This just in! University of Iowa Psychiatrist Dr. Susan Shen, MD, PhD, is an assistant professor of psychiatry at The University of Iowa Carver College of Medicine and, hold on to your hat, she’s the first female psychiatrist, the first from Iowa, and only the third psychiatrist overall to receive to win the Avenir Award (French for “future), a highly competitive grant!
The $2.3 million dollar grant will help fund her lab’s research into the underpinnings of substance use and psychiatric disorders. The grant is administered through the National Institute on Drug Abuse (NIDA), one of the National Institutes of Health (NIH).
How about some good news? This just in, University of Iowa Physician-Scientist, Dr. Michael Welsh, wins the 2025 Lasker Award for his research on cystic fibrosis.
His work and the work of two other researchers with whom he’ll share the award set the stage for the development of new drugs which saves the lives of those who suffer from cystic fibrosis.
I learned from the article that the cystic fibrosis gene was discovered in 1989; I was a second-year medical student then. Since then, the development of new treatments has meant that many people who died in early adulthood now can live into their 80s.
There’s a new podcast in town from The University of Iowa Health Care and the title is “When to Suspect Atypical Recreational Substances.”
This is a fascinating topic and the discussion ran for close to an hour, which is longer than usual because there’s a lot to say about it. The substances include a lot of chemicals that are not illegal and, in some cases, easily available in convenience stores and gas stations. In fact, the name for one of them is gas station heroin, which is tianeptine, approved in other countries as an antidepressant.
The discussion also included substantial information (or maybe better said, lack of enough information) about bath salts (usually cathinones), kratom, and something I’ve never even heard of: diamond shruumz (chocolate bars which can contain various substances not limited to psilocin). Remember that guy who chewed the face off of somebody in Miami in 2012? That was attributed to intoxication with bath salts.
This is way beyond the 1970s stuff like window pane or blotter (LSD) and pot. Many people end up in emergency rooms for evaluation of what looks like poisoning from multiple drugs. The stickler is the possibility that they got poisoned from something bought at a convenience store. Often it’s difficult to tell what the person ingested.
One of the takeaways from this podcast is that, whenever possible, try to get a history from the patient. They might just tell you what you need to know.
I’ve been looking for other ways that Iowa addresses mental illness and its impact on homelessness and other adverse outcomes since my last post on the issue.
It turns out that, despite Iowa ranking 51st out of all U.S. states for the low number of psychiatric beds according to the Treatment Advocacy Center statistics (in 2023, it had just two beds per 100,000 patients in need), a new mental health court established in in May of 2023 has made substantial progress in reducing the number of crisis contacts, psychiatric hospitalizations, and days in the hospital. Arrests, jailings, and days in jail were also reduced.
Participants in the new program include the University of Iowa Health Care, Iowa City VA Hospital, the Abbe Center, Guidelink Center, National Alliance for the Mentally Ill (NAMI), Shelter House, and several other mental health service agencies in Johnson County.
The Johnson Mental Health Court continues to operate since June of this year when the pilot program’s funding from the East Central Iowa Mental Health Region was supposed to have ended on June 30, 2025, due to the change in mental health regions. This is a program for patients under involuntary mental health commitment that avoids incarceration and placement in a state psychiatric hospital.
This civil mental health program didn’t exist until well after I retired and I hope for its continued success.
I listened to the Rounding@Iowa podcast “End-of-Life Doulas” twice because I’m at that difficult age when I think about my personal death. I don’t think about it at great length, mind you, but when I think about it, I feel afraid. Early mornings tend to be the time I wonder how much time now until…?
There was the usual podcast format, Dr. Gerry Clancy interviews Mary Kay Kusner, who is certified death doula to get the overview and details about what death doulas are all about.
I listened to the podcast in the late afternoon and discussed it only briefly with Sena. I felt out of sorts for a few hours afterward. I was in a funk until later in the evening when my thoughts almost abruptly switched to something funny. It was about a topic I’m thinking of for another blog post which has a humorous angle to it. I even chuckled a little out loud. I didn’t force that line of thought—it just happened.
But I know why it happened.
I didn’t know what a doula was until I listened to the podcast. Because I’m a writer by inclination, I looked for the original definition, which is a female servant who helps women with birthing. That didn’t enlighten me much, obviously; I can’t remember the last time I was pregnant (see what I did there?). An end of life-or-death doula helps people come to terms with impending death, death when it happens, and with whatever comes up after death has happened.
The title of this post comes from the Mary Kay Kusner’s short anecdote near the end of the podcast. Early in her career as a chaplain, she met with a 4-year-old child in the oncology unit who had a terminal illness, evidently death was coming and asked her, “How will I get to heaven?” They talked about it and the next thing the child said was, “So it’s like another dimension?” which Kusner evidently validated in some way. It’s a really cute story.
Anyway, there was a thread running through the podcast which pointed to what is apparently an ongoing psychological disconnect medical professionals have about death because we’re so focused on cure. It’s disappointing, but there you go. Death doulas are around to fill the role of talking calmly and matter-of-factly about it with patients and families.
There are some nuts and bolts about the profession, some of which I get and others which I scratch my head about. There are a couple of doula organizations in Iowa City which Kusner mentions: Community Death Doulas and Death Collective Eastern Iowa. Mary Kay Kusner is certified as a death doula via online training through INELDA.
Interestingly some people do not believe that this is a profession which can be certified, at least without some practical clinical experience. There’s a web site in which the question-and-answer section is longer than the article itself about this. The author recommends specific courses.
Death doulas are not covered by health insurance, so the practitioners arrange for payment, often through a sliding scale hourly fee. Part of the reason for the training of and demand for death doulas is that hospice nurses have heavy caseloads.
This reminds me of the hospice where my younger brother died after his battle with cancer. He was in his forties. Before he entered hospice, I had to be one of his doctors on the medical psychiatry inpatient unit after he accidentally overdosed on his pain medication.
When my brother was in hospice, I sat at his bedside. Most of the time, he was delirious. I watched and listened as one of the hospice workers as he asked him whether he was entering the dying process. He used those words. My brother was just as delirious as he was when he had to be admitted to the medical-psychiatry unit. I don’t know how much he heard.
I sat at his bedside, determined to hold some kind of death watch vigil. This was interrupted, ironically, by some friends of his who visited. They stood opposite the bed so that I had to look at them instead—and to listen as they told me stories about how close they’d been to him and how much they loved him.
By the time they were finished and I turned back to my brother, he was gone. It took me a little while to figure out I had not missed anything I really needed.
So, I think death doulas could be vital in building a bridge between those who are dying and those who need to connect with them. That’s the main thing.
Today is designated Earth Day although there is such a thing as Earth Month. Among the several trees Sena planted in our back yard trees are a few that we hope exemplify the Earth Day theme, which is Our Power, Our Planet.
One of them is a dogwood, which we’re hoping will bloom soon. Dogwoods represent joy and rebirth. There are a couple of crab apple trees, a red jewel and a perfect purple. Crab apple trees represent love and all are very special to Sena and me.
Love, joy, and rebirth. They can all be linked to power, which can be the power of will. The will to respect the planet also implies respecting each other. Practicing humility can be a kind of power.
The power to be still and listen to each other can make us more open to change.
On that note, because I can’t go for long without joking around, I should retell the story about me and the walking dead meditation. About 13 years ago, I had an even more serious case of not listening to others than I do now, if you can believe that. It eventually led to my choosing to take the Mindfulness Based Stress Reduction (MBSR) class ( see this current University of Iowa mindfulness essay). I wrote an essay for the Gold Foundation and it’s still available (I updated the links):
How I left the walking dead for the walking dead meditation (August 13, 2014)
About a year or so later, I bought Jon Kabat-Zinn’s book on Mindfulness-Based Stress Reduction (MBSR), Full Catastrophe Living, because I was dimly aware of the burden of stress weighing on me as a consulting psychiatrist in an academic medical center. I didn’t get much out of Kabat-Zinn’s book on my first read. But then in 2012 I started getting feedback from colleagues and trainees indicating they noticed I was edgy, even angry, and it was time for a change.
Until then, I’d barely noticed the problem. Like most physicians, I had driven on autopilot from medical school onward. I had called myself “passionate” and “direct.” I had argued there were plenty of problems with the “system” that would frustrate any doctor. I had thought to myself that something had to change, but I never thought it was me.
After reflecting on the feedback from my colleagues and students, I enrolled in our university’s 8 week group MBSRprogram. Our teacher debunked myths about mindfulness, one of which is that it involves tuning out stress by relaxing. In reality, mindfulness actually entails tuning in to what hurts as well as what soothes. I was glad to learn that mindfulness is not about passivity.
But I kept thinking of Kabat-Zinn’s book, in which he described a form of meditation called “crazy walking.” It involved class members all walking very quickly, sometimes with their eyes closed, even backwards, and crashing into each other like billiard balls. I hoped our instructor would not make me “crazy walk” because it sounded so—crazy. I dreaded crazy walking so intensely that I considered not attending the 6-hour retreat where it might occur.
We didn’t do crazy walking. Instead, we did what’s called the “walking meditation.” Imagine a very slow and deliberate gait, paying minute attention to each footfall—so much so that we were often off balance, close to crashing into each other like billiard balls.
I prefer to call this exercise the “walking dead meditation” because it bore a strong resemblance to the way zombies move. One member of the class mentioned it when we were finally permitted to speak (except for the last 20 minutes or so, the retreat had to be conducted in utter silence). It turned out we had all noticed the same thing!
Before MBSR, I was like the walking dead. I was on autopilot — going through the motions, resisting inevitable frustrations, avoiding unstoppable feelings, always lost in the story of injustices perpetrated by others and the health care system.
In practicing mindfulness, I began noticing when my brow and my gut were knotted, and why. Just paying attention helped me change from simply reacting to pressures to responding more skillfully, including the systems challenges which contribute to burnout. About halfway through the program, I noticed that the metaphor connecting flexibility in floor yoga to flexibility in solving real life problems worked.
Others noticed the change in me. My professional and personal relationships became less strained. My students learned from my un-mindfulness as well as my mindfulness, a contrast that would not have existed without MBSR.
As my instructor had forewarned, it was easy for me to say I didn’t have time to practice meditation. I had to make the time for it, and I value the practice so much that I’ll keep on making the time. I will probably never again do the walking dead meditation.
Today we gather to reward a sort of irony. We reward this quality of humanism by giving special recognition to those who might wonder why we make this special effort. Those we honor in this fashion are often abashed and puzzled. They often don’t appear to be making any special effort at being compassionate, respectful, honest, and empathic. And rewards in society are frequently reserved for those who appear to be intensely competitive, even driven.
There is an irony inherent in giving special recognition to those who are not seeking self-aggrandizement. For these, altruism is its own reward. This is often learned only after many years—but our honorees are young. They learned the reward of giving, of service, of sacrifice. The irony is that after one has given up the self in order to give back to others (family, patients, society), after all the ultimate reward—some duty for one to accept thanks in a tangible way remains.
One may ask, why do this? One answer might be that we water what we want to grow. We say to the honorees that we know that what we cherish and respect here today—was not natural for you. You are always giving up something to gain and regain this measure of equanimity, altruism, trust. You mourn the loss privately and no one can deny that to grieve is to suffer.
But what others see is how well you choose.
Leonard Tow awardGetting the pinOn my lapel; in my heart
I’m still practicing mindfulness-more or less. Nobody’s perfect. We hope the dogwood tree blooms soon.
Okay, so here’s my pitch on how potential donors can support programs at The University of Iowa. Today the One Day for Iowa fund drive kicks off, and it ends at 11:59 PM today on March 26, 2025.
I got a soft spot in my heart for The University of Iowa College of Medicine and University of Iowa Health Care (UIHC), even though my undergraduate Bachelor’s degree was from Iowa State University.
You can find in the UIHC Medical Museum a description of the historical development of the medical school. Following the Flexner Report in 1909 which found fault with all U.S. medical schools including Iowa’s, there was a drive to avoid “inbreeding,” meaning hiring of one’s own graduates. Nowadays, there are legislative efforts to keep as many as we can of Iowa’s best and brightest.
I had my regular visit to the dentist at The University of Iowa Health Care (UIHC) today, and it was a good thing I did. For the past couple of weeks or so I’ve had cold and hot sensitivity in a couple of teeth. No surprise, the dentist found 3 teeth that needed a little work.
The dental hygienist also suggested I try using a tongue cleaner and gave me a free one. I’d never heard of a tongue cleaner before. The package advertisement (in English, French, and Spanish) says it’s for combatting bad breath, although the dental hygienist assured me in 6 different languages that she didn’t detect that problem in me.
I was there for my annual teeth cleaning but now I had 3 teeth needing work. Luckily, the dentist had an appointment in the early afternoon. It was a 3 hour wait, but I thought it was better to get it done sooner rather than later. Anticipating a visit with a dentist is sometimes almost as bad as getting in the chair and exercising my ability to refrain from flinching as the high-speed instruments whine in my ear while the dentist and the assistant do their level best to see that I gag several times in at least 9 different languages, including Klingon.
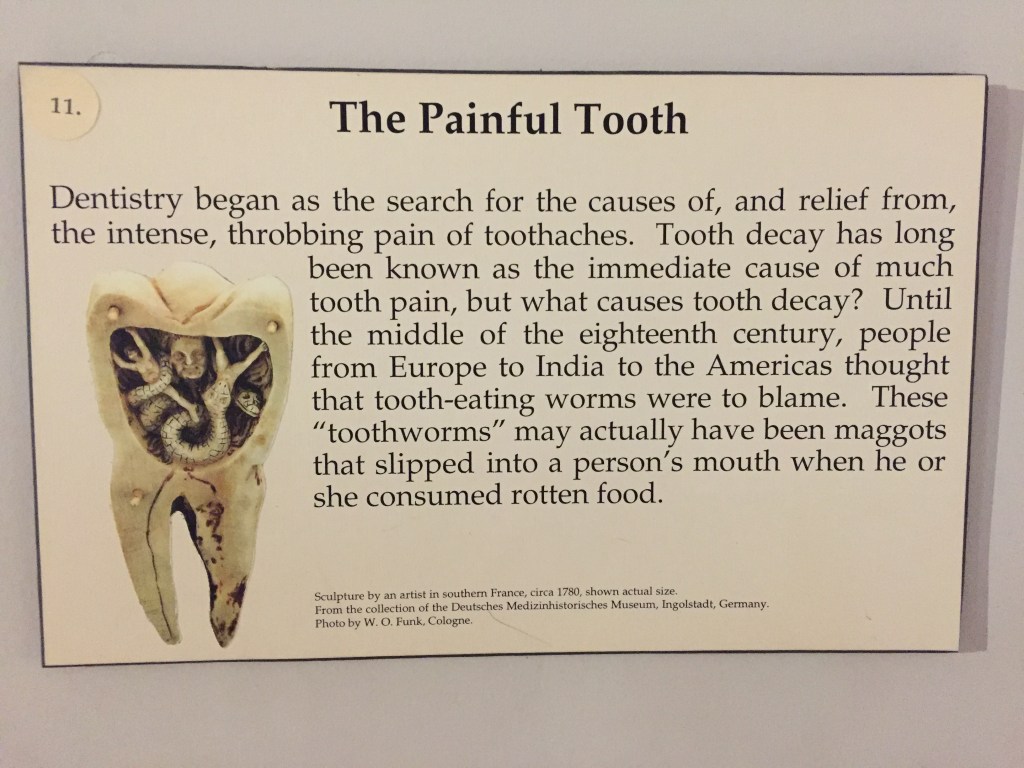
It’s hard to explain why I was having tooth sensitivity because, according to the dentist, the damage was not that severe. It wasn’t until I wandered around the hospital while waiting for the 2nd appointment that I realized I had never visited the Medical Museum on the 8th floor. And that’s where I found a possible explanation that made more sense than the modern one. It’s probably toothworms.
No kidding, back in the 18th century, a lot of people thought worms caused tooth decay by eating them from the inside out. There was also a College of Dentistry display in the Medical Museum featuring a typical dentist chair and samples of rusty tools, which made wonder if I should put off the filling work until, say, after my next ten reincarnations.
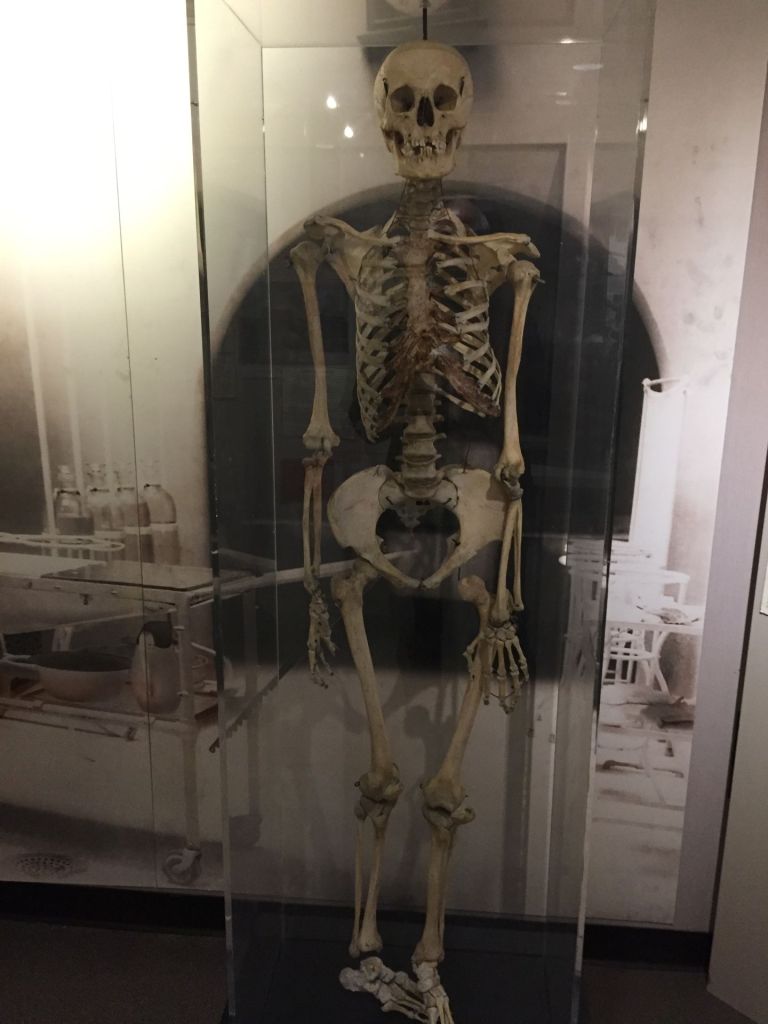
There’s a human skeleton in the museum which is affectionately called Gertie. The historical note on Gertie is very interesting in that it was thought to be a male when Ottumwa Regional Health Center donated it to UIHC in 2013. It turns out he is actually a she and the “…two symmetrical holes in the upper jaw are the result of large dental abscesses.” Just what I wanted to learn on a day when I’m anticipating dental work.
Anyway, my teeth got repaired. I would say that the UIHC dental clinic has come a long way from 1904. You don’t turn and spit in a bowl anymore. They just siphon the toothworms out with a suction wand nowadays.
This episode of Rounding@Iowa is about important medical advances in the treatment of pancreatic cancer. As you listen to Dr. Clancy interview Dr. Joseph Cullen about what’s new, you’ll hear a lot about high-dose intravenous Vitamin C. This can enhance treatment and improve response to chemotherapy and radiation therapy. Dr. Cullen’s most recent study about this technique showed the overall survival of patients with late-stage pancreatic cancer increased from 8 months to 16 months.
Reference:
Kellie L. Bodeker, Brian J. Smith, Daniel J. Berg, Chandrikha Chandrasekharan, Saima Sharif, Naomi Fei, Sandy Vollstedt, Heather Brown, Meghan Chandler, Amanda Lorack, Stacy McMichael, Jared Wulfekuhle, Brett A. Wagner, Garry R. Buettner, Bryan G. Allen, Joseph M. Caster, Barbara Dion, Mandana Kamgar, John M. Buatti, Joseph J. Cullen,
A randomized trial of pharmacological ascorbate, gemcitabine, and nab-paclitaxel for metastatic pancreatic cancer,
Patients with metastatic pancreatic ductal adenocarcinoma (PDAC) have poor 5-year survival. Pharmacological ascorbate (P-AscH-, high dose, intravenous, vitamin C) has shown promise as an adjunct to chemotherapy. We hypothesized adding P-AscH- to gemcitabine and nab-paclitaxel would increase survival in patients with metastatic PDAC.
Methods
Patients diagnosed with stage IV pancreatic cancer randomized 1:1 to gemcitabine and nab-paclitaxel only (SOC, control) or to SOC with concomitant P-AscH−, 75 g three times weekly (ASC, investigational). The primary outcome was overall survival with secondary objectives of determining progression-free survival and adverse event incidence. Quality of life and patient reported outcomes for common oncologic symptoms were captured as an exploratory objective. Thirty-six participants were randomized; of this 34 received their assigned study treatment. All analyses were based on data frozen on December 11, 2023.
Results
Intravenous P-AscH- increased serum ascorbate levels from micromolar to millimolar levels. P-AscH- added to the gemcitabine + nab-paclitaxel (ASC) increased overall survival to 16 months compared to 8.3 months with gemcitabine + nab-paclitaxel (SOC) (HR = 0.46; 90 % CI 0.23, 0.92; p = 0.030). Median progression free survival was 6.2 (ASC) vs. 3.9 months (SOC) (HR = 0.43; 90 % CI 0.20, 0.92; p = 0.029). Adding P-AscH- did not negatively impact quality of life or increase the frequency or severity of adverse events.
Conclusions
P-AscH− infusions of 75 g three times weekly in patients with metastatic pancreatic cancer prolongs overall and progression free survival without detriment to quality of life or added toxicity (ClinicalTrials.gov number NCT02905578).
Dr. Cullen mentions that patients contact him not infrequently to ask if taking high-dose oral Vitamin C will help them achieve similar results. Unfortunately, it will not. Giving it intravenously facilitates giving much higher doses. The study had a relatively small number of participants, which limited ascertainment of quality of life.
On the psychological side, there are ways to bolster the mental health challenges of those with pancreatic cancer, which typically has a grim outcome in terms of survival:
Spiegel D. Mind matters in cancer survival. Psychooncology. 2012 Jun;21(6):588-93. doi: 10.1002/pon.3067. Epub 2012 Mar 21. PMID: 22438289; PMCID: PMC3370072.
Further, Dr. William Breitbart, MD, Chair of the Department of Psychiatry and Behavioral Sciences at Memorial Sloan Kettering Cancer Center was interviewed in 2021 and emphasized the need for bolstering mental health for those diagnosed with pancreatic cancer. According to Breitbart, “Pancreatic cancer triggers an inflammatory response in the body, which can lead to mood disorders,” Breitbart explains. Psychiatrists can prescribe certain antidepressant medications that directly target that inflammatory response.”
I listened to the Rounding@Iowa podcast of February 11, 2025, “Challenges in Transitioning Seriously Ill Patients from Pediatric to Adult Systems of Care.”
Join Dr. Clancy, Dr. Appenheimer & Dr. Barker as they discuss prevention, diagnosis and treatment of various tick-borne illnesses. CME Credit Available: https://uiowa.cloud-cme.com/course/courseoverview?eid=82296 Host: Gerard Clancy, MD Senior Associate Dean for External Affairs Professor of Psychiatry and Emergency Medicine University of Iowa Carver College of Medicine Guests: Ben Appenheimer, MD Clinical Associate Professor of Internal Medicine-Infectious Diseases Assistant Director, Infectious Diseases Fellowship Program Associate Clinical Director, Infectious Diseases Co-Medical Director, TelePrEP, University of Iowa Health Care University of Iowa Carver College of Medicine Jason Barker, MD Associate Professor of Internal Medicine-Infectious Diseases University of Iowa Carver College of Medicine Financial Disclosures: Dr. Gerard Clancy, his guests, and Rounding@IOWA planning committee members have disclosed no relevant financial relationships. Nurse: The University of Iowa Roy J. and Lucille A. Carver College of Medicine designates this activity for a maximum of 1.0 ANCC contact hour. Pharmacist and Pharmacy Tech: The University of Iowa Roy J. and Lucille A. Carver College of Medicine designates this knowledge-based activity for a maximum of 1.0 ACPE contact hours. Credit will be uploaded to the NABP CPE Monitor within 60 days after the activity completion. Pharmacists must provide their NABP ID and DOB (MMDD) to receive credit. JA0000310-0000-26-038-H01 Physician: The University of Iowa Roy J. and Lucille A. Carver College of Medicine designates this enduring material for a maximum of 1.0 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Other Health Care Providers: A certificate of completion will be available after successful completion of the course. (It is the responsibility of licensees to determine if this continuing education activity meets the requirements of their professional licensure board.)
This was a very interesting presentation about the challenges of helping persons with life-limiting conditions (for example, hemophilia, cystic fibrosis, sickle cell anemia and more) transition from pediatric to adult systems of care. Most of the discussion was about the difficulty in finding doctors who would be willing and able to assume care of patients who had survived to adulthood who had been previously seen in pediatrics throughout childhood.
I listened very carefully to the whole podcast, waiting to hear about what the role of mental health care professionals would be in this kind of transition. There was no mention of it, not even after one of the presenters described a patient who was starting to have hallucinations.
My role as a consulting psychiatrist in a general hospital was mainly to see those with chronic diseases who were being treated by colleagues during a bout of cystic fibrosis or sickle cell crisis. I remember they were young adults, struggling with emotional distress and disruptive behavior.
I was surprised at the lack of discussion about the role of mental health assessments, diagnoses, and treatment including psychotherapy during transitions from pediatric to adult health care. Not that I would have had much to offer other than questions about how mental health professionals could be helpful regarding transitions—but I think they would have not been out of place.
I took a quick look at the resources provided. One of them was a University of Iowa website, the Iowa Center for Disabilities and Development: Transition to Adulthood Clinic For Teens and Young Adult Ages 14-30. Even here, the role of a psychologist was to evaluate learning problems.
One of the discussants mentioned a program called Got Transition, which has a very comprehensive website. There was a section for Special Populations and a list of resources and research when I searched the site using the term “mental health.” It was hard to find a section specific to the population under discussion in the podcast. On the other hand, it was very comprehensive.
In this podcast, discussants talked about the importance of a team approach to transitions. I wonder if there’s a place on the team for psychiatry.