The title of the post is “Mysteries in History,” and before I chose it, I realized it had a familiar ring to it. It’s from Men in Black II. It’s an imaginary, cheesy, very low budget TV series narrated by Peter Graves in the movie. And it’s actually the perfect title for what my wife and I think about the Mason City, Iowa YWCA not being on the National Register for Historic Places. It’s a mystery in history which is anything but cheesy. I mentioned it in my previous post about the Mason City Ys.
I asked the State Historical Society of Iowa about it. It turns out it has been deemed eligible twice for nomination to the National Register, in 1991 and again in 2003, which was a year after the YMCA was added to the list.
The Mason City YWCA has never been nominated. Why it has never been nominated is the mystery in history.
It’s not a simple matter to get a building on the National Register. The process is outlined on the State Historical Society of Iowa web site. Unless you’re a professional historian, it’s a tough project and can take at least a year to accomplish.
I found a 36-page form on the web which documented the approval of the Mason City YMCA as a historic site fit for the National Register. It’s minutely detailed and I imagine it took a year just to complete the form itself, not to mention all the other hurdles you have to negotiate. The photos bring back memories of when I lived there as a young man. You could actually live in small, single occupancy dormitory rooms. You could do that at the YWCA as well, once upon a time.
There are 2 Artists who bought the YWCA building last year. It’s 100 years old and the place needs a lot of work. There’s a Trulia entry on the web which says it has housed a health spa, an intermediate care facility for people with intellectual and developmental disabilities called One Vision, a Women’s shelter and the list apparently doesn’t stop there.
A couple of articles say that one of the two new owners, Elisha Marin, filmed his music video, “Shining Out,” in an abandoned YWCA. They don’t say which one, but I wonder if it’s the Mason City YWCA. It would fit the long and winding story.
The Mason City Public Library (my favorite place when I was a kid) has a web page with a historical timeline indicating that the YWCA was built in 1918. The YMCA was dedicated in 1927 and placed on the National Register in 2002. I think a lot of the historical documents which helped get the YMCA listed might also prove the YWCA should be listed too.
I found another place called Five College Compass Digital Collections, which also has a ton of documents on microfilm about the Mason City YWCA. It was difficult to navigate and some of the pages were rotated, making them hard to read unless you can bend your head 90 degrees. You can click a button which apparently flips the pages upright, but transforms the text into something that looks like a foreign language.
You can get technical assistance in getting a property listed. The assistant would be available for 24 hours total. You can apply for grants, which can help with some of the expenses. It looks exhausting, though. Hey, I’m the kind of guy who flunked history.
It would sure be nice to solve this mystery in history. Maybe the 2 Artists will consider it. I wish them luck.
We were out on the Terry Trueblood Trail and saw a lot of different kinds of birds doing the things that birds—and humans do. Looking for mates, mating, nesting, hunting, feeding. We’re a little more romantic about it, at least sometimes.
Often, I wonder. Who are the real bird brains around here?
We took a walk this weekend on Scott Boulevard and eventually found our way to Fire Station No. 4. At first, we were struck by what looked like a real Dalmatian apparently sitting just inside the door. It was a pretty good sculpture. Just behind it was a large American Flag hanging on the wall. Below it was the title “Flag of Honor.”
One of the firefighters noticed us and welcomed us inside. He talked a long time about the Iowa City Fire Department and what they did. They responded to a lot of medical calls. In fact, those were the most frequent calls, fires not so much. He graciously answered our questions, including the one about The Flag of Honor on the wall. It’s to honor the victims and the heroes of the September 11, 2001 attack on America.
Later, I found out more on the web about the Flag of Honor. Over 800,000 Flags have been distributed across America. They’re in many places: public buildings, private homes, police and EMS stations, and firehouses.
I remember where I was on September 11, 2001. I was running up the stairs from the lower level to the first floor. I think I had just finished a psychiatric consultation and I was probably on my way to another one, or to my office. It was my usual routine. Like most general hospital psychiatric consultants, I was a lot like a firefighter, going from one urgent consultation to another, to the critical care unit, the emergency room, and others. My pager was like a fire alarm and off I would go.
I was on the stair landing just going up to the first floor. The stairs overlooked a lobby and the television on the wall was showing a video of one of New York City’s Twin Towers on fire, smoke all around it.
I stopped in my tracks and watched, not comprehending the scene. I can’t remember if the volume was high enough for me to hear the reporter. I don’t think it was. I just saw the fire and the smoke and at that moment I didn’t know what happened. That news I wouldn’t hear until later.
And then much later, in the summer of 2017, Sena and I took a vacation in New York City. Like many tourists, we saw the reflecting pools and Sena took a snapshot of me by the Callery Pear—the Survivor Tree.
The firefighter finally had to excuse himself, because there was somewhere he had to go, something he had to do.
He had probably been busy when we showed up, remarking on the Dalmatian which looked so lifelike, taking pictures of the Flag of Honor, asking questions about what Fire Station No. 4 does, listening to his answers, admiring his patience, his sense of humor, his sense of duty—and thanking him for all of it.
I ran across this quote the other day: littera scripta manet. The English translation is, I think, “the written word endures.”
Not to dwell too much on the prosaic side of the issue which is that, for me, often the word has been blurred because of problems with my vision. I just had retinal detachment surgery a little over a month ago and I’m making a good recovery. But early on I had a lot of trouble with blurry vision, tearing, and light sensitivity.
Just the other night though, I was able to read a section of a book without having as much blurred vision as I did before the surgery when I looked up from the page at something distant. I’ve been wearing progressive lenses for many years and it probably got worse because of the detached retina, which was chronic or maybe acute on chronic.
Now to get beyond trivialities, I saw the quote above in an issue of the University of Iowa publication, Iowa Magazine. It was in the last Old Gold column of University Archivist, David McCartney. He retired in March of this year. The title was “Old Gold: The Enduring Power of the Written Word.”
He notes the Latin expression is on the seal of the U.S. National Archives and Records Administration. McCartney’s point is that technology can undermine as well as strengthen the power of the written word. He identities Horace as the originator of the expression, “the written word endures.”
I went pecking around the internet and found out that a lot of people think an educator named Neil Postman was the originator of this quote. What makes me doubt this is that the original is in Latin, which suggests a much older origin. He was born in 1931 and died in 2003. Interestingly, Postman criticized the effect of technology on thought and culture.
A website that seems dedicated to explaining English translations of Latin indicates that the quote comes from a longer expression: Vox audita perit, littera scripta manet, which translates to “the spoken word perishes, but the written word remains.” One contributor says the originator was Horace. Another insists that “littera” does not mean word at all, although concedes that the proposed translation is correct, nevertheless.
Further, there is a Wikipedia entry which cites the Latin expression differently, “verba volant, scripta manent,” which in English is “spoken words fly away, written words remain.” The author says the proverb originated from a speech of senator Caius Titus to the Roman Senate.
Anyway, McCartney points out that the world is becoming increasingly digitized and that the average website lasts only a little over two and a half years. Some important digital records have been lost, unreadable (blurred?) because of improper management.
My previous blog survived about 7 years but is lost. Maybe that’s not such a bad thing. My current blog is a little over 3 years old. So far, I’m beating the odds as far as typical longevity, but is it worthwhile?
Both written and digital records have strengths and weaknesses in terms of durability. And deciding what to preserve and how is essential to any society. We need good stewards to help us decide.
Good luck in your retirement, David McCartney. I’m sure the University of Iowa treasures your stewardship. Let the written word endure unblurred.
I read a short article, “The case for pursuing a consultation-liaison psychiatry fellowship” by Samuel P. Greenstein, MD in Current Psychiatry (Vol. 1, No. 5, May 2022). After 3 years as an attending, he found his calling as a C-L psychiatrist, especially after getting teaching awards from trainees. But when he applied to academic institutions for position as a C-L academic psychiatrist, people kept advising him to complete a fellowship training program in the subspecialty first. He gave it careful thought and did so, even he called it going “backwards” in his career.
On the other hand, he believes C-L fellowships will help meet the challenges of addressing rising health care costs and improving access to what most people see as the critically important goal of providing access to integrated mental health and medical care.
I’ve been retired from consultation-liaison psychiatry for two years now. I get an enormous sense of achievement on the rare occasions when I hear from former trainees who say things like “For me you were…one of the most outstanding attendings I had at my time at Iowa.” And “I can at least take comfort that University of Iowa is still at the forefront of psychiatry.”
Several years ago, one of the residents suggested starting a Psychosomatic Medicine Interest Group (PMIG). This was before the name of the subspecialty was formally changed to Consultation-Liaison Psychiatry in 2018. I know many of us were very pleased about that.
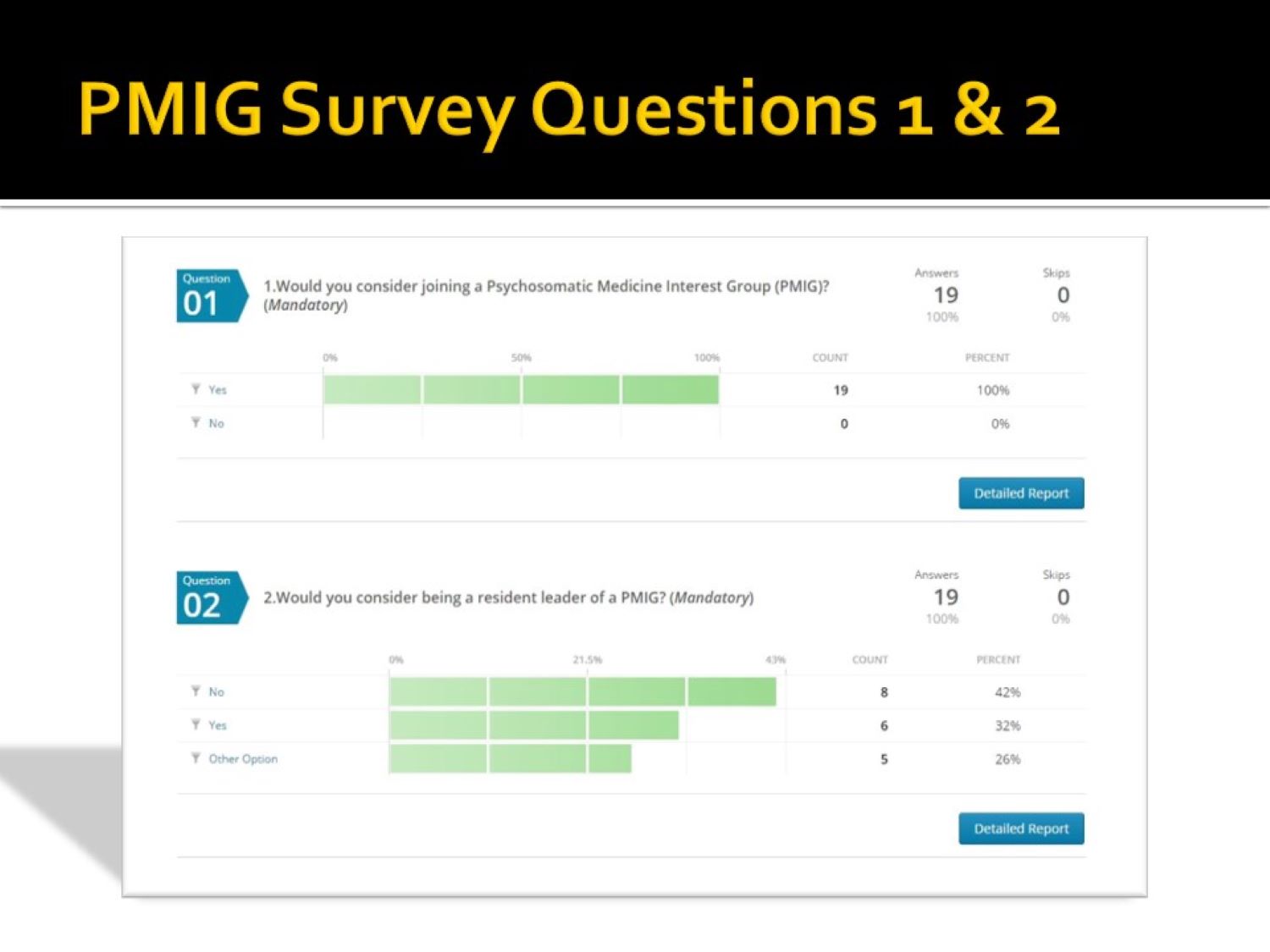
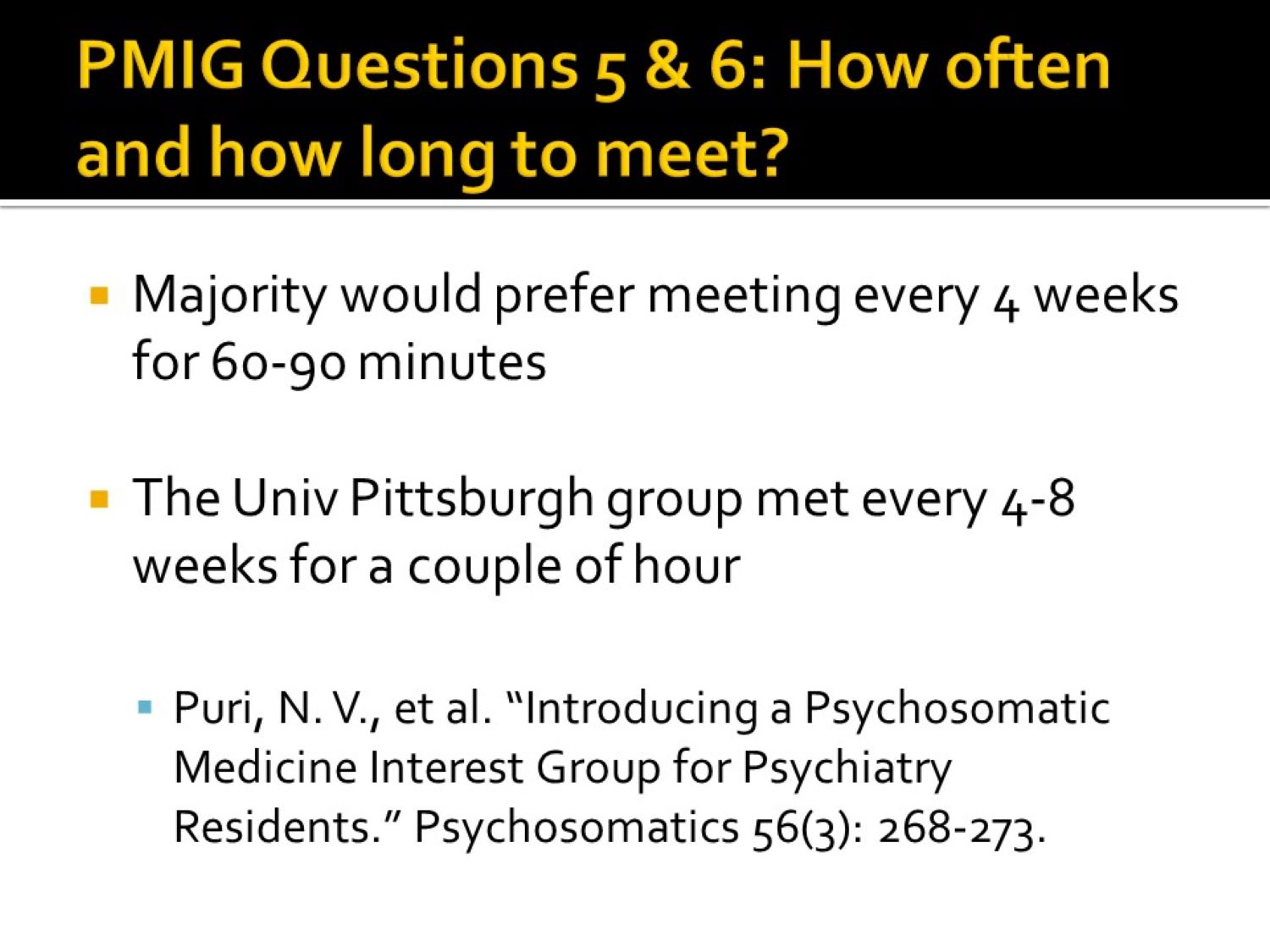
I sent a short survey (see the gallery below the slide show) to the faculty and residents in an effort gauge support for the idea and readiness to participate. I used a paper published at the time to guide the effort, (Puri NV, Azzam P, Gopalan P. Introducing a psychosomatic medicine interest group for psychiatry residents. Psychosomatics. 2015 May-Jun;56(3):268-73. doi: 10.1016/j.psym.2013.08.010. Epub 2013 Dec 18. PMID: 25886971.).
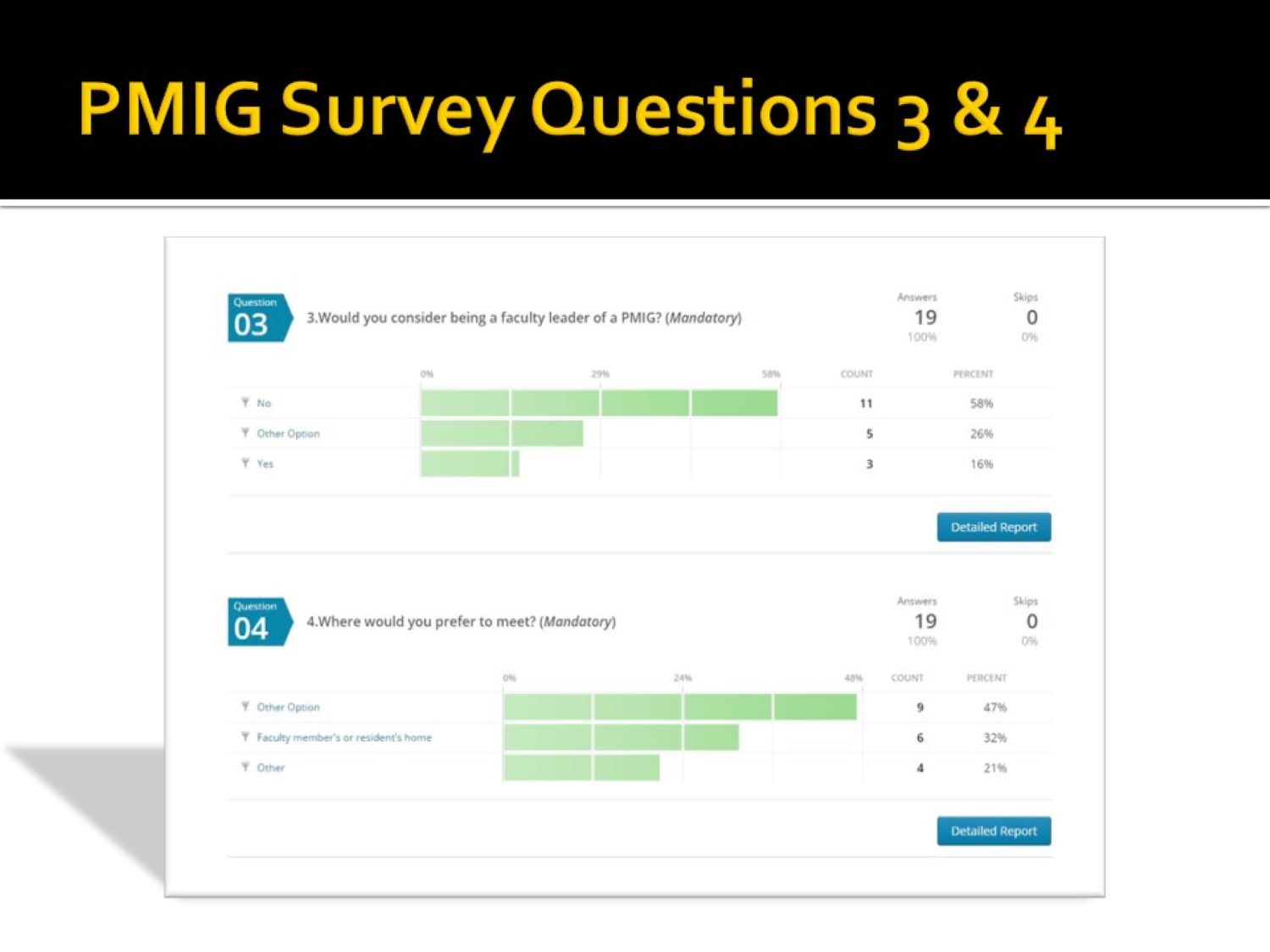
You’ll notice on slide 4 one faculty member’s comment, “I think it doesn’t matter whether faculty are certified in PM.” As Dr. Greenstein discovered, it probably does matter, at least if you want to be board certified.
I was initially certified by the American Board of Psychiatry & Neurology (ABPN), but I objected to the whole Maintenance of Certification (MOC) program, as did many other psychiatrists. I eventually declined to continue participating in the MOC process. However, I notice that the Delirium Clinical Module that I and a resident put together is still accessible on the ABPN website.
Although response numbers were low, there was clearly an interest in starting the interest group. There was also an incentive to reapply to the ACGME for approval of a Psychosomatic Medicine (Consultation-Liaison Psychiatry now) fellowship.
My attempt years earlier had been frustrating. While it was approved, I couldn’t attract any fellows, forcing me to withdraw it without prejudice (meaning another application for approval could be attempted). Fortunately, that situation changed later. The Psychiatry Department at The University of Iowa now has an early career C-L psychiatrist who graduated from the reinstated C-L fellowship.
As the saying goes, “What goes around comes around.” Although the origin of that saying might have originated in the 1970s, at least one person thought his grandmother had her own version in the 1950s: “You get what you give.”
This is just a reminiscence. I know the word “wherefores” in the title is old-fashioned, but I’m an old guy and so what? When I was a young guy living in Mason City, Iowa where I grew up, I could not afford to rent an apartment. Shortly after I became an emancipated minor, I was lucky to be able to rent a dormitory room at the YMCA at 15 North Pennsylvania Avenue. The building was placed on the National Register of Historic Places in 2002.
Reference: M, Ben and Clio Admin. “Mason City YMCA (1926-200).” Clio: Your Guide to History. September 30, 2021. Accessed May 10, 2022. https://theclio.com/entry/140366
I guess that makes me sort of historic too. It was built in 1926. I think it rents out apartments now. I recently read a Globe Gazette article about the beginnings of the YWCA on 2 South Adams and it was built in 1918. The current Mason City Family YMCA is located on 1840 S Monroe Avenue.
There is a local legend that bank robber John Dillinger and his gang stayed at the YMCA while planning their robbery of the First National Bank in 1934. Track star Jesse Owens stayed there briefly in 1937, starring for a basketball exhibition.
I recently read a Globe Gazette article on the web about the beginnings of the YWCA on 2 South Adams. As I said, it was built in 1918, but I don’t know when it closed. The YWCA sat empty for years until a couple of artists got a loan from a local realtor. They’re renovating it. (Zachary DuPont. “Old YWCA building takes strides toward renovation,” Globe Gazette on line, 10/29, 2021, updated 1/18/2022).
They plan to build artist studios on the 2nd floor, performance space where a basketball court is presently, a community area and art gallery on the first floor, and make single apartment/dormitory rooms cheaper than regular apartments (maybe similar to what the YMCA had many years ago, up to 12 units on 3rd floor). My wife, Sena, stayed there briefly and that was very helpful.
The YWCA is not on the National Register of Historic Places. It’s not clear why. The artists have raised some money with a GoFundMe campaign toward the renovation project. The website is titled “Save the Historic Mason City YWCA.” So why is it not on the National Register of Historic Places?
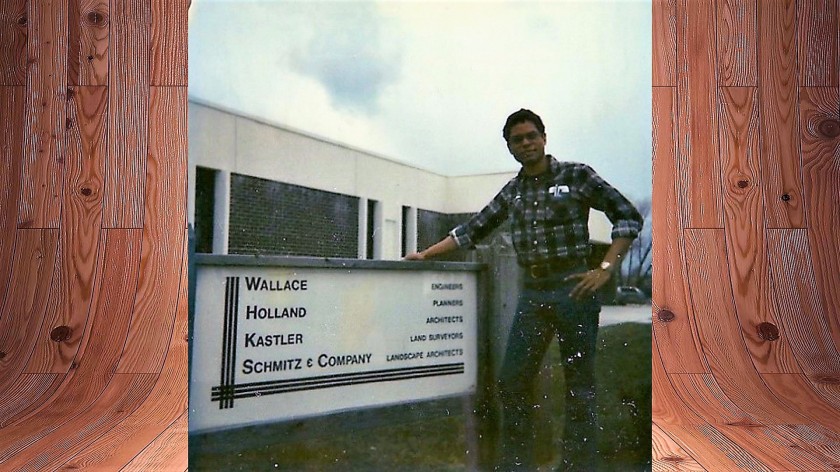
Anyway, I moved into a very cramped room at the YMCA on either the 3rd floor in my teens. I was working as a draftsman and surveyor’s assistant for WHKS & Co., a consulting engineering company. It was mainly a place to sleep. Most of the time I was traveling, working on out-of-town jobs such as relocating Highway 13 between Elkader and Strawberry Point (really more like straightening out all the curves in it), land surveys and the like.
Portrait of the legacy blogger as a young man
I also have a distant memory of learning how to swim at the YMCA when I was a kid. I was terrified of even putting my face in the water and used to get fierce headaches just getting into the pool. I’m not sure how I got over it, but I did.
There were a fair number of eccentric characters who lived at the YMCA back in my day. I didn’t consider myself one of them and that’s probably why I didn’t end up staying there for decades. I could have worked in Mason City for the rest of my life, having breakfast at the café in the old Brick and Tile Building on East State Street, and eating all of my other meals in restaurants along Federal Avenue until I was too old to do much more than sit in Central Park.
But I didn’t. I’ll get to that.
There were a number of guys who stayed long term at the YMCA. It was kind of uncomfortable for that. There was only one communal bathroom and shower. There were no kitchens. There was barely enough room for a bed, a kneehole desk and chair, and you had to listen to the cast iron heater radiator clank most of the night. They were just sleeping rooms, but it was a little too loud to sleep sometimes because of the banging noise from the radiators.
I found out one of my neighbors was building a motorcycle in his room. He was very proud of it. It was a large machine and took up a lot of space. He kept it very clean. The Director of the YMCA at the time was John Calhoun and he’d been involved with the YMCA since 1943. He had a reputation for being pretty strict about the rules, which likely included one prohibiting the building of motorcycles in your dormitory room. We kept the motorcycle a secret of course.
There were some guys whose wives kicked them out of the house. They were always going out for coffee. They could drink a lot of coffee, smoke a prodigious number of cigarettes, and talk non-stop about how bad things were in the world in general.
There was an old candy bar vending machine on the floor. I got what must have been an ancient Butterfinger. I bit into it and found what I thought was half a worm wriggling around. Finding a worm was bad enough, but half a worm alarmed me. Where was the other half?
I even telephoned the local hospital emergency room to ask if I were in danger of some kind of poisoning. There was only a pay phone available at the YMCA, even for the guys who lived there. The ER doc couldn’t stop laughing long enough to say more than I’d most likely be just fine. “Fine,” he said. I haven’t eaten a Butterfinger since.
I met one guy who kept saying basically one thing over and over: “So my ancestors came over on the Mayflower. All well and good…” Then he would sort of trail off. His expression didn’t change at all. In fact, he looked flat most of the time. I didn’t know it at the time, but he probably had a chronic, severe mental illness.
I don’t remember who told me that the athletic director was gay. I don’t know if he was or not, and it didn’t matter. He treated everybody with kindness and respect and we treated him likewise. I remember he gave me sound advice about the safest length of time to spend in the steam room after I almost blacked out after sitting in there way too long.
I learned the dollar bill jump trick from an older guy in the weight room. He didn’t call it that, but it was a similar challenge. The idea is to bet you that you can’t bend over or squat, grab just your toes and jump over a broomstick—without letting go of your toes. I think he actually showed it to me and another youngster. We tried over and over. All we did was fall and laugh. It’s a good thing he didn’t make us bet.
There wasn’t much to do around there except play pool. There was this underfed-looking guy who used to play a deadly game of call shot eight ball. He amazed me because he worse eyeglasses that were as thick as pop bottle bottoms. I didn’t understand how he could even see his own hands. He won every game.
I know it sounds a little dull, living at the YMCA. On the other hand, I’d have probably been in a tight spot if the YMCA had not been there when I was young.
I read a Wikipedia article about the song in the late 1970s, “Y.M.C.A.” by the Village People. The author noted that in the early days of the YMCA, the single room occupancy dormitory rooms were for guys who moved to the city from rural areas to find work. Later, YMCA tenants tended to be youth “…facing life issues” or the homeless.
And I met Sena there. She switched jobs from working across the street at a school administration building to work at the YMCA.
I never hung out at the front desk as much as I did after she showed up. I pretended to read the newspaper a lot. She probably wondered why I was always there. We played bumper pool. I don’t remember who won the games, but I had trouble concentrating on my shots.
She does everything. There must be a God because she is God’s gift to me. I guess after all, I did just fine after eating half a worm.
I’m not a fan of country music, generally. I usually listen to the Big Mo (AKA John Heim) blues show on KCCK 88.3 on Friday nights. I also listen to the Music Choice channel on TV, either Easy Listening or Light Classical.
However, a few nights ago I heard the song “Grandpa, Tell Me ‘bout the Good Old Days” on Easy Listening. It was a haunting instrumental that I can be a sucker for sometimes. I noticed the rhythms that alerted me to its country genre, though.
On the other hand, the melody had that quality which makes me want hear nothing else for a while. An artist named Danielle Nicole sang “Bobby” on a Friday night blues in the second week of February, which did that for me.
How I feel about this kind of music reminds me of the Greek myth of Odysseus, who on his long journey back to Ithaca following the Trojan war, he and his crew of sailors encountered the island of the Sirens. Their voices made anyone who heard them forget everything but their haunting voices. The sailors wasted away, leaving hills of their skeletons. The only way to pass the Sirens safely was to stop the ears of the crew with wax. But Odysseus wanted to hear the song and made his men lash him to the mast so that he could not join those who gave up their lives to hear the music. He ached for knowledge in the lyrics even more than the melody of the songs the Sirens sang, and for the deepening of the spirit which absorbed the souls of those who heard the hypnotizing cadences. Just hearing the melody could extinguish the will to live.
The good old days melody didn’t extinguish my will to live, of course. But it was easy to get caught up in it and I noticed how deeply I reminisced. I looked up the lyrics and, at first, thought they were just quaint. Then they began to sound ironic to me.
The song (and I mean mainly the melody although the irony of the lyrics was part of the spell) seemed to raise the image of a bubble, which I know sounds strange. I remember blowing soap bubbles when I was a kid. They are delicate, bright, beautiful, but fragile—just like those so-called memories of what some older people call the good old days. You don’t even want to breathe too hard on them, which would hurt the spell, the illusion that there are such things as shiny, clear, light as air memories of a past without sorrows that float forever.
Of course, the bubbles burst as I got older. Innocence doesn’t last long in the world. It seems like every generation has to learn this all over again. The joys are replaced by broken promises, sorrows, and regrets.
Eventually, a golden haze settles over the anger, shame and guilt, softening the broken edges of the world which cut our souls. And the golden stories of the good old days that never happened save us for a little while every now and then—as long as there are those willing to sing them. Because we can almost always find the bubbles when we need them. Be careful not to listen to the Sirens too long. And if you do, be careful not to breathe too hard on the beautiful and fragile bubbles.
How much better would it be if we make the good times happen here and now?
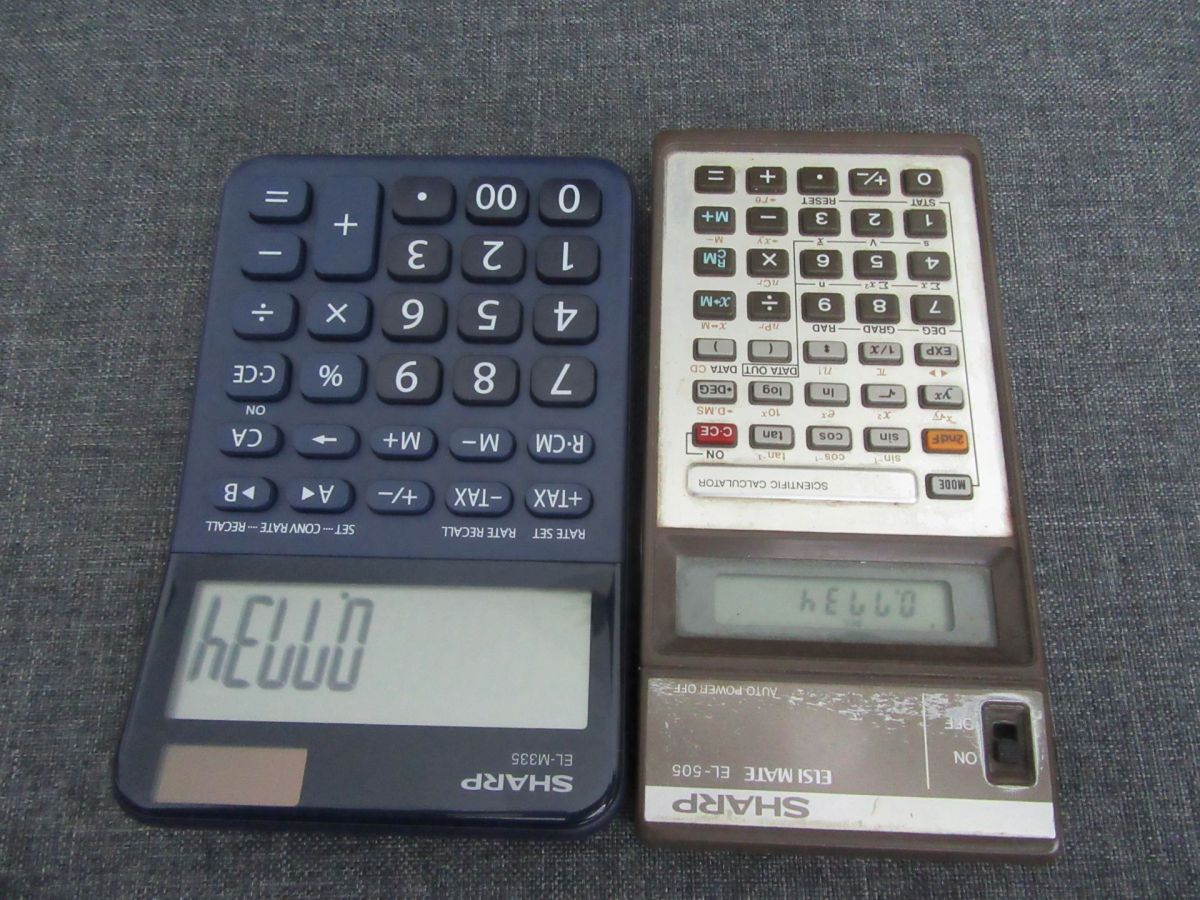
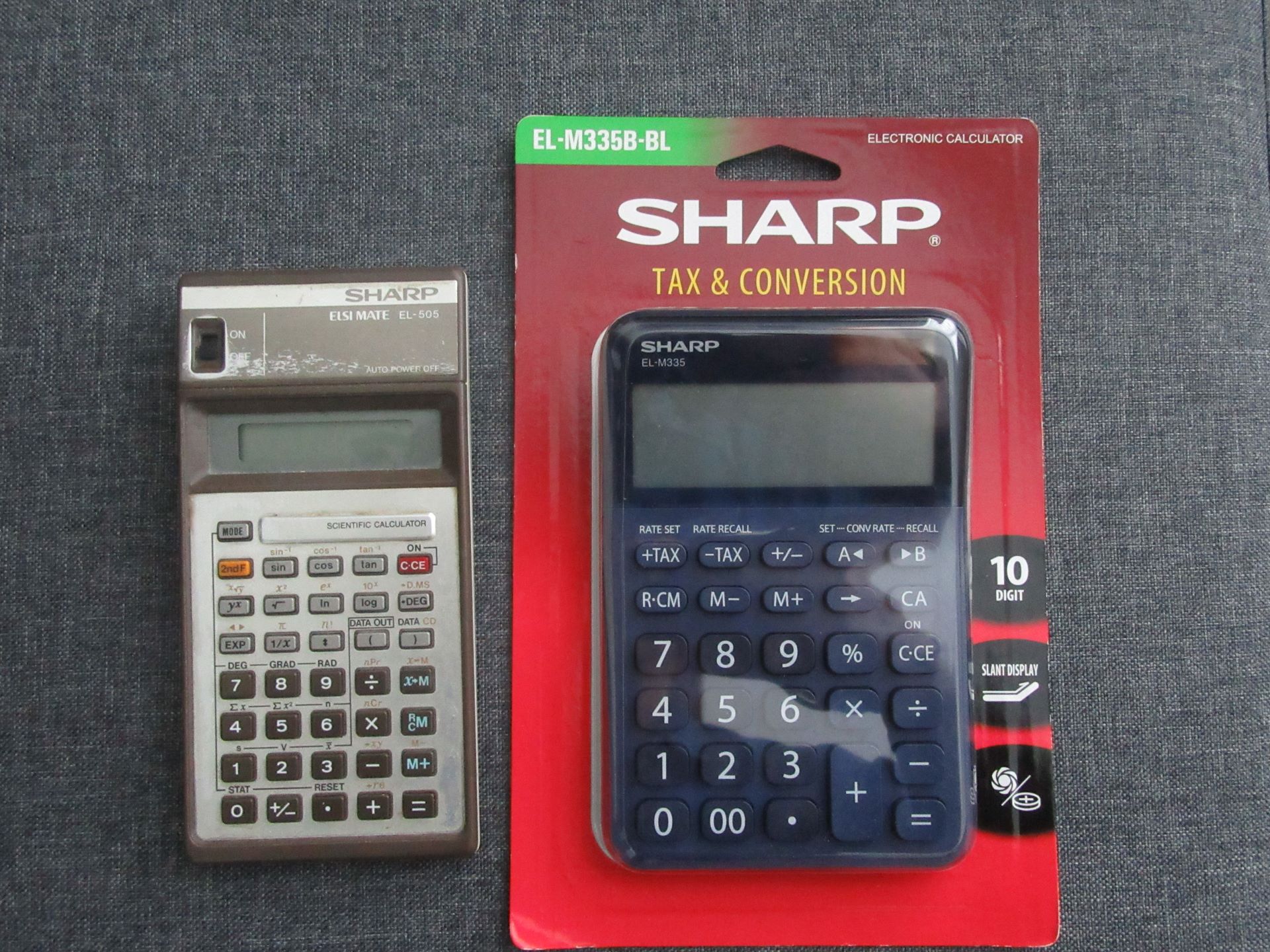
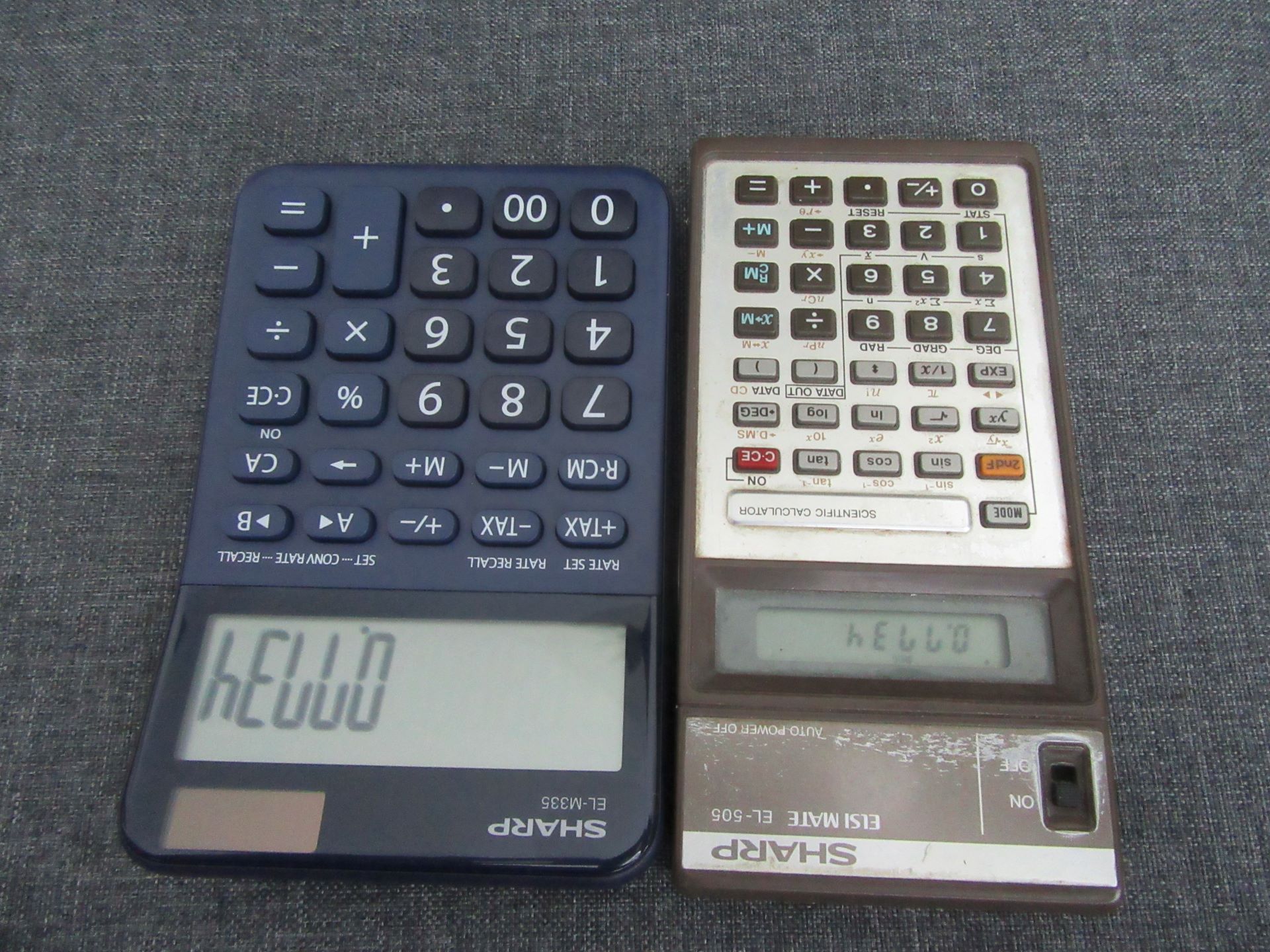
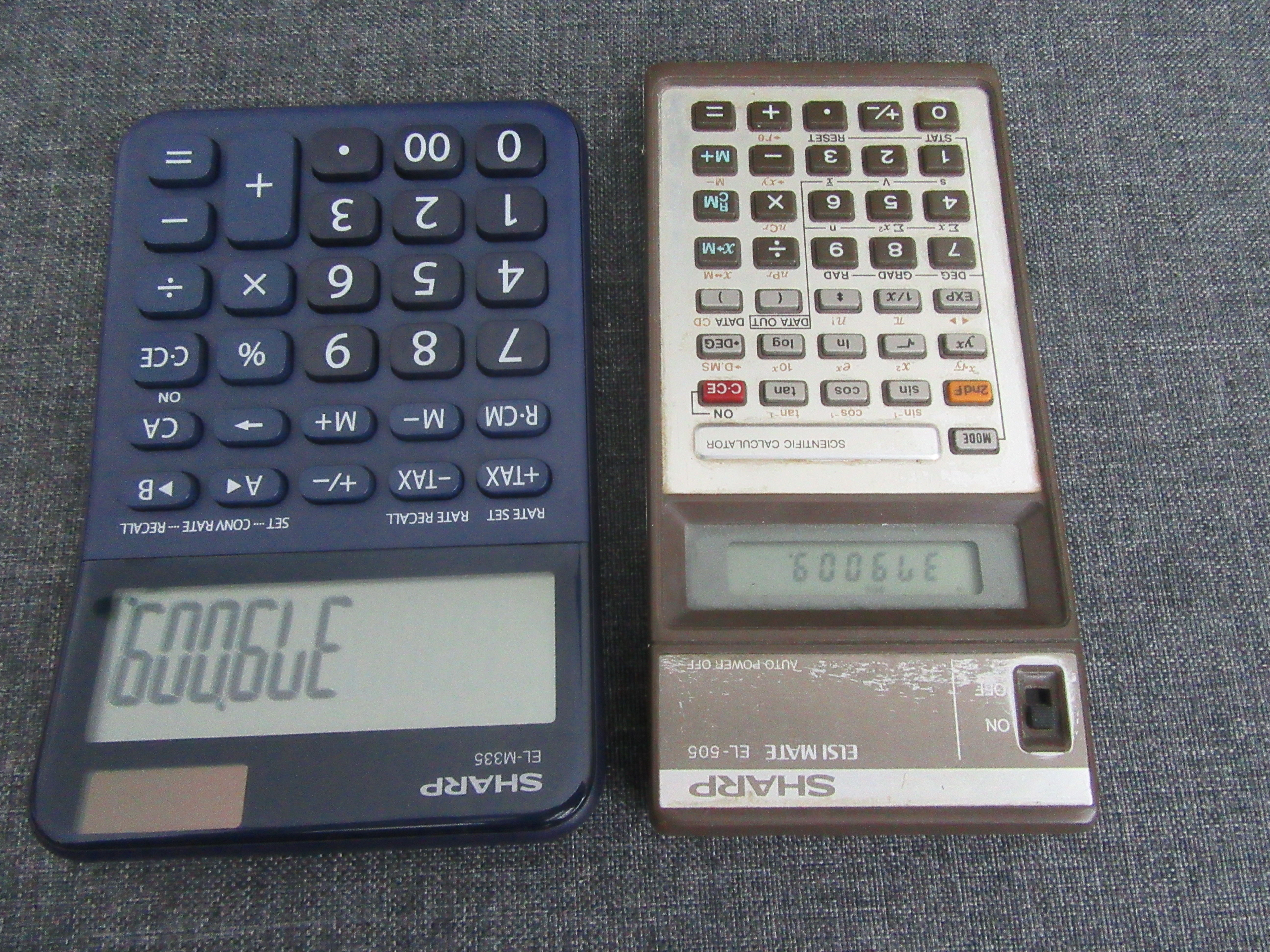
Well, Sena ordered a new Sharp calculator and we just got it. It’s a Sharp EL-M335. It has a bigger, easier to see display and larger keys than the vintage Sharp ELSI MATE EL-505. We stuck with the Sharp brand because it’s durable and reliable.
I’ve mentioned the old Sharp EL-505 in previous posts, mainly to highlight the idea that vintage doesn’t necessarily mean useless. It served well for over 30 years believe it or not, and we didn’t change the two double AA batteries for more than a decade. You can call me a liar or demented, but it’s the truth.
I’ll probably use the new one to do things like total up our Scrabble game scores to find out how badly I lose each time we play and to spell words on it. It’ll be used for other tasks.
And an added plus—the words I spell on the new calculator are larger and easier to read than on the old one.
I remember buying the old one shortly before we moved to Ames, Iowa so I could start college at Iowa State University. I got the Sharp ELSI MATE EL-505 because it had special scientific functions on it because I was planning to study engineering.
I quickly found out I didn’t have the head for the mathematics necessary to get through an engineering program. So, I ended up using it for things like—scoring Scrabble games and spelling words.
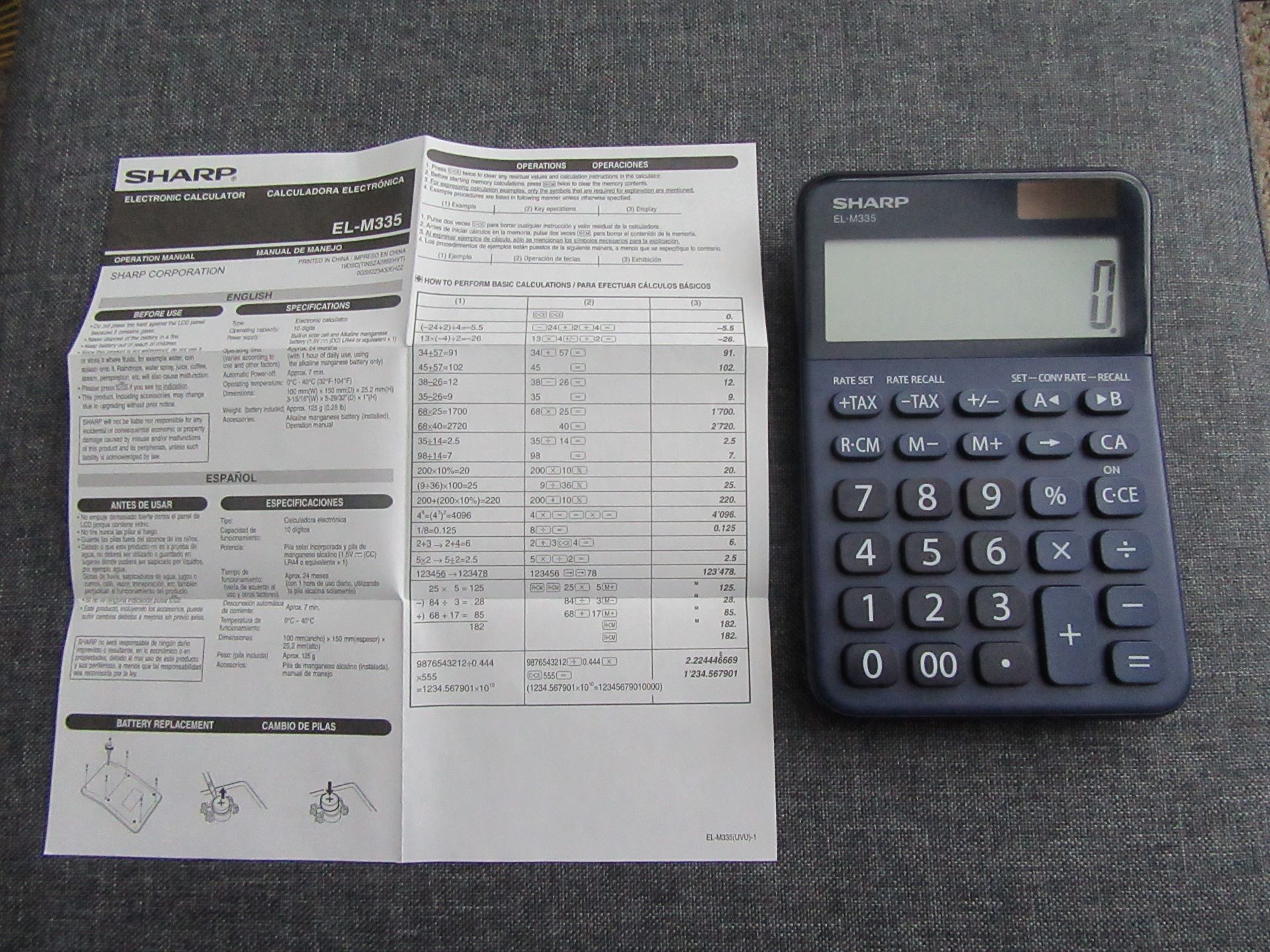
The Sharp EL-M335 actually uses a solar cell and a backup Alkaline manganese battery. I wouldn’t have been able to tell you that unless I used a magnifying glass to see the operation manual’s tiny print. It’s a good thing the display uses bigger characters.
However, replacing the battery in the new calculator will require using a very tiny screwdriver to remove 6 very tiny screws. It’s a good thing we have a very tiny Kobalt screwdriver set with Phillips and flat head bits that you can store in the handle.
So, there you have it. We have a brand new, modern Sharp calculator. And it looks sharp. But we don’t plan to throw away our vintage calculator. It’s been good to us.
I’ve seen several articles on Medscape about how to convince doctors to retire or even force them to retire when they’re too old to practice. The articles are titled, “How Old Is Too Old to Work as a Doctor?”; “Are Aging Physicians a Burden?”; and “When Should Psychiatrists Retire?”
The Great Resignation almost makes the debates about this moot. Doctors, including psychiatrists, are retiring or quitting in droves because of burnout, largely related to the stress of the Covid-19 pandemic in the last two years. However, a lot of physicians were quitting medicine even prior to the pandemic.
The same arguments get trotted out. Doctors often lack insight into their failing cognition and physical health as they age. How do we respectfully assess and inform them of their deficits? Are there gentle ways to move them away from active medical, surgical, and psychiatric practice and into mentoring roles to capitalize on their strengths in judgment and experience?
The decision to persuade some doctors to retire, not so much because of advancing chronological age but because of dwindling cognitive capacity and other essential skills, needs to be handled with empathy and wisdom, especially if this is going to increase the workload for the rest of the doctors holding the fort.
Like the song says, “Break it to Me Gently.”
And speaking of songs, this doctor retirement discussion reminded me of a song I heard on TV when I was a kid. I could remember just one line, “Your Love is Like Butter Gone Rancid.”
I thought I heard it on an episode of an old TV sitcom, The Real McCoys. In fact, it was from a 1968 episode of the Doris Day Show called The Songwriter. Hey, we watched what my mom wanted to watch.
The song’s awful lyrics, which Doris Day “wrote” (only as part of the show; it was actually written by Joseph Bonaduce) were tied to the melody of “My Bonnie Lies Over the Ocean”:
Your love is like butter gone rancid,
It’s no good now, it’s started to turn,
I pray that it’s just like the man said,
You can’t put it back in the churn
Can’t put
Can’t put
Can’t put it back in the churn
Oh, durn!
You can’t put it back…in the churn
The context here is that another character (Leroy) in the show had previously submitted the lyrics of a similarly bad song (“Weeds in the Garden of My Heart”) to a crooked music publishing company that lavishly praised the song and promised to publish it—at Leroy’s expense.
Leroy was clueless about getting cheated. He was too dumb to know how bad the song was, but his feelings would have been badly hurt if the family just flatly told him that. They had to figure out a way to break it to him gently. So, Doris wrote the equally terrible “Your Love is Like Butter Gone Rancid,” and performed it for Leroy and the rest of the family. Leroy thought Doris Day’s song was garbage but didn’t know how to tell her without hurting her feelings.
Doris then told Leroy she was also going to submit her rancid song to the crooked publishing company.
After Doris got the exact same letter the crooked company sent to Leroy—he learned his lesson and felt supported, gosh darn.
Anyway, I was moved to write a short song about the doctor retirement issue, “When Doctors Are Too Old to Practice,” sung to the tune of “My Bonnie Lies Over the Ocean” of course:
When doctors are too old to practice
And can’t tell your elbows from knees
When they sing old songs to distract us
It’s high time we tell them to leave
High time
High time
It’s high time we tell them to leave
Oh, beans!
It’s high time we tell them…to leave
I’ve received hundreds of billions of requests for a sing-a-long version of “My Bonnie Lies Over the Ocean” because you can’t sing the parodies unless you know the original tune.
I searched the web for a picture of ambivalence and had a tough time finding one. The featured image comes close. The reason I’m ambivalent is because of a conflict I have about the Iowa Hawkeye football program, which is currently the subject of a lawsuit by former African American players compared to the University of Iowa asking fans to find a new song to accompany the traditional Hawkeye Wave, in which players and fans wave at the kids watching the game from the UI Stead Family Children’s Hospital.
I think it’s a moving gesture. I’d like to formally nominate a new song. But I’m not sure I could call myself a fan, given the conflict between two principles: honoring the families with sick children, and also wanting a just outcome for the former football players suing the Hawkeye football program, alleging that it created a hostile environment.
I dislike bringing this up, mainly because I want to be fair to both sides. On the one hand, the former Hawkeye players and the Hawkeye football program somehow need to find justice. On the other, I really believe families love the Hawkeye Wave, and so do I. I’m very ambivalent.
I even have a song I’d like to formally vote for. It’s “I Lived” by OneRepublic. It was originally dedicated to children with cystic fibrosis and, when the music video was released in 2014, it featured Bryan Warnecke, a 15-year-old showing how he not only lived with, but triumphed over the disease.
I want the best for both sides of this conflict between ideals. I don’t know if I can count myself as a fan of the Hawkeye football program right now.
But speaking as a retired University of Iowa general hospital psychiatric consultant who once served as a colleague to the pulmonology specialists who called me to help care for the emotional and physical health of their patients with cystic fibrosis, a few of whom were living into young adulthood—they are Hawkeyes and so am I.
So, I’m voting informally for “I Lived” because I think it captures the spirit of what the Hawkeye Wave is really all about—kindness, generosity, and hope.
Featured image picture credit Pixabaydotcom.
Update April 24, 2022: I voted formally today for “I Lived” by OneRepublic. You can submit yours here.