OK, so just heard this song “Jumpin’ Jack Rabbit” by Catfish Keith, playing on KCCK Big Mo Blues Show. I’ve looked for the lyrics and can’t find them. Anyway it was interesting, but puzzling.
I don’t know anything about guitars and never heard of Principato, but this is unreal.
We finally got a sunny break yesterday and headed out to the Terry Trueblood Trail for a walk. It was good to stretch our legs. The spring birds are back. The Tree Swallow nest boxes are installed, although one of them was upside down. I’m not sure how that happens. A sparrow chased one of the swallows off, probably staking a claim on one of the nest boxes. Lucky break for the sparrow. Lucky for all that the nest boxes were available; unlucky if some are upside down, though.
The great weather was a lucky break, actually. Rain is in the forecast for the next couple of days. Talk about luck. We both got lucky playing cribbage the other day. Sena got a double run of 2 through 5 counting the cut card—and so did I. We both got 12 points. I had the crib, and got 12 more. Neither of us can recall what we threw to my crib.
Luck is important in cribbage. An expert player, Frank Lake, once said that cribbage is 85% luck and 15% skill. Others back him up.
I got to listen to some of the presentations yesterday during the ACIP meeting on Covid-19 vaccines and boosters. My impression is that there seems to still be some discussion about what the most important goals of the vaccination program. Is it to prevent severe disease, hospitalization, and death? Or is it to prevent infection altogether?
It’s not lost on me that even mild infection with Covid-19 can lead to a chronic (“long haul”) syndrome. On the other hand, it doesn’t sound plausible that a vaccine to prevent infection would even be possible, given that so many people remain unvaccinated. That’s part of the context for the rise of variants that can lead to vaccine-resistant strains. That can lead to boosters and what some ACIP committee members are now afraid might lead to a new vogue term-“booster fatigue.”
Sena and I are now immunized as far as we can go, with 4 doses. We’re hoping for a new vaccine that is safe, effective against variants, and doesn’t involve boosting every few months.
We focus a lot on vaccines. But the other side of the risk of getting infected and sick are a part of host immunity. It gets weaker as we get older. It’s weak in those who are immunocompromised for other reasons, including things like underlying diseases and organ transplantation.
Looking at other ways to prevent disease with Covid-19, such as new medications that might counter the decline of the immune system as we age, and any other innovations are also important.
I was looking at an early version of the handbook of consultation-liaison psychiatry that eventually evolved into what was actually published by Cambridge University Press. I wrote virtually all of the early version and it was mainly for trainees rotating through the consult service. The published book had many talented contributors. I and my department chair, Dr. Robert G. Robinson, co-edited the book.
In the introduction I mention that the manual was designed for gunslingers and chess masters. The gunslingers are the general hospital psychiatric consultants who actually hiked all over the hospital putting out the psychiatric fires that are always smoldering or blazing. The main problems were delirium and neuropsychiatric syndromes that mimic primary psychiatric disorders.
The chess masters were those I admired who actually conducted research into the causes of neuropsychiatric disorders.
Admittedly the dichotomy was romanticized. I saw myself as a gunslinger, often shooting from the hip in an effort to manage confused and violent patients. Looking back on it, I probably seemed pretty unscientific.
But I can tell you that when I followed the recommendations of the scientists about how to reverse catatonia with benzodiazepines, I felt much more competent. After administering lorazepam intravenously to patients who were mute and immobile before the dose to answering questions and wondering why everyone was looking at them after the dose—it looked miraculous.
Later in my career, I usually thought the comparison to a firefighter was a better analogy.
The 2008 working manual was called the Psychosomatic Medicine Handbook for Residents at the time. This was before the name of the specialty was changed back to Consultation-Liaison Psychiatry. I wrote all of it. I’m not sure about the origin of my comment about a Psychosomatic Medicine textbook weighing 7 pounds. It might relate to the picture of several heavy textbooks on which my book sits. I might have weighed one of them.The introduction is below (featured image picture credit pixydotorg):
“In 2003 the American Board of Medical Specialties approved the subspecialty status of Psychiatry now known as Psychosomatic Medicine. Long before that, the field was known as Consultation-Liaison Psychiatry. In 2005, the first certification examination was offered by the American Board of Psychiatry and Neurology. Both I and my co-editor, Dr. Robert G. Robinson, passed that examination along with many other examinees. This important point in the history of psychiatry began many decades ago, probably in the early 19th century, when the word “psychosomatic” was first used by Johann Christian Heinroth when discussing insomnia.
Psychosomatic Medicine began as the study of psychophysiology which in some quarters led to a reductionistic theory of psychogenic causation of disease. However, the evolution of a broader conceptualization of the discipline as the study of mind and body interactions in patients who are ill and the creation of effective treatments for them probably was a parallel development. This was called Consultation-Liaison Psychiatry and was considered the practical application of the principles and discoveries of Psychosomatic Medicine. Two major organizations grew up in the early and middle parts of the 20th century that seemed to formalize the distinction (and possibly the eventual separation) between the two ideas: the American Psychosomatic Society (APS) and the Academy of Psychosomatic Medicine (APM). The name of the subspecialty finally approved in 2003 was the latter largely because of its historic roots in the origin of the interaction of mind and body paradigm.
The impression that the field was dichotomized into research and practical application was shared and lamented by many members of both organizations. At a symposium at the APM annual meeting in Tucson, AZ in 2006, it was remarked that practitioners of “…psychosomatic medicine may well be lost in thought while…C-L psychiatrists are lost in action.”
I think it is ironic how organizations that are both devoted to teaching physicians and patients how to think both/and instead of either/or about medical and psychiatric problems could have become so dichotomized themselves.
My motive for writing this book makes me think of a few quotations about psychiatry in general hospitals:
“Relegating this work entirely to specialists is futile for it is doubtful whether there will ever be a sufficient number of psychiatrists to respond to all the requests for consultations. There is, therefore, no alternative to educating other physicians in the elements of psychiatric methods.”
“All staff conferences in general hospitals should be attended by the psychiatrist so that there might be a mutual exchange of medical experience and frank discussion of those cases in which there are psychiatric problems.”
“The time should not be too long delayed when psychiatrists are required on all our medical and surgical wards and in all our general and surgical clinics.”
The first two quotes, however modern they might sound, are actually from 1929 in one of the first papers ever written about Consultation Psychiatry (now Psychosomatic Medicine), authored by George W. Henry, A.B., M.D. The third is from the mid-1930s by Helen Flanders Dunbar, M.D., in an article about the substantial role psychological factors play in the etiology and course of cardiovascular diseases, diabetes, and fractures in 600 patients. Although few hospital organizations actually practice what these physicians recommended, the recurring theme seems to be the need to improve outcomes and processes in health care by integrating medical and psychiatric delivery care systems. Further, Dr. Roger Kathol has written persuasively of the need for a sea change in the way our health care delivery and insurance systems operate so as to improve the quality of health care in this country so that it compares well with that of other nations (2).
This book is not a textbook. It is not a source for definitive, comprehensive lists of references about all the latest research. It is not a thousand pages long and does not weigh seven pounds. It is a modest contribution to the principle of both/and thinking about psyche and soma; consultants and researchers; — gunslingers and chess masters.
In this field there are chess masters and gunslingers. We need both. You need to be a gunslinger to react quickly and effectively on the wards and in the emergency room during crises. You also need to be a chess master after the smoke has cleared, to reflect on what you did, how you did it—and analyze why you did it and whether that was in accord with the best medical evidence.
This book is for the gunslinger who relies on the chess master. This book is also for the chess master—who needs to be a gunslinger.
“Strategy without tactics is the slowest route to victory. Tactics without strategy is the noise before defeat”—Sun Tzu.”
References:
1. Kathol, R.G., and Gatteau, S. 2007. Healing body and mind: a critical issue for health care reform. Westport, CT: Praeger Publishers. 190 pp.
2. Kornfeld, D., and Wharton, R. 2005. The American Psychiatric Publishing Textbook of Psychosomatic Medicine. Psychosomatics 46:95-103.
Yesterday I got the second Covid-19 booster jab. Sena got hers shortly before I did. The pharmacy was practically deserted. Nobody is waiting in line to get this one, evidently. Sena and I are now 4 for 4 jabs with no end in sight unless somebody comes up with a new vaccine that’ll last longer than a couple of months.
No pharmacy employees wore masks. I think I was the only one in the store who wore one. I’m not sure what to think of that. We’re still wearing masks out in public.
Some infectious disease specialists are recommending you get the 2nd booster if you’re over 60, even if you don’t have serious medical comorbidities.
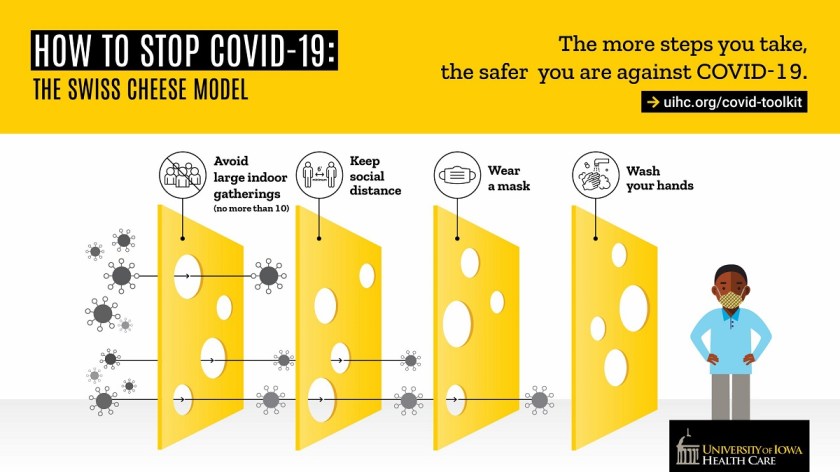
Keeping a watchful eye on transmission levels in the areas where you live is also important. Right now, it’s low in ours. But that could change, especially if we ignore the Swiss cheese method for protecting ourselves from Covid-19.
I told the little story about a postop nurse asking me a CAM-ICU question (Will a stone float on water?) after I got back to the recovery room following my retinal detachment surgery last week. I got that one right by answering “No.” But for a split second—I had to think about it.
Sena was there and remembers the nurse also asking me if I knew the day of the week. I don’t remember that question, although Sena says I got it right.
I think I was a little hazy and probably was less than fully attentive because I got some sedation during the procedure (thank goodness).
Sena found a couple of videos that challenge the notion that the answer to the question about whether or not a stone floats on water has an obvious answer. It turns out that it all depends—on what kind of rock we’re talking about and whether a scientist is answering the question.
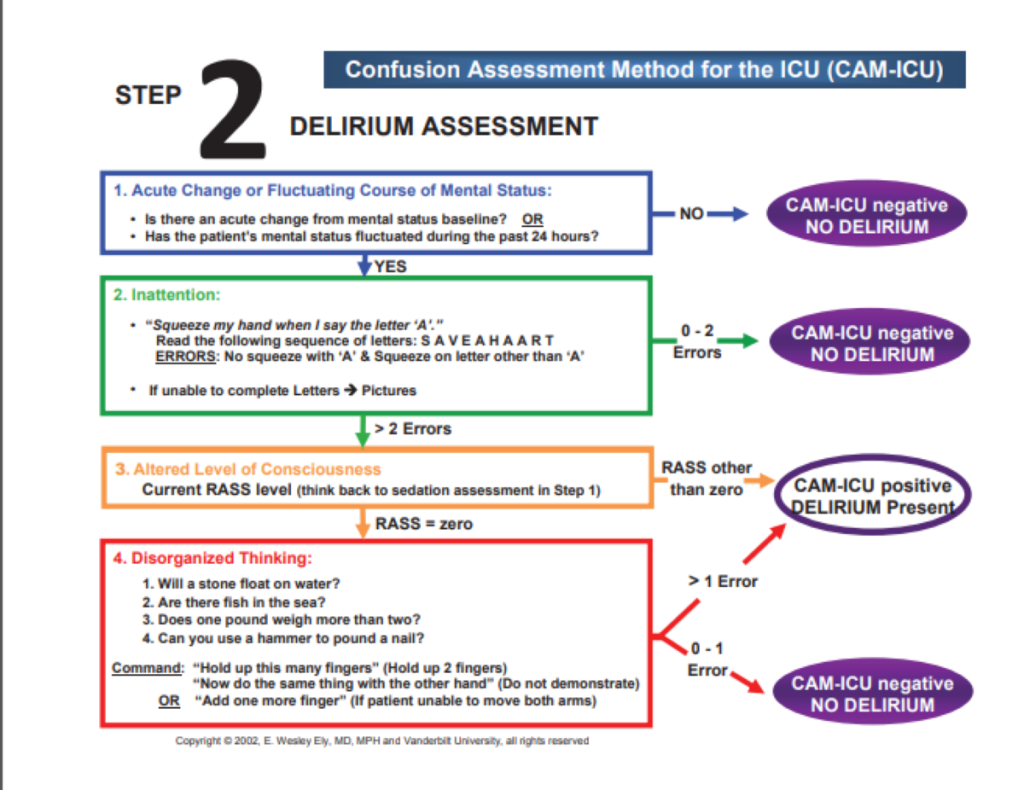
The CAM-ICU questions about thought disorganization have been outlined thoroughly, as in the picture below:
They’re in section 4: Disorganized Thinking, where you’ll see the question, “Will a stone float on water?” and others. According to the directions, you could make one “error” here and be judged not delirious.
Sena found a couple of YouTube videos that showed some rocks will, in fact, float on water. Volcanic rocks like pumice will float.
And then there are scientists like Neil deGrasse Tyson who can talk circles around you about this issue of why some kinds of rocks can float under certain conditions.
I think I was mildly delirious. But everybody took really good care of me.
To boost or not to boost? That is the question. I’m still thinking about whether or not it’s important for me to get the second booster for the COVID vaccine. What might help me decide is a little bit more information from University of Iowa Hospital epidemiologist Dr. Daniel Diekema, MD.
The Omicron subvariant, BA.2, is much more transmissible than most past variants. According to Dr. Diekema, it’s responsible for more than half of all Covid-19 cases in Iowa. On the one hand, it doesn’t cause more severe disease than the other variants, and it’s just as responsive to the current vaccines.
On the other hand, just because I’m older makes me more susceptible to severe disease and less responsive to vaccines. That’s according to studies done by Stanley Perlman. MD, PhD at the University of Iowa.
So even if the first booster dose is effective against severe COVID-19 disease, I may be better off getting the second booster sooner rather than later.
It’s also important to continue wearing a mask and practicing social distancing as well as good hand hygiene.
Here’s another oldie but goodie blog post, “It’s Survey Time.” It’s a blast from the past (May of 2011) but it needs a short introduction on why I’m reposting it.
So, I’m about a week out from my surgery for a detached retina. I’m doing pretty well. I keep thinking about a question a nurse asked me right after I was taken to the recovery room from the operating room. I was a little hazy because I’m pretty sure I got some sedation medication, although I was definitely mostly awake for the procedure. The nurse asked me, “Well, can you answer a question for me; will a stone float on water?”
First of all, I gave the right answer, “No.” More importantly, I was momentarily stunned because I recognized the question is from the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). And I told the nurse that. It reminded me of my early career as a general hospital consultation-liaison psychiatrist.
Most of my old blog posts from The Practical Psychosomaticist are about my frustration over what seemed to be my fruitless efforts to teach nurses and physicians about how to prevent, assess, and manage delirium.
I can’t tell you how happy I was that my recovery room nurse asked me a CAM-ICU delirium screening question.
I mentioned the American Delirium Society (ADS) in the post and also found a fairly recent article on the CAM ICU. Among the authors were those I met at one of t he first ADS meetings: Malaz Boustani and Babar Kahn.
“It’s Survey Time!”:
“I know, I know, I can hear it out there, “Doesn’t Dr. Amos ever learn? Nobody does surveys and polls!” Hey, that’s OK; I have so much fun doing them anyway. Of course, it would be nice to get some responses… I’ve talked to you and I’ve talked to you, and I’m done talkin’ to you! Come back here, I’m not done talkin’ to you!
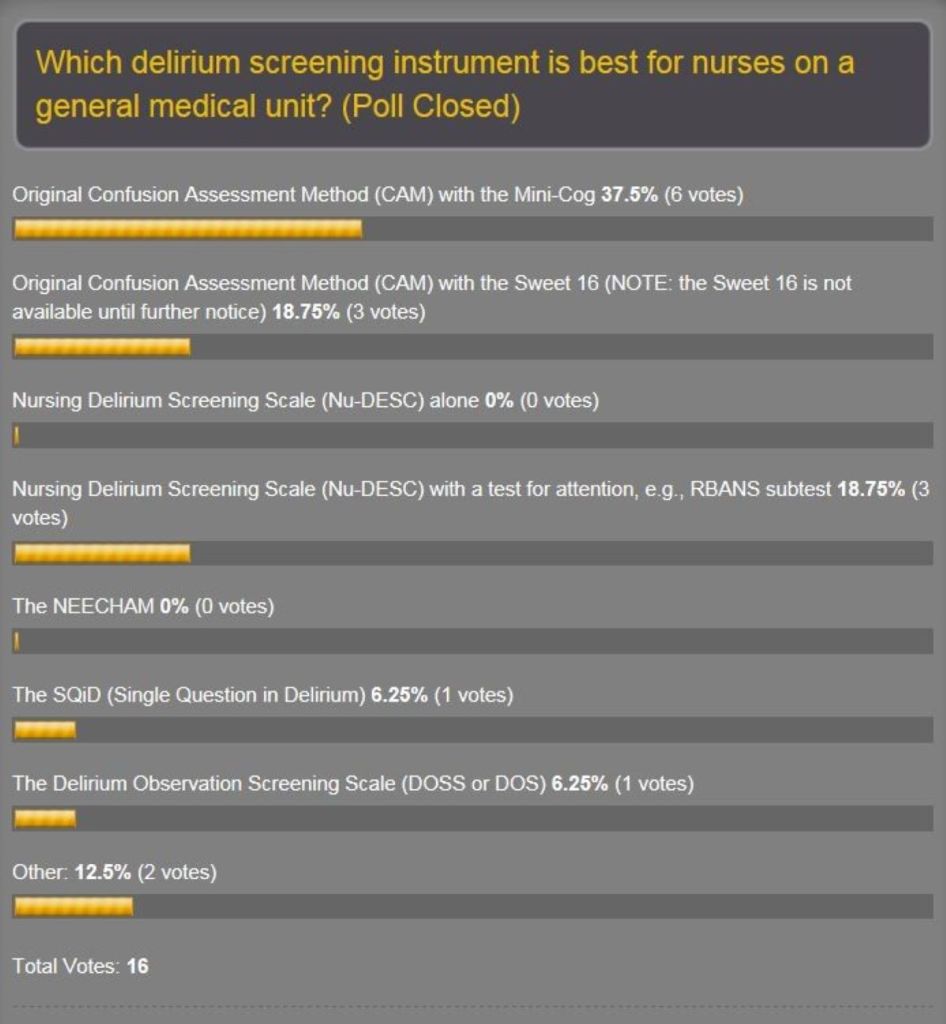
Anyway, the new poll for what’s hot and what’s not about delirium screening scales is up on the home page. The original one was partly to help our delirium prevention project committee to decide on which one to use. Well, the original got only 16 responses…but they were great responses! The amazing thing was that, despite the paucity of votes, the results were plausible. See the results:
Recall that at our 7th project meeting we selected the DOSS. What? There is good literature supporting all of these scales and a lot of factors influence selection of any tool, not the least of which is feasibility, which is mainly ease of use. That means it’s quick and doesn’t require a lot of training or additional assessments. And you should use a tool that’s validated for the patient population you want to protect from delirium. I probably got a lot of questioning looks at the screen when this poll came out because the Confusion Assessment Method-Intensive Care Unit (CAM-ICU) was not on the list. Well, you heard it from one of the main dudes on the team that developed the CAM-ICU that it’s probably not appropriate for use on general medical units…Dr. E. Wesley Ely himself (see post April 29, 2011). Hey, as far as the ICU patient population goes, the CAM-ICU is the holy grail. We need to keep looking for a sensitive and specific tool which is quick and easy for nurses to administer on general medical units.
We’re going with the DOSS. And one of my neuropsychologists, John, is offering to run neuropsychology test batteries on the patients that nurses screen with the DOSS. Atta boy, John! Neuropsychologists are going to be indispensable in this area. I remember pushing for the addition of subtests of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS), especially the Coding test in order to detect delirium early as possible. It didn’t make it, but it was close. This has been advanced by another one of our neuropsychologists here who’s done some delirium research in the bone marrow transplant unit with delirious patients. Hey, I still wonder what we could accomplish if the Coding test were added to the DOSS or even the Nursing Delirium Screening Scale (Nu-DESC). Maybe there’s already somebody out there putting a practical implementation plan for that into the real world.
So why do the poll again? Because I’d like to see if I could persuade nurses from large American and world organizations to put the nickel down and vote. And if I keep shoving this thing out there, maybe somebody will let us know that, hey, we’re not in this alone and offer to collaborate.
And I stole a couple of survey questions from our group to see what physicians and nurses think about how they manage delirium. It’s a way to take a snapshot of the culture of how docs and nurses work together on delirium recognition and interventions. And hey, why am I doing that? Because I’m a thief…no, no, I mean the reason is delirium is a medical emergency and we all need to work together to find ways to understand it better in order to prevent it. The American Delirium Society (ADS) tell you why delirium prevention is critical in the endless search to find ways to deliver high-quality medical care to patients:
Delirium Simple Facts:
More than 7 million hospitalized Americans suffer from delirium each year.
Among hospitalized patients who survived their delirium episode, the rates of persistent delirium at discharge, 1, 3 and 6 months are 45%, 33%, 26%, and 21% respectively.
More than 60% of patients with delirium are not recognized by the health care system.
Compared to hospitalized patients with no delirium and after adjusting for age, gender, race, and comorbidity, delirious patients suffer from:
Higher mortality rates at one month (14% vs. 5%), at six months (22% vs. 11%), and 23 months (38% vs. 28%);
Hospital stay is longer (21 vs. 9 days); Receive more care in long-term care setting at discharge (47% vs. 18%), at 6 months (43% vs. 8%) and at 15 months (33% vs. 11%); and
Have higher probability of developing dementia at 48 months (63% vs. 8%).
And have you registered for the ADS inaugural conference on June 5-7 in Indianapolis? Good for you! And are you going to bring back something from that conference for The Practical Psychosomaticist, and I don’t mean doughnuts? That’s the spirit! The surveys have spaces for free-text comments as well, which I want to hear!”
I heard “Oh Mary Don’t You Weep” by the Swan Silvertones for the first time earlier this evening. It kicked off ‘da Friday Night Blues with John Heim. on Jazz 88.3 KCCK. Every Friday night, Big Mo says something that sounds like, “KCCK, your blues prophylactic protecting you from the demon seeds of life.” Don’t believe me? Listen on Friday nights starting at 6:00 PM.
This song reminds me of some people I used to know.
I just found a University of Iowa Health Care announcement about a potential novel treatment to protect older patients from the ravages of Covid-19 infection. According to the announcement:
“An experimental drug that counters immune aging, effectively prevents death in older mice with severe COVID-19, suggesting it may have potential as a therapy to protect older people who are most at risk from the disease. The new findings by researchers with University of Iowa Health Care were published recently in the journal Nature.”
The experimental drug is called Asapiprant. I’m far from knowing anything much about immunology but the path to this discovery reminds me of the work of Ed Wasserman who wrote a book I’ve not yet read but probably should, As If By Design: How Creative Behaviors Really Evolve (2021, Cambridge University Press).
I first found out about Dr. Wasserman from an episode of The University of Iowa’s virtual events of Uncovering Hawkeye History. The title for this one was “Endless Innovation: An R1 Research Institution (1948–1997).” This event series was designed to highlight notable elements of UI’s 175-year history.
Anyway, in a nutshell, Wasserman’s theory is that innovation is often more about perspiration rather than inspiration. He says it’s often a combination of the 3 C’s: Context, Consequence, and Coincidence. And while I was noodling around on the web, it struck me that this might fit how the Asapiprant innovation developed.
To be sure, the University of Iowa was a critical part of the story of how Asapiprant eventually became an important agent to protect the elderly from immune system aging and thereby decrease the mortality from Covid-19 disease.
I found out the agent was originally called S-555379. It was developed by Shionogi & Co., Ltd as a possible treatment for hay fever several years ago. I think that would be the Coincidence.
But in 2011, Stanley Perlman MD, PhD, professor of microbiology and immunology in the UI Carver College of Medicine, published a paper, which I think is part of the Context:
Zhao J, Zhao J, Legge K, Perlman S. Age-related increases in PGD(2) expression impair respiratory DC migration, resulting in diminished T cell responses upon respiratory virus infection in mice. J Clin Invest. 2011 Dec;121(12):4921-30. doi: 10.1172/JCI59777. Epub 2011 Nov 21. PMID: 22105170; PMCID: PMC3226008.
This paper was cited by Shionogi in the company’s announcement of their license agreement with BioAge Labs, Inc., posted on January 26, 2021:
“It is known that age-related declines in immune function are significant risk factors that increase morbidity and mortality from infectious diseases2. Therefore, it has been suggested that restoring immune function may reduce the severity of various infectious diseases, including COVID-19. The DP1 receptor has been identified as a drug discovery target that improves age-related declines in immune function in an original AI-driven analysis of longitudinal omics data in humans conducted by BioAge. In addition, in a study conducted at the University of Iowa by Dr. Stanley Perlman in which an existing DP1 receptor antagonist was administered in an aged mouse model of SARS coronavirus (SARS-CoV) infection, the mortality rate of mice was improved and a significant decrease in viral load in the lungs was observed3. Based on these exciting study results, we have concluded a license agreement in expectation of development of this compound as an immunopotentiator for the elderly by drug repositioning.”
And I think part of the Consequence is that BioAge, Inc. has announced that the drug, the name of which was changed to BGE-175 and now called Asapiprant is about to undergo Phase 2 clinical trials for treating older patients hospitalized with COVID-19.
Whether you call it perspiration or inspiration, I think it deserves our admiration.