
-

More Thoughts On “Our Hidden Conversations” Book by Michele Norris
I need to correct something I got wrong in my first post about Michele Norris’s Distinguished Lecture on January 23rd. While reading her book, “Our Hidden Conversations” I ran across this race card in the chapter “Black Babies Cost Less to Adopt:” “Vote (for) Obama! He looks like me!” That was the 8-year-old daughter said…
-
Preliminary Thoughts on “Our Hidden Conversations” Book
This is a short post about my initial impressions about the book, “Our Hidden Conversation” by Michele Norris. I’m not finished with the book yet, but I thought I would let you know that the first chapter, “Bread Crumbs” was tough to read. I had to put it down and come back to it a…
-

Sweethearts on a February Stroll
Yesterday, we went out for a walk because it was a pretty nice day for February. All the snow was pretty much gone. We saw a hawk who also saw us. We approached the tree it was perched in very slowly. It tolerated our attention until we got too close for comfort—and flapped off in…
-

The Big Tomato On The Vegetable Hamburger, Please!
Sena bought a pretty big tomato at the grocery store the other day. When she picked it up, she said to a store employee that she was going to make a huge “vegetable hamburger” with it. Evidently, the guy didn’t know what to make of the name “vegetable hamburger” because he asked her why she…
-
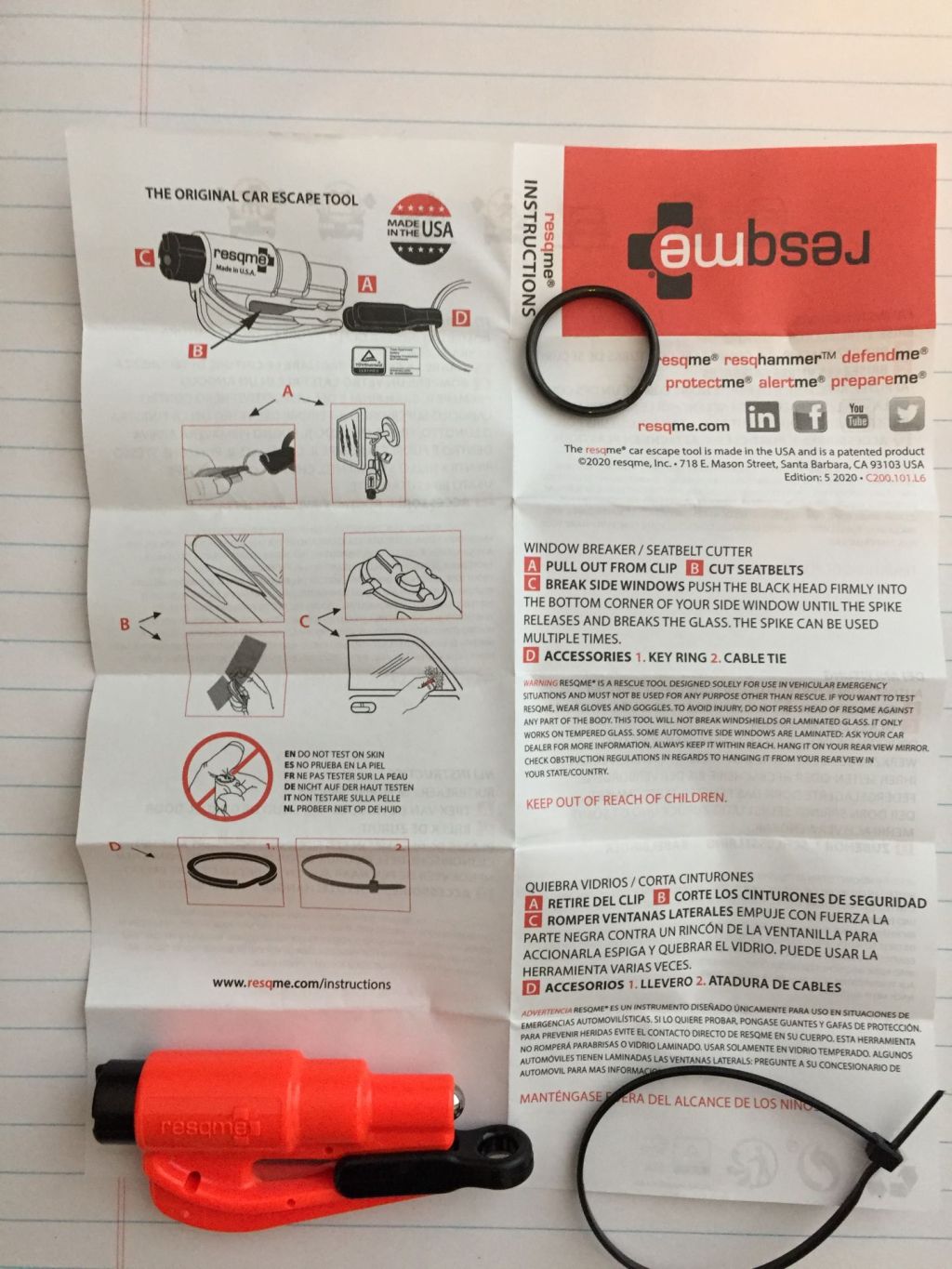
How to Remove the Blade Guard from the RESQME Car Escape Tool
I just found out how hard it is to remove that blade guard from the RESQME car escape tool. You can’t waste time busting a gut trying to pull that out when you’re about to drown while your car is sinking in a flood. You might need the blade to cut your seat belt. That’s…
-

How About That Rad Composer and Bird Watcher Antonin Dvorak?
I thought I would share a couple of ideas about the Czech composer Antonin Dvorak. I’m not a music expert by any stretch of the imagination, but I enjoy listening to classical music on the Music Choice Classical Masterpieces channel. Music Choice always have interesting bits of biographical information about the musicians. The items about…




