, recent news revealed that Scripps Clinical Medical Group agreed to pay almost $7 million to physicians to settle an age and disability discrimination charge filed with the U.S. Equal Opportunity Commission over a policy requiring them to retire at age 75.
And this reminds me of an article in Hektoen International A Journal of Medical Humanities: Jean Astruc, the “compleat physician.” He was a doctor in the Age of Enlightenment and was a geriatrician. An excerpt from the article:
Jean Astruc had a special interest in geriatrics and in 1762 gave a series of lectures that were taken down by one of his students. He described how in old age the skin becomes thick and hard, the hair and teeth fall out, there becomes need for glasses, respiration becomes labored, urine escapes, there is insomnia, and people forget what they have done during the day but remember every detail of what they have done in the distant past. He recommended diet, some wine to help the circulation, exercise, long sleep, and “a life from bed to table and back to bed.”
I think there is a contradiction in Astruc’s recommendations.
I retired voluntarily a little over 3 years ago. It just so happens that one of the reasons was the Maintenance of Certification (MOC) program, which the BMJ study authors mentioned in the first paragraph of the introduction:
“Interest in how quality of care evolves over a physician’s career has revived in recent years, with debates over how best to structure programs for continuing medical education, including recent controversy in the US regarding maintenance of certification programs.”
That reminds me that I got an email a few days ago from Jeffrey M. Lyness, MD, the new President and CEO of the American Board of Psychiatry and Neurology (ABPN) in January of 2023, replacing Larry Faulkner, MD. It was a letter explaining how I could recertify. I decided not to renew several years ago and I’m not thinking of coming out of retirement. I have always been an opponent of the MOC.
Maybe he sent me the letter because he found the Clinical Chart Review Module on delirium that a resident and I made in 2018. As of January 24, 2024 you can still find the module on the web site just by typing in the word “delirium” in the search field. It could be the only document about delirium on the ABPN web site, although that’s difficult to believe.
On the other hand, it’s one of two modules that are labeled as approved although valid through December 31, 2023. Maybe it’s headed for retirement.
I just saw an article in the Daily Iowan about the importance of knowing how to avoid frostbite during wind chill advisory and warning periods. As a consulting psychiatrist in the general hospital, I saw what can happen to people who suffered frostbite injuries. They were treated on the Burn Unit.
The risk for frostbite will continue to be high for the next few days with wind chills as low as minus 30 below zero, according to the National Weather Service.
The University of Iowa Hospital has a frostbite education web page worthing reviewing. There is also a compelling story posted in 2022 about how two patients were treated for severe frostbite injuries.
Here’s another blast from the past about Complexity Intervention Units (CIUs) or what used to be called Medical-Psychiatry Units. I co-staffed one for 17 years at Iowa Health Care, the organization formerly known as Prince. No wait, that used to be called the University of Iowa Hospitals & Clinics. They’re rebranding.
I was looking up CIU on the web. It’s a common search term now, so Roger Kathol, the guy who built the CIU at Iowa Health Care, was right.
On the other hand, I was also puzzled when the results showed that a hospital in Wisconsin has what’s called a brand new CIU-only it’s not a psychiatric unit.
I thought a CIU was, by definition, a combined specialty unit, with facilities for acute care of both psychiatric and medical problems. But Froedtert Medical Center in Milwaukee has a new CIU and yet says: “The department is licensed as a Medical Unit – not a Psychiatric Unit.”
In fact, Medical College of Wisconsin says essentially the same thing about the CIU: “Please note that the CIU is not an inpatient psychiatric unit, but rather a facility dedicated to integrated care.”
OK, so I probably missed the memo about what a CIU is nowadays. It’s tough to find out how many CIUs are in operation in the U.S., maybe partly depending on how you define it and who you ask. Anyway, this is what I wrote about them 12 years ago:
The Complexity Intervention Unit for Managing Delirious Patients
Is there such a thing as a specialized unit in the general hospital where patients with delirium could be treated, where both their medical and behavioral issues could be managed by nurses and doctors specifically trained for that purpose? It turns out there is. Although they are usually called medical-psychiatry units, an internationally recognized expert about designing and staffing these specialized wards, Dr. Roger Kathol, M.D., F.A.P.M., would prefer to call them “Complexity Intervention Units” (CIUs). It’s a mouthful, but it’s a better description of the interaction between physical and psychiatric illness, along with social and health care system challenges typically managed in these units.
We’ve had one at Iowa since Dr. Kathol started it in 1986. It was one of the first such units built and now that it has been redesigned, updated, and beds with cardiac monitors added, it’s arguably the only unit of its kind in the country. The CIU allows us to provide both intensive medical and psychiatric interventions that would be all but impossible to deliver on general medical floors with psychiatric consultation. The essential features of the CIU include:
The unit is used to optimize management of a variety of patients with both medical and psychiatric diagnoses. The focus is on providing care for the 2%-4% of patients admitted to general hospitals who are too complicated to manage on either psychiatric or medical units. And it’s an excellent teaching resource for helping new doctors learn about the inevitable interaction between medical and psychiatric disorders in an environment that fosters both/and thinking. Trainees learn that delirium mimics nearly every other psychiatric disorder and how to distinguish delirium from primary psychiatric illness.
I co-staff the unit with a colleague from internal medicine when I’m not staffing the general hospital consultation service. That helps me blend the perspectives of each role. Often, acting in the role of psychiatric consultant, I can assist the generalist in managing patients with less complicated delirium without transferring them to the CIU. And for those whose behavioral challenges would be overwhelming for nurses and physicians on open medical units, it’s helpful to have the CIU option available.
While the CIU is a great resource for managing delirious patients, they are expensive to build and generally have a limited number of beds. So it’s still important to continue work on developing practical delirium early detection and prevention programs in every hospital.
There’s something embarrassing yet fascinating about reading my old blog posts from years ago. The one I read yesterday is titled simply “I Remember HT Heroes.” I make connections between my undergraduate college days at Huston-Tillotson College (now Huston-Tillotson University (an HBCU in Austin, Texas) and my early career as a consultation psychiatrist at The University of Iowa Hospitals & Clinics (now rebranded to Iowa Health Care).
My first remark about getting mail from AARP reminds me that organization is sponsoring the Rolling Stones current tour, Hackney Diamonds. And the name of my specialty was changed from Psychosomatic Medicine to Consultation-Liaison Psychiatry in 2017.
The photo of me attached to the original post reminds me of how I’ve gotten older—which also makes me hope that I’ve gotten wiser than how I sound in this essay. The pin in my lapel is the Leonard Tow Humanism in Medicine award I received in 2006.
I Remember HT Heroes
Getting membership solicitations in the mail from the American Association of Retired Persons (AARP) is a sure sign of aging, along with a growing tendency to reminisce. Reminiscence, especially about the seventies, may be a sign of encroaching senility.
Why would I reminisce about the seventies? Because I’m a baby boomer and because my ongoing efforts to educate my colleagues in surgery and internal medicine about Psychosomatic Medicine, (especially about how to anticipate and prevent delirium) makes me think about coming-of-age type experiences at Huston-Tillotson College (Huston Tillotson University since 2005) in Austin, Texas. Alas, I never took a degree there, choosing to transfer credit to Iowa State University toward my Bachelor’s, later earning my medical degree at The University of Iowa.
Alright, so I didn’t come of age at HT but I can see that a few of my most enduring habits of thought and my goals spring from those two years at this small, mostly African-American enrollment college on what used to be called Bluebonnet Hill. I learned about tenacity to principle and practice from a visiting professor in Sociology (from the University of Texas, I think) who paced back and forth across the Agard-Lovinggood auditorium stage in a lemon-yellow leisure suit as he ranted about the importance of bringing about change. He was a scholar yet decried the pursuit of the mere trappings of scholarship, exhorting us to work directly for change where it was needed most. He didn’t assign term papers, but sent me and another freshman to the Austin Police Department. The goal evidently was to make them nervous by our requests for the uniform police report, which our professor suspected might reveal a tendency to arrest blacks more frequently than whites (and yes, we called ourselves “black” then). He wasn’t satisfied with merely studying society’s institutions; he worked to change them for the better. Although I was probably just as nervous as the cops were, the lesson about the importance of applying principles of change directly to society eventually stuck. I remember it every time I encounter push-back from change-resistant hospital administrations.
I’m what they call a clinical track faculty member, which emphasizes my main role as a clinician-educator rather than a tenure track researcher. I chose that route not because I don’t value research. Ask anyone in my department about my enthusiasm for using evidence-based approaches in the practice of psychiatry. I have a passion for both science and humanistic approaches, which again I owe to HT, the former to Dr. James Means and the latter to Dr. Jenny Lind Porter. Dr. Means struggled to teach us mathematics, the language of science. He was a dyspeptic man, who once observed that he treated us better than we treated ourselves. Dr. Porter taught English Literature and writing. She also tried to teach me about Rosicrucian philosophy. I was too young and thick-headed. But it prepared the way for me to accept the importance of spirituality, when Marcia A. Murphy introduced me to her book, “Voices in the Rain: Meaning in Psychosis”, a harrowing account of her own struggle with schizophrenia and the meaning that her religious faith finally brought to it.
Passion was what Dr. Lamar Kirven (or Major Kirven because he was in the military) also modeled. He taught black history and he was excited about it. When he scrawled something on the blackboard, you couldn’t read it but you knew what he meant. And there was Dr. Hector Grant, chaplain and professor of religious studies, and champion of his native Jamaica then and now. He once said to me, “Not everyone can be a Baptist preacher”. My department chair’s echo is something about how I’ll never be a scientist. He’s right. I’m no longer the head of the Psychosomatic Medicine Division…but I am its heart.
I didn’t know it back in the seventies, but my teachers at HT would be my heroes. We need heroes like that in our medical schools, guiding the next generation of doctors. Hey, I’m doing the best I can, Dr. Porter.