
Need a little help to get started with exercising for your total health? See the video below:
Category: health care
Sena Tries Miracle Whip on Braunschweiger!

The other day, Sena suggested we have a soup and sandwich dinner. We both had a Braunschweiger sandwich on toasted bread, with onions—and Miracle Whip! Sena suggested the adding the onions and toasting the bread. She also decided to try the Miracle Whip spread. I chose the soup, which was so spicy we needed a drink of lemonade with every bite.
Usually, she prefers mayonnaise to Miracle Whip, so I was floored. In fact, adding onions on toasted bread with the sandwich was delicious! We both liked it.
Braunschweiger is also very nutritious. According to one web article, a single serving has 14 grams of protein, important for muscle growth, repair, and health overall. It also has heart healthy monosaturated fats (good for you), it’s high in Vitamin A which is great for eye health, and has many essential vitamins and minerals.
And is Miracle Whip good or bad for you? It turns out it has half the calories and fat of mayo, so it’s a healthy choice.
Sena actually liked the Braunschweiger with Miracle Whip sandwich. She made sure I put onions on the sandwiches and she liked the way I diced them. In fact, onions are also good for you. They’re low in calories and nutrient rich.
Try to pair it with a soup that it isn’t nuclear grade spicy and doesn’t require a gallon of lemonade to put out the fire.
Older adults can learn more about healthy eating and exercise at the Move Your Way link. Try it. You might like it.
Move Your Way!

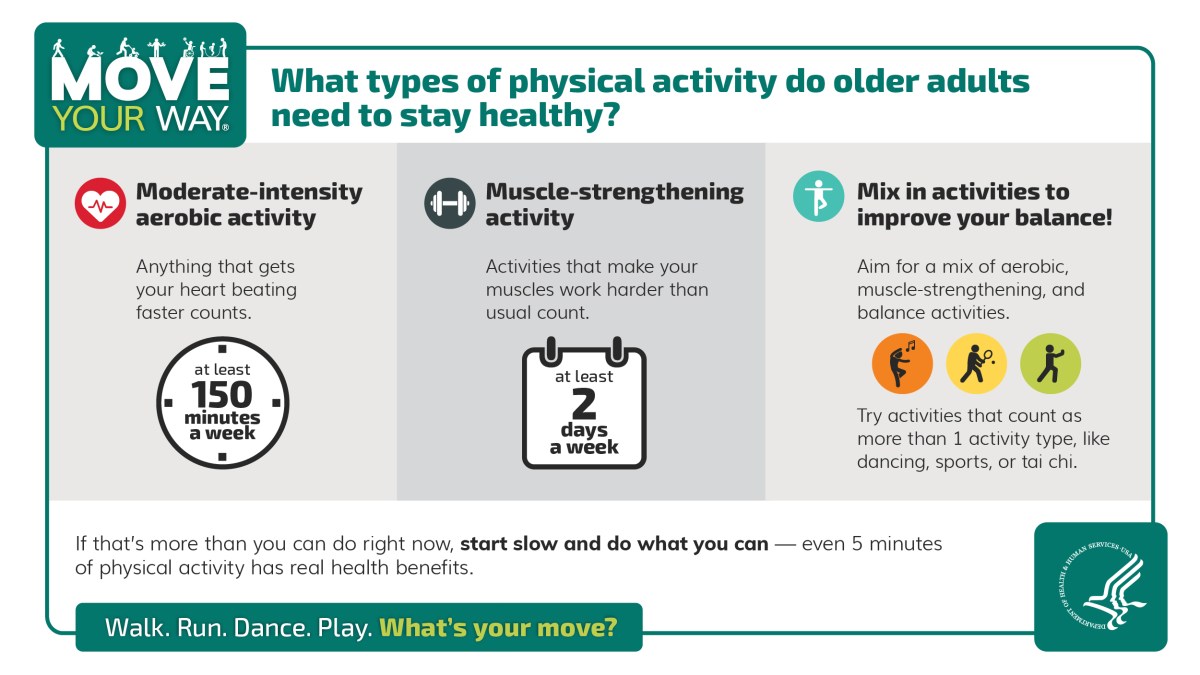
I saw the HHS Move Your Way campaign regarding the new strategy on encouraging older people to exercise, namely the Midcourse Report: Implementation Strategies for Older Adults.

There are many ways to get and stay fit. We could all do better, including me. I exercise pretty much daily for about 30 minutes. Following that, I usually sit in mindfulness meditation for 30 minutes.
The report says we should do moderate intensity aerobic activity for at least 150 minutes a week and muscle strengthening activity for at least 2 days a week.
I do a combination of stationary bicycle exercise, weight exercises with dumbbells, planks, body weight squats. I also do one leg stand, one minute each leg.
And juggling is great aerobic exercise. I struggle a bit with advanced thumb wrestling.
Raccoon in the Mulberry Tree

I was not sure what exactly I saw this between 6:30 and 7:00 this morning shaking the mulberry tree branches in our backyard. It seemed too big to be a squirrel and I dismissed the thought, telling myself that it was most likely the usual squirrel getting its mulberry breakfast.
Just prior to this incident, I had seen and heard what I thought was a blue jay in the mulberry tree. It gave a series of short whistles while bobbing up and down on the branch. I had never heard a blue jay make whistle notes, just the usual screeches. I doubted what I saw and heard. I checked my bird book, “Birds of Iowa: Field Guide” by Stan Tekiela. It didn’t mention anything about blue jays making short whistling notes and bobbing up and down as they did so. I didn’t bother to get up and try to get a video of it. It would have been through the window of our sun room and the jay didn’t sit for more than a few seconds.
So, I looked it up on the web. It turns out blue jays make a variety of noises besides the jeer. They bob up and down as a part of a courtship ritual. They make what is termed a “pump handle call” and I found a video which duplicates what I saw and heard.
Anyhow, getting back to the critter in the mulberry tree, it turned out to be a large raccoon. It was eating mulberries and I tried to take video of it as it was climbing down the tree. This reminded me of an essay by E.B. White entitled “Coon Tree.” If you’ve ever read essays by E.B. White, you probably know already that this one is about a lot more than raccoons.
It’s basically about the conflict between nature and technology. The main essay was published in 1956 and a post script was added in 1962. The coon represents nature which White idealizes and contrasts with references to new inventions, including nuclear devices which represent the destructive side of technology.
I guess we can forget for the moment that raccoons can carry diseases like rabies and roundworm. I’m also reminded of an old TV commercial in the 1970s about margarine (an alternative to butter) in which an actor says angrily, “It’s not nice to fool Mother Nature!” The idea was that margarine (which was a new invention in the late 19th century) was healthier than the natural spread, butter—although the trans fat in it makes the comparison a bit more complicated.
White also says something interesting about unsanitary homes, claiming that children who live in them become more resistant to certain diseases like polio than the kids who grow up in clean homes. The polio scourge raised its ugly head recently in New York, which renewed the recommendation by the Centers for Disease Control recently that people who didn’t get vaccinated against polio should get vaccinated—regardless of how dirty your home was.
And then there is the artificial intelligence (AI) technology. I wonder what E.B. White would say about that? AI can improve detection of some diseases and assist in medical research. On the other hand, AI can still make mistakes and it needs human surveillance.
I read you can sometimes use loud noises to keep raccoons out of your yard. For example, you could try recordings of blue jays.


Four Seasonal Vaccines for Older Adults?
There are a number of seasonal vaccines recommended for older adults in the U.S. They include vaccines for influenza, pneumonia, and the newest one is Respiratory Syncytial Virus (RSV).
I noticed that during the recent FDA meeting to decide on approval of another vaccine for the XBB variant of Covid-19, many experts objected to the use of the word “periodic” in the voting question.
Those objecting to it did so because of the implicit suggestion that Covid-19 is a seasonal virus. Not all experts agree on that. I gather it takes time to determine whether or not an infectious agent should be considered seasonal or not.
If the XBB variant of Covid-19, RSV, pneumonia, and influenza are all considered seasonal, then there are 4 vaccines for which older adults would be eligible.
The consensus among most experts is that you can take both influenza and Covid-19 vaccines at the same time. Most of us older adults also get the pnemococcal vaccine as well.
Will the RSV vaccine be added to the list? Should you get all 4 at the same time? Or should they be spaced out? Should you get the influenza and Covid-19 vaccines together and wait a week or two before getting the RSV and pneumococcal vaccines?
The increase in recommendations for vaccinations could be burdensome for those without health insurance. Vaccine uptake will probably continue to be a challenge.
