I just got Wes Ely’s new book, Every Deep-Drawn Breath. You do need to buy this book to learn about delirium, Post-Intensive Care Syndrome (PICS) and what Dr. Ely and colleagues are doing to prevent it. PICS is a syndrome patients suffer after being hospitalized with severe medical illness in critical care units. It includes impairments in cognitive skills (impaired executive functioning), emotional functioning (depression, anxiety, post-traumatic stress disorder), and physical function (weakness, myopathy, and neuropathy).
Reading the prologue and first chapter reminded me of my early years in medical school and residency. It also reminded me of my frustrations when I was working as a psychiatric consultant trying to teach my colleagues about delirium, which a large percentage of patients suffer in the intensive care unit (ICU). I retired a little over a year ago.
Dr. Ely’s book also reminded me that I wrote an article about delirium 10 years ago, which was published in Psychiatric Times. I can still find it on line. The title is “Psychiatrists Can Help Prevent Delirium.” Prevention is the key because once delirium sets in, the challenge to offset the neurocognitive impairment becomes far greater.
A couple of years before I wrote it, I had tried working in private practice in Wisconsin. Aside from gaining weight from the good food there, I didn’t adjust well and quickly returned to Iowa City. I did make a consultation visit to a primary care clinic where I worked, which was a welcome surprised to the clinician who asked for help. You can take the psychiatric consultant out of the hospital, but you can’t take the hospital out of the psychiatric consultant.
I also met Dr. Ely around that time as well, because I kidded him about what he wrote in another book, Delirium in Critical Care (2011). There was a couple of paragraphs in a section called “Psychiatrists and delirium.” I’m going to risk somebody rapping my knuckles about copyright rules, but I’ll quote the sentence that usually made me chuckle: “Should we, or should we not, call the psychiatrist? Can we replace them with a screening tool and then use haloperidol freely?”
I think that was meant to be funny—and it was in an ironic way. Every psychiatric consultant knows that the main treatment for delirium is not haloperidol, but treating the underlying medical illnesses. Anyway, I poked a little fun at that book section in a blog post (which I no longer have, called “The Practical Psychosomaticist”) and shortly thereafter, he emailed me, asking me to write a few posts highlighting the serious and important research he and others were conducting about delirium. I learned a lot.
Eventually, I actually met Dr. Ely, at meeting of the American Delirium Society in Indianapolis. I respect and admire him. He’s a brilliant doctor and a caring man. And you should buy his book.
This is just an update on the Pfizer-BioNTech COVID-19 vaccine Comirnaty vs Comiranty spelling issue at UIHC, which has been resolved today. It took a few emails to get it fixed. I was beginning to think I was losing my mind and that I was the only who could see the mistake. Comirnaty had apparently been misspelled as Comiranty on several web pages for maybe a couple of weeks.
You can just look at the word Comirnaty and see how this could have happened. Looking at it in print makes me think there are two letter “m’s” in it. Transposing the two letters “a” and “n” looks easy to do. There are a few anagrams web sites that are picking up on the word Comirnaty. I kind of like “try anomic.” Can you really get “community,” “immunity,” and “mRNA” out of that agglomeration? Maybe. It’s a name game.
I could chalk this up to just me being a retired guy with too much time on his hands and nitpicking. On the other hand, there is that story about a typo ending World War II. In all fairness, there is some doubt about the accuracy of it. But it’s fascinating to think that the difference in spelling between cryptogamist (someone who studies algae) and cryptogramist (someone who studies codebreaking) might have made all the difference in the war’s outcome.
When I think about all the mandates and bans against mandates for the COVID-19 vaccines and masks, I wonder about my own motive for getting the vaccine and wearing a mask.
In one sense, I’m doing it for myself. I’m a retired consultation-liaison psychiatrist and I got called to the intensive care units a lot. Almost always, the patient was delirious. And almost always, the patient was delirious in the setting of being on the ventilator or in the process of being liberated from the ventilator.
The critical care physician and the nurses were always looking for one specific thing from me. I was supposed to stop the patient from being agitated, to calm the wildly thrashing, terrified person fighting the restraints and struggling with hallucinations and fragmented paranoid delusions that every caregiver in the unit was trying to kill him. Often there were many medical problems, including multiple organ failure often from lack of oxygen, resulting in brain injury as well. Nowadays, COVID-19 is a frequent cause of delirium for the same reasons.
Years ago, the only tool I had was an antipsychotic called haloperidol, because it could be given intravenously. It would calm some patients, but it could and did cause side effects including akathisia (extreme restlessness), dystonia (severe muscle spasms), and neuroleptic malignant syndrome NMS, a rare, complex, life-threatening neurologic emergency attributable to antipsychotics. Over the past several years, the ICU pharmacies acquired newer drugs like dexmedetomidine, which is not a psychiatric drug. That didn’t stop the ICU from calling me.
I’ve seen all of that. I got the vaccine and wear the mask mostly because I don’t want to be in that boat. But I think those measures help protect others, too. I think many people have that motive. Those who think they’re getting it just for themselves can go on thinking that.
We’re taking a risk when we get the vaccine. It’s not completely harmless. There are very rare side effects which can be life-threatening and they have killed people. There is some level of altruism involved. Those who get the vaccine are playing a role, however small, in reducing the chance the virus will mutate into something that will kill even more people.
Wearing masks is a nuisance and doesn’t really feel heroic. But this act combined with other measures (the usual suspects: hand-washing, social distancing, avoiding large crowds) spreads love instead of infection.
We don’t have to agree. We don’t have to love each other. I just hope we can respect each other.
Occasionally I’ll reminisce, an activity which recently got triggered when I realized why I tend to like watching TV shows like Highway Thru Hell and Heavy Rescue 401, which are heading into the 10th and 6th seasons, respectively. Despite that, last year I didn’t see any episodes in which the COVID-19 pandemic was even mentioned. Nobody wears masks. They’re hard-working people in Canada who basically drag semi-trucks out of various ditches. It’s hard work, they’re down-to-earth and they’re not acting.
I marvel at what they do. It’s brutal, real, and no-nonsense. While I watch them, I tend to forget about the pandemic, and the social and economic upheaval everywhere on the planet. For a little while, I almost stop thinking about bored I am and without a purpose or meaning sometimes in retirement. I just find myself being glad I don’t have their job.
Sometimes I think about how I got my start as a working stiff, starting out as a teenager doing practical work like the heavy tow truck drivers. Now, don’t get me wrong. I’m not trying to sell you the idea that land surveying is really hard work. I was outside most of the time, although in the winter when highway, street, and other construction was down, I would do some drafting. I worked for WHKS & Co. If you click the link to their website, scroll all the way down on the About Us section. There’s a black and white picture with four frowning men sitting at a heavy desk in front of a bookcase with many large books in it. They are from left to right, Richard “Dick” Kastler, Francis Holland, Ralph Wallace, and Frank Schmitz. I didn’t know Richard but his brother, Carol Kastler, was my boss along with the other three. Carol Kastler was the head of the land surveying department.
This is not going to be a history of surveying, which I’m not qualified to do; just my impressions of it as a young man. I can flesh it out a little with a video about how to throw a chain, and an extremely detailed reminiscence written by a real old-timer about surveying that was a lot like the way I remember it. Try to read all of Knud E. Hermansen’s first essay about measuring with a steel tape, “Reminisce Of An Old Surveyor, Part I: Measuring a Distance by Taping.” You can skip Part II, which even I couldn’t relate to because the stuff was way before my time.
Hermansen’s description of measuring distance using a steel tape and plumb bob is spot on, though. The other thing I would do in the winter down time was tie up red heads—which is not what you’re thinking. You tied red flagging around nails which were used to mark distances measured.
We often did work out in the field through the winter, though. When we set survey corners using what were called survey pins. Sometimes we had to break through the frozen ground first by pounding a frost pin with a sledge hammer. I remember WHKS & Co. made their own cornerstones using a wood frame box and cement. They were several feet long and they were heavy and surveyors carried them slung to their backs through the timber.
We spent a lot of cold days on straightening out a lot of the curves in Highway 13 between Strawberry Point and Elkader in eastern Iowa. We had expense accounts and were often away from our homes a week at a time for most of the winter. We ate a lot of restaurant food. Carol Kastler was partial to pea salad.
Guys told colorful stories out in the field, some of them pretty sobering. We were out setting stakes for widening a drainage ditch and talking with an old timer running a piece of heavy equipment called a dragline excavator. It has a long boom and a bucket pulled by a cable. The old timer told a harrowing study about his son, a dragline operator himself, who suffered a terrible accident. Somehow the boom broke off and fell on him. It didn’t outright kill him and workers frantically called his father (the old timer). They told him to come quick to see his son before he died because they knew they couldn’t get him to a hospital quick enough from way out in the field. The old timer just said, “I don’t want to see him.” It was just like that, a simple statement. It sounded cold but he somehow conveyed that he just didn’t want his last encounter with his son to be under a horrifying circumstance like that.
The company had Christmas parties which almost everybody enjoyed a lot. There were some guys who had a hard time relaxing. I remember a driven, work-devoted surveyor, who was thinking about work. I could tell because there was some kind of game we were playing which involved writing something like a question on a piece of paper and giving it to someone else, some inane thing like that, I can’t remember the details. I gave him my slip, and he took it. While he scribbled something on it without looking at it, he looked away and mumbled, “I really don’t have a whole lot of time.” He was at the party but his mind was out in the field.
It’s hard not to absorb experiences like that early in your life when you’re still young and impressionable. Work can become a way of life. It doesn’t seem to make a difference what kind of work it is. Even Agent J in Men In Black 2 gets a short lecture from Zed after Agent J returns from a mission and seems like he’s on autopilot, asking Zed for yet another mission, “What do you got for me?” Zed says, “Dedication’s one thing, but this job will eat you up and spit you out.”
It’s even hard for some of the guys in Highway Thru Hell and Heavy Rescue 410 to relax; even after a heart attack, one older guy can’t wait to get back in the tow truck. But even he knows that it’s a young man’s job.
Anyway, I promised I would show a video about how to throw a chain, which I learned how to do back in the day. I’m pretty sure I couldn’t do it today.
Yesterday somebody asked me “So what do you do now that you’re retired?” I have come to dread the question. I told him I write this blog. That seemed to surprise him a little. It sounded a little lame to me as I said it. I’m not sure it’s the right answer to this question that I still don’t know how to answer, even though I’ve been retired for a little over a year.
I remember the blog post I wrote a couple of years or so ago, “Mindfully Retiring from Psychiatry.” It sounded good. It still sounds good even as I re-read it today. Others were reading it too, judging from my blog stats. I wondered if one of them was the guy who asked me the dreaded question.
I still exercise and do mindfulness meditation, although for several months after I retired, I dropped those habits. A lot was going on. We moved. I didn’t weather that process well at all. I was bored. In fact, I still struggle with boredom. The derecho hit Iowa pretty hard. It knocked over a tree in our front yard, which I had to cut up with a hand saw. The COVID-19 pandemic and social upheaval is an ongoing burden for everyone and seems to be directly related to making everyone very angry all the time. Sena and I are fully vaccinated but I’m pretty sure that more vaccinations are on the way in the form of boosters.
I’ve had to do things I really never wanted to learn how to do. Sena handed me a hickory nut she found in the yard this morning, reminding me of walnut storms we had at a previous home. I picked up scores (maybe hundreds) of walnuts there. I don’t want to do that again. I remember being jarred awake each time a walnut hit the deck.
And for the first time, I had to replace a dryer vent duct. I’m the least handy person on the planet. Our washer and dryer pair are both 54 inches tall and I found out that when you have to drag a big dryer away from the wall, you have to do it like you really mean business.
You don’t want to look at what’s behind the dryer. Worse yet is jumping down behind it in a space barely big enough for me to turn around. Getting out of it is even harder. Jump and press to the top of the machines and watch those cords and hoses.
I tried so-called semi-flexible aluminum duct. I switched to flexible foil duct, despite the hardware store guy telling me that it’s illegal. It’s not. You want to wear gloves with either because you’ll cut up your hands if you don’t.
Who’s the genius who thought of oval vent pipe on the wall when the duct is 4-inch round? It’s not illegal but it does make life harder. And how do you attach the duct ends to the pipes? Turn key or screw type worm drive clamps. If you don’t have enough room for a screw driver, the turn key style is the best bet. Good luck finding those wire galvanized squeeze-style full clamps. I think they’re often out of stock because they’re not only older, but easier to use and cheaper.
See what I mean? I would not even have the vocabulary for that kind of job if I were still working as a psychiatrist. I would just hire a handyman to do it—like I do for a lot of other things I still don’t know how to do since I retired. It’s sort of like that Men in Black movie line from Agent K when he tells Agent J what they have to do on their first mission: “Imagine a giant cockroach, with unlimited strength, a massive inferiority complex, and a real short temper, is tear-assing around Manhattan Island in a brand-new Edgar suit. That sound like fun?”
No, it doesn’t and neither does replacing a dryer vent duct or any number of things retired guys get to learn because they have too much time on their hands.
So, I’m really glad to change the subject and talk about other people who are doing things I admire. First is a former student of mine, Dr. Paul Thisayakorn, who is a consultation-liaison (CL) psychiatrist in Bangkok, Thailand. He did his residency at The University of Iowa Hospitals and Clinics. He put together a CL fellowship program in Thailand. The photo below shows from left to right: Paul, Dr. Tippamas, the first CL Psychiatry fellow, and Dr. Yanin. Dr. Tippamas will be the first CL Psychiatry trained graduate in Thailand next year and will work at another new medical school in Bangkok. Dr. Yanin just graduated from the general psychiatry residency program last year. Paul supervised her throughout her CL Psychiatry years. Now she is the junior CL staff helping Paul run the program. Within the next few years, Paul will send her to the United States or the United Kingdom or Canada for clinical/research/observership experience so she can further her CL education. Way to go, Paul and your team!
Dr Paul Thisayakorn and CL Psychiatry grads (see text for details)
By the way, that tie I’m wearing in the Mindfully Retiring from Psychiatry post picture (the one with white elephants; the white elephant is a symbol of royal power and fortune in Thai culture) was a going away gift from Paul upon his graduation.
The other is a heavy-hitter I met years ago, Dr. E. Wes Ely, MD, MPH, a critical care doctor who is publishing a new book,Every Deep-Drawn Breath, which well be coming out September 7, 2021. Our interests converged when it came to delirium, especially when it occurs in the intensive care unit, which is often. I met him in person at an American Delirium Society meeting in Indianapolis. He’s a high-energy guy with a lot of compassion and a genius for humanely practicing critical care medicine. I sort of made fun of one of his first books, Delirium in Critical Care, which he wrote with Dr. Valerie Page and published in 2011, the same year I started a blog called The Practical Psychosomaticist (which I dropped a few years ago as I headed into phased retirement). Shortly after I made fun of how he compared the approaches of consult psychiatrists and critical care specialists managing delirium, he sent me an email suggesting I write a few posts about the ground-breaking research he and others were doing to advance the care of delirious ICU patients—which I gladly did. I think he actually might have remembered me in 2019 when he came to present a grand round in the internal medicine department at University of Iowa Hospitals & Clinics (I wrote 3 posts about that visit: March 28 and April 11 and 12).
In the email Dr. Ely sent to me and many others about the book, he said, “Every penny I receive through sales of this book is being donated into a fund created to help COVID and other ICU survivors and family members lead the fullest lives possible after critical illness. This isn’t purely a COVID book, but stories of COVID and Long COVID are woven throughout. I have also shared instances of social justice issues that pervade our medical system, issues that you and I encounter daily in caring for our community members who are most vulnerable.”
I look up to these and others I had the privilege of working with or meeting back before I was not retired and struggling to come up with a good answer to the dreaded question: What do you do now that you’re retired?
This is just a post from a retired psychiatrist who barely passed the statistics course in medical school, so take it with a big grain of salt. I found an article written by Rocco J. Perla about something called Shewhart control charts to monitor the course of pandemic fluctuations. I noticed it because of what Perla commented on, which is the tendency of the press to make sensational headlines about every squeak in the turning wheel of COVID-19, including CDC making changes in masking guidelines leading to congressmen calling for investigations of the CDC for making the changes. It makes it look as though we don’t know what we’re doing.
I don’t know if Shewhart charts can help us make better decisions about what to advise us to do at the community level to help monitor and predict outbreaks. But it looks like we need to try something better soon. Because I can’t stand the pop-up ads at the U.S. News & World Report web site and limitations on how many articles I can view for free where I first saw Perla’s story, I looked up his original article published in the Int J Qual Health Care.
This led to my discovering the web site ISQua (International Society for Quality in Health Care). There I found a Shewchart for my state of Iowa, which shows what happened here this month. I don’t know if the Iowa Department of Public Health (IDPH) is already using it and I’m not qualified to tell them what to do. By the way, I think that mindset of “Don’t tell me what to do” crankiness might be an epiphenomenon of the COVID-19 pandemic. Nobody wants to be told to wear masks or to get a vaccine. It just leads to a pandemic of backlashes. I don’t know if Rocco is right about the Shewhart chart method not being in use by public health officials. But I want to go on record as not telling anybody what to do.
The Shewhart charts look labor intensive and maybe that’s why some public health departments don’t use them. They’re understaffed and overworked. Iowa has been scaling back the collection and reporting of COVID-19 data, partly because things appeared to be so rosy early in July. I’m not so sure how rosy they’ll be after the Iowa State Fair in August, which is expected to draw about a million visitors.
But I’m not telling anyone not to go to the state fair and I’m not telling anyone to wear a mask and I’m not telling anyone to get vaccinated. I’m not even telling anyone to pay any attention to Perla’s article on the Shewhart chart. I am telling you that I’m too old and cranky to be getting backlashes about any of this business.
Have fun at the fair.
Perla RJ, Provost SM, Parry GJ, Little K, Provost LP. Understanding variation in reported covid-19 deaths with a novel Shewhart chart application. Int J Qual Health Care. 2021;33(1): mzaa069. doi:10.1093/intqhc/mzaa069
Inkelas M, Blair C, Furukawa D, Manuel VG, Malenfant JH, Martin E, et al. (2021) Using control charts to understand community variation in COVID-19. PLoS ONE 16(4): e0248500. https://doi.org/10.1371/journal.pone.0248500
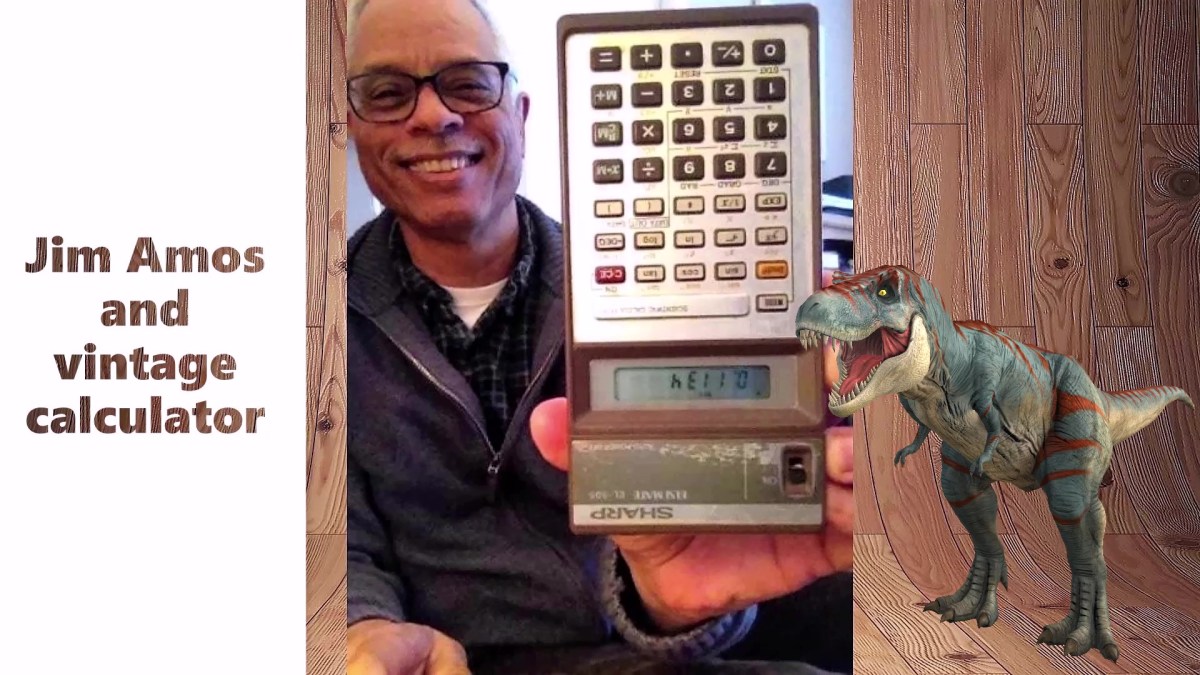
I still have a vintage calculator. It’s a Sharp ELSI MATE EL-505. You can buy one on eBay for $30. I bought this dinosaur back in the early 1980s just before heading to college at Iowa State University. It’s still usable, so just because it is vintage doesn’t mean it is wreckage. The original batteries last for over a decade at least, and probably longer.
My original major was engineering but I quickly changed my mind and eventually ended up in medical school at The University of Iowa. I’ve been retired from being a consultation-liaison psychiatrist now for a year. A couple of days ago, I ran into someone I know from the hospital and she asked me how retirement was going. She was on her way into and I was on my way out of Best Buy (nothing big, just a toner cartridge). I mumbled something quickly about having ups and downs but in general doing OK. The automatic door kept opening and closing. It was distracting so we said quick goodbyes.
We’ve got a couple of computers at home that are probably quickly becoming vintage, especially now that Microsoft is pushing the next iteration of the operating system (OS), Windows 11. The introduction is having a rough start, beginning with the puzzling PC readiness checker. You got a message that your PC would either be good to go with Windows 11—or not. That was pretty much it until the complaints started cropping up, generally starting with “What the heck do you mean it won’t run on my machine; why not?” They finally dropped the PC checker routine.
We’ve been through pretty much every Windows OS since Windows 95. If you’re wondering why go through all that, let me say that I actually started with a Mac at the hospital in my first year on the job at the hospital, on the advice of my mentor and first supervisor on the psychiatry consult service. He had a Mac and liked it a lot. On the other hand, even though I liked it too, it soon became clear that it was often impossible to interface with the PC-based office support staff network. I ended up going with a PC and have been dealing with Windows ever since.
Actually, my very first computer was given to me by an endocrine staff physician who co-attended with me in the medical-psychiatry unit. I didn’t pay a dollar for it and it was obviously vintage, in the negative connotation as I soon discovered after trundling it out to the parking lot in a cart and getting it home. When I pressed the power button—nothing happened. I returned it the very next day. My colleague could not explain it.
I could not get Windows 95 to run basic computer games at first. Even Myst, a simple point and click game that probably nobody remembers, would freeze and lock up the machine. I spent hours on the phone with tech support. You could do that then. It was not fun. Windows 98 was only slightly better. I’m still trying to forget Windows Me (Windows Millennium Edition or Mistake Edition). Windows XP had some longevity and ran OK. Windows Vista was another dud. I can’t remember much about Windows 7. I hated Windows 8 Live Tiles nonsense. We’ve been coping with Windows 10 and the updates to the present day.
Now here comes Windows 11 and seems like the most I can recall from articles about it is that it will have a Mac-like graphic interface. Then why shouldn’t I just go back to the Mac?
In some ways, my vintage calculator has done better over time than Windows. I can even spell “hello” on it.
Man, you know you’re retired when the most exciting event going on in a typical day is going out to get a haircut. It was an even bigger deal today because I haven’t been in a barber’s chair in about 35 years. Sena usually cuts my hair, but if I hadn’t gone out today to get a pro job haircut, I’d have very little else to write about except this poem that occurred to me last night.
I cannot say I know
That any UFO
Has an interstellar driver.
And if I then insist
No aliens exist,
Would you think I’m even wiser?
Weirdly, this doggerel is relevant since my head now reminds me of a bald alien. Don’t get me wrong, I actually think the stylist (I guess that’s what you call them nowadays) did a great job. I call it the Bullet Head cut or just the Bullet Head for short.
There were only two stylists and only one wore a mask. Masks were optional and since I’ve been fully vaccinated for almost 3 months, I left mine in my pocket.
My haircut took only 15 minutes. Did you want that sentence served with “literally?” OK here you go, but just this once: My haircut literally took only 15 minutes. I’ve never had such a fast haircut. On the other hand, I’ve had a lot shorter times sitting in barber shop waiting rooms. The shop takes walk-ins, if you’re willing to wait for at least an hour, often longer. The air-conditioning really worked. I was afraid to step outside to warm up a little because I didn’t know if that would remove me from my place on the wait list, which I could see on a video screen from my chair (along with the wait time, typically 90 minutes or more). Step to the right, step to the left, attempt to escape.
The other thing I was not hip to was that I could have checked in on-line using my smartphone. It also sounded like they would give you a jingle a few minutes ahead of your appointment time. I did it the old-fashioned way—and spent a long time reading the labels on hair care products. Ever wonder what’s in that tall red spray can labeled Big Sexy Hair? Me neither.
I know you’re wondering what clipper guard number the stylist used. It was a number 2, which typically leaves about a quarter inch length on a scalp which could burn under a noonday sun. But I like it. I got the senior discount and a coupon for next time. You probably want to know the name of the place; it was Great Clips. I would go back, especially if they turn the thermostat up. If you go, ask for the Bullet Head. Tell them I sent you.
It’s a cool, sunny afternoon. The lawn has just been neatly mowed by hard-working, reliable people who use power mowers. We used to mow lawns at previous properties using old-time reel mowers. I should say my wife used to do the lion’s share of that while I was at the hospital, working as a consulting psychiatrist. Now that I’m retired, I sometimes just wonder what I’m good for.
But it’s not hard to remember what Memorial Day is for. I was never a soldier. I never knew anyone who died in war. I only talked with military recruiters in a time so long ago, I barely remember being that young. I think they knew I was not ready to die for my country. They didn’t scorn or openly reject me. They treated me with respect.
Though I know what grief is because I am bereft, I cannot imagine what it’s like to grieve the death of any loved one who perished in war.
All I know is that when I was young and thought I wanted to be in the armed forces, there were recruiters who saw through me and knew I did not want to be a soldier.
They knew I did not want to die thousands of miles from my home in a bloody field. They knew I did not want to be buried forever in a foreign graveyard.
They knew I could not be one of them. Yet they did not treat me like an outsider. Now all I can do is be grateful. Now what I can do is honor them in silence.
We were on our way home yesterday and drove by a couple of restaurants (Wig & Pen Pizza and Vine Tavern and Eatery) with crowded parking lots. We have not seen that since the COVID-19 pandemic hit a year ago. This seemed to coincide with the CDC announcement of the new mask guidance indicating you can ditch the mask both outdoors and indoors—if you’re fully vaccinated. The updated guideline was a little hard to find on the CDC website, I noticed. It didn’t jump right out at you like the update on the pause of the Johnson & Johnson vaccine.
I checked the websites for both restaurants. They still say you have to wear masks. Pretty soon after that CDC update, news headlines appeared which provoked a few questions. How do you tell the difference between unmasked and masked persons who say they’re fully vaccinated? One headline said something like, “Get vaccinated or keep wearing your mask.”
And I saw a new term today, “vaccine bouncers.” Nobody wants to be a vaccine bouncer. In other words, since you can’t tell by looking at somebody if they’re fully vaccinated, how are you going to confirm the vaccination status of anyone? I don’t think there’s a lot of confidence in the ability to reliably detect the Pinocchio effect. And, regrettably, vaccination cards can be faked.
Some of us are vaccine hesitant. And some of us are unmask hesitant. Even though Sena and I are fully vaccinated, we still tend to wear masks indoors for now. And to be fair, the CDC guidelines stipulate that you should abide by local rules on wearing masks if required by public transportation and stores. But those guidelines are rapidly changing, maybe a little too rapidly for those who paid attention to daily scary news about upticks in coronavirus death rates when people sing too loud.
I feel like telling us to ditch the masks might be another way of offering an incentive to get vaccinated. Most of us hate masks. They’re hot, confining, make us feel too stifled to breathe easily, and so on. On the other hand, getting infected with COVID-19 is the ultimate respiration suppressor. As a recently retired general hospital psychiatric consultant, I’ve been called to critical care units to help manage anxiety in patients bucking respirators, which means they were fighting the ventilator tube. I didn’t have a whole lot to offer.
I think incentives are better than mandates, though (don’t spend it all in one place!). The best incentive is doing something to help all of us recover from the pandemic.