


I read a short article, “The case for pursuing a consultation-liaison psychiatry fellowship” by Samuel P. Greenstein, MD in Current Psychiatry (Vol. 1, No. 5, May 2022). After 3 years as an attending, he found his calling as a C-L psychiatrist, especially after getting teaching awards from trainees. But when he applied to academic institutions for position as a C-L academic psychiatrist, people kept advising him to complete a fellowship training program in the subspecialty first. He gave it careful thought and did so, even he called it going “backwards” in his career.
On the other hand, he believes C-L fellowships will help meet the challenges of addressing rising health care costs and improving access to what most people see as the critically important goal of providing access to integrated mental health and medical care.
I’ve been retired from consultation-liaison psychiatry for two years now. I get an enormous sense of achievement on the rare occasions when I hear from former trainees who say things like “For me you were…one of the most outstanding attendings I had at my time at Iowa.” And “I can at least take comfort that University of Iowa is still at the forefront of psychiatry.”
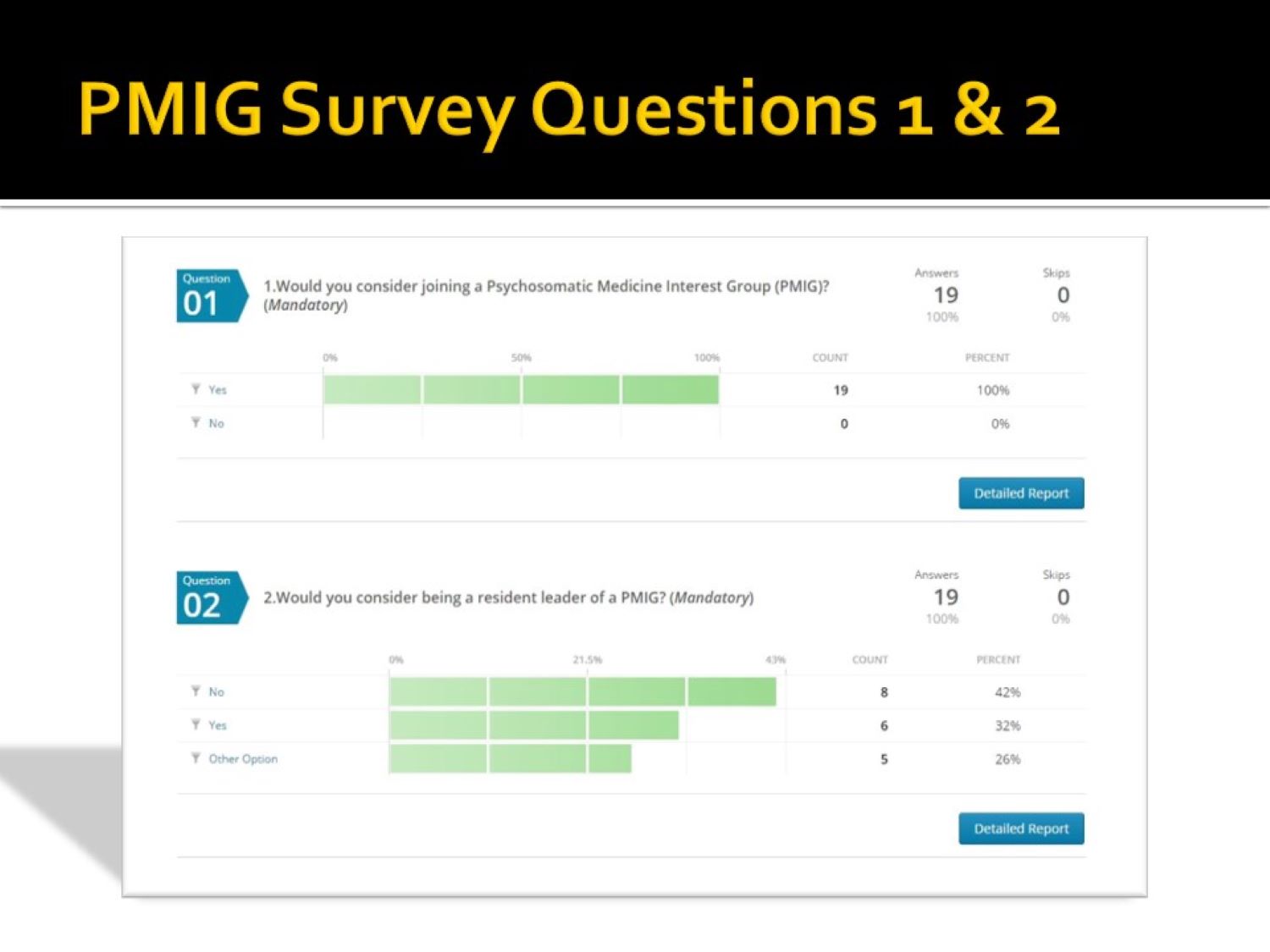
Several years ago, one of the residents suggested starting a Psychosomatic Medicine Interest Group (PMIG). This was before the name of the subspecialty was formally changed to Consultation-Liaison Psychiatry in 2018. I know many of us were very pleased about that.
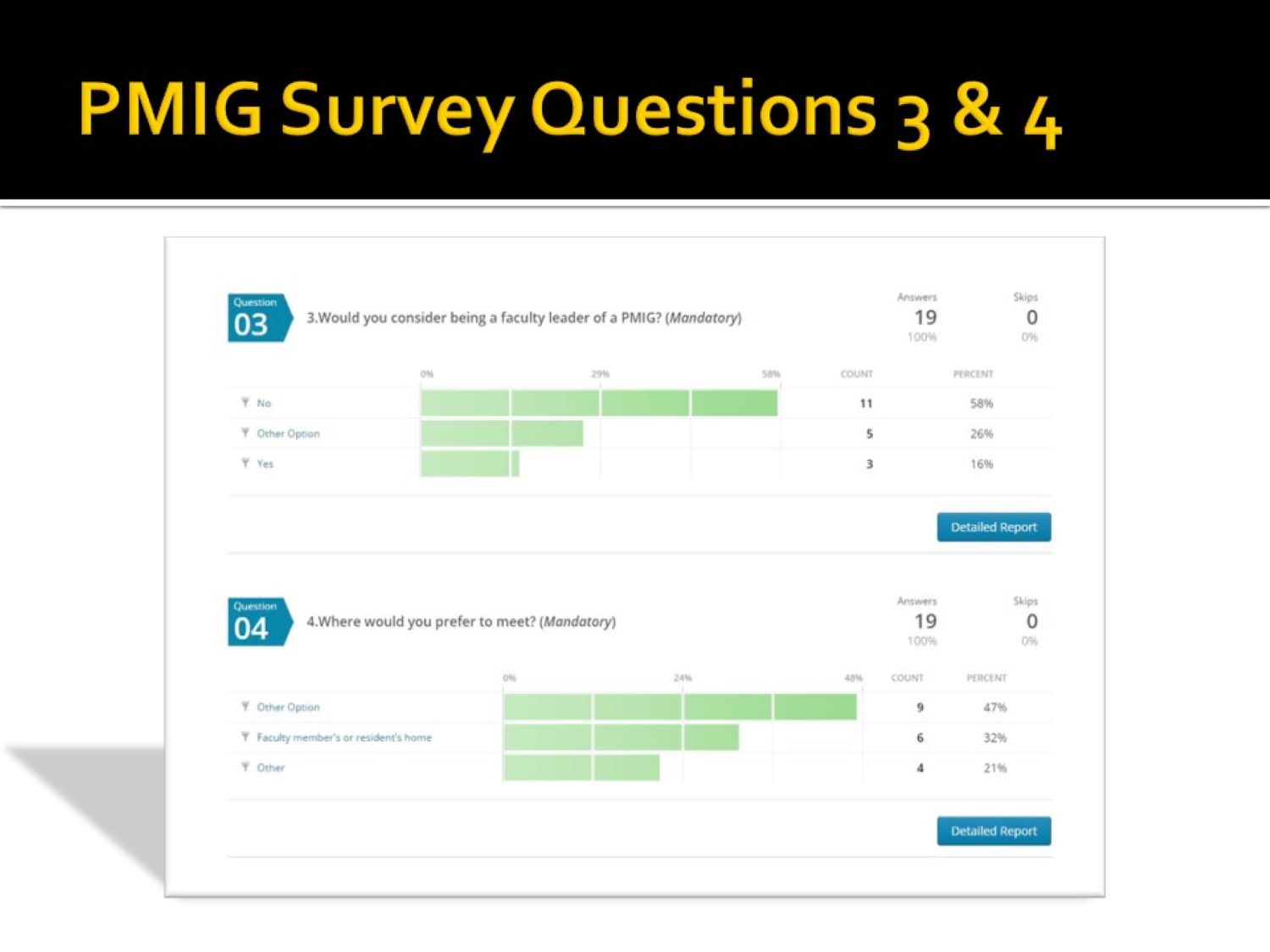
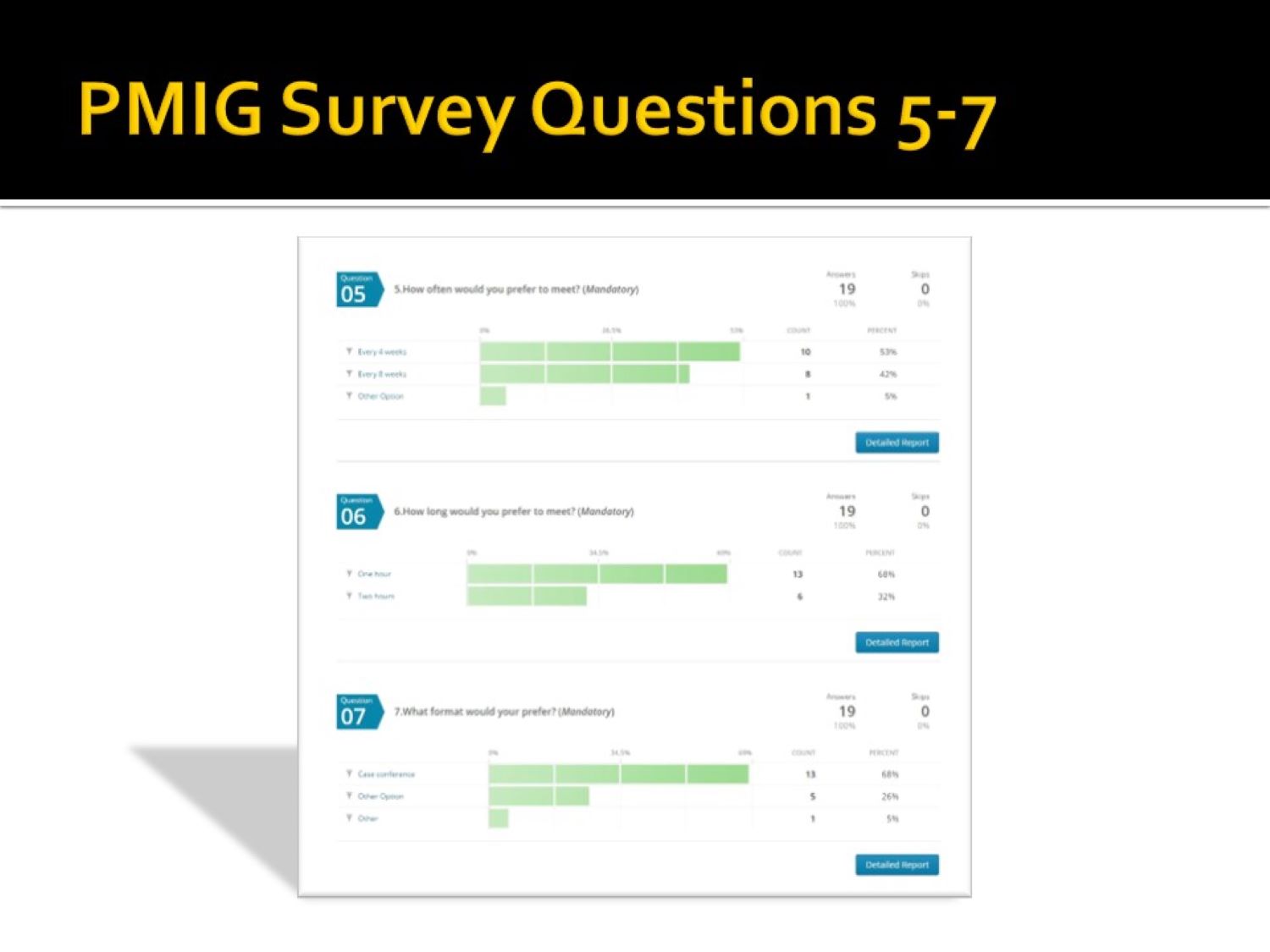
I sent a short survey (see the gallery below the slide show) to the faculty and residents in an effort gauge support for the idea and readiness to participate. I used a paper published at the time to guide the effort, (Puri NV, Azzam P, Gopalan P. Introducing a psychosomatic medicine interest group for psychiatry residents. Psychosomatics. 2015 May-Jun;56(3):268-73. doi: 10.1016/j.psym.2013.08.010. Epub 2013 Dec 18. PMID: 25886971.).

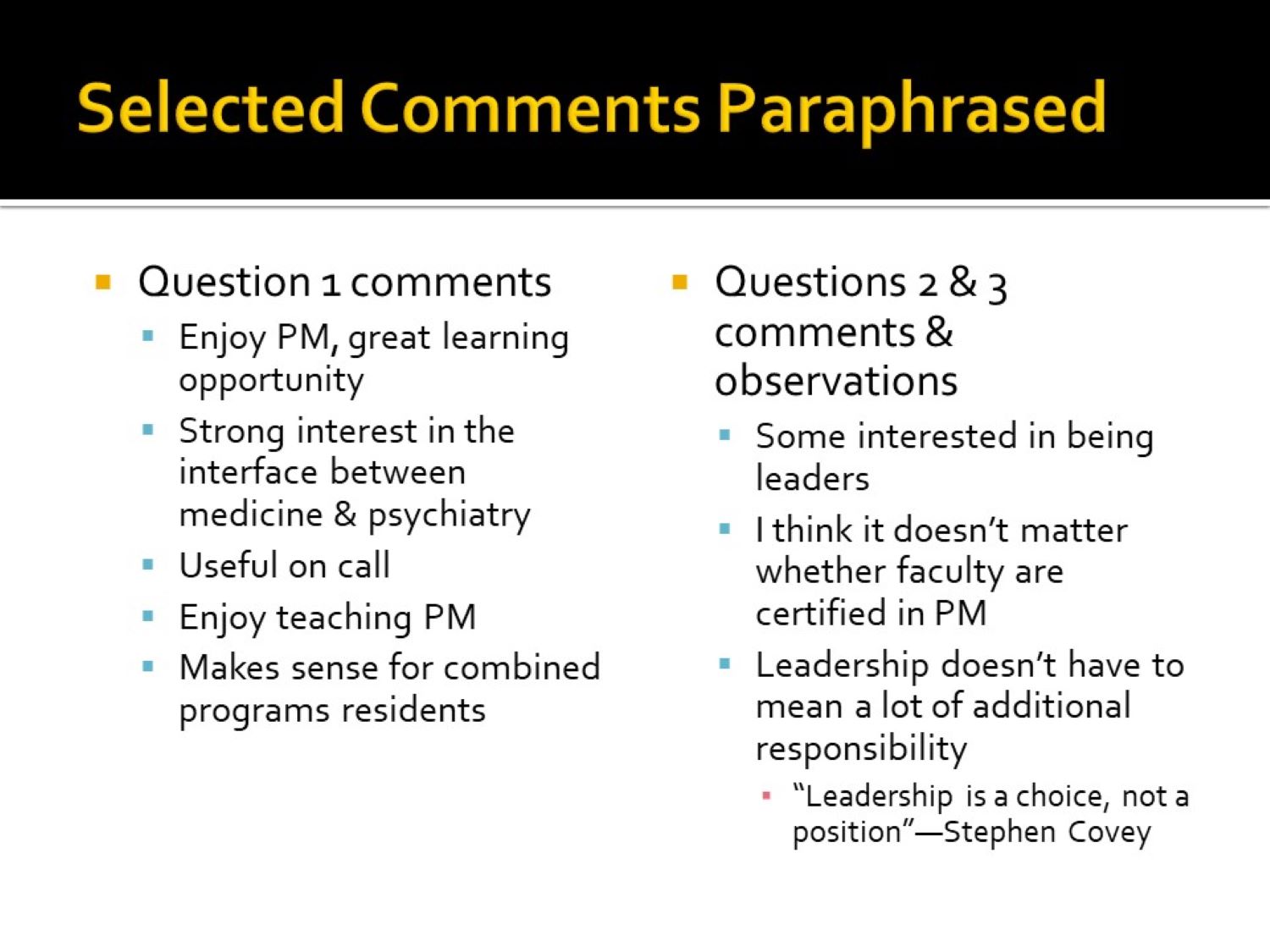

You’ll notice on slide 4 one faculty member’s comment, “I think it doesn’t matter whether faculty are certified in PM.” As Dr. Greenstein discovered, it probably does matter, at least if you want to be board certified.
I was initially certified by the American Board of Psychiatry & Neurology (ABPN), but I objected to the whole Maintenance of Certification (MOC) program, as did many other psychiatrists. I eventually declined to continue participating in the MOC process. However, I notice that the Delirium Clinical Module that I and a resident put together is still accessible on the ABPN website.
Although response numbers were low, there was clearly an interest in starting the interest group. There was also an incentive to reapply to the ACGME for approval of a Psychosomatic Medicine (Consultation-Liaison Psychiatry now) fellowship.
My attempt years earlier had been frustrating. While it was approved, I couldn’t attract any fellows, forcing me to withdraw it without prejudice (meaning another application for approval could be attempted). Fortunately, that situation changed later. The Psychiatry Department at The University of Iowa now has an early career C-L psychiatrist who graduated from the reinstated C-L fellowship.
As the saying goes, “What goes around comes around.” Although the origin of that saying might have originated in the 1970s, at least one person thought his grandmother had her own version in the 1950s: “You get what you give.”
