-

Sometimes Names are Hard
I was listening to John Heim aka Big Mo on the Big Mo Blues Show (radio KCCK 88.3) last night and he was talking about this time of year, calling it “Indian summer.” He second-guessed himself about calling it that and even wondered aloud whether it might be “politically incorrect.” Sometimes names are hard. All…
-
The Secret of Patience
The secret of patience is to do something else in the meantime. Croft M. Pentz A few days ago, Sena noticed a noise in one of the sunroom window shade wand controls. She can hear noises I can’t hear, which is a good thing. She wondered if the wand battery needed recharging. We have 3…
-
Maybe We Need a Dose of Humor
Sena and I were listening to the Mike Waters morning radio show (KOKZ 105.7) this morning and his invitation to listeners was to call in and quote their favorite dumb question. One of the callers recited something which was actually a George Carlin joke. Neither one of us thought we heard it right, but it’s…
-
Look on the Bright Side
Yesterday was the first day of Autumn. Happy Autumn! Was that too cheerful? You know, I used to watch the show Monty Python’s Flying Circus years ago. I thought it was outrageously funny. What reminded me of the show was Sena telling me that on Wednesday night, a member of the Flying Circus cast, Eric…
-

Thoughts on Suicide Risk Assessment
I know the term “suicide risk assessment” sounds very clinical. That’s because I did it for many years as a consultation-liaison psychiatrist in the general hospital. The human part of it was using the suicide safety plan, which I got from the Centre for Applied Research in Mental Health & Addiction (CARMHA). You can download…
-
What Would Make Psychiatry More Fun?
I just read Dr. George Dawson’s post “Happy Labor Day” published August 31, 2022. As usual, he’s right on the mark about what makes it very difficult to enjoy psychiatric practice. And then, I looked on the web for anything on Roger Kathol, MD, FACLP. There’s a YouTube video of my old teacher on the…
-
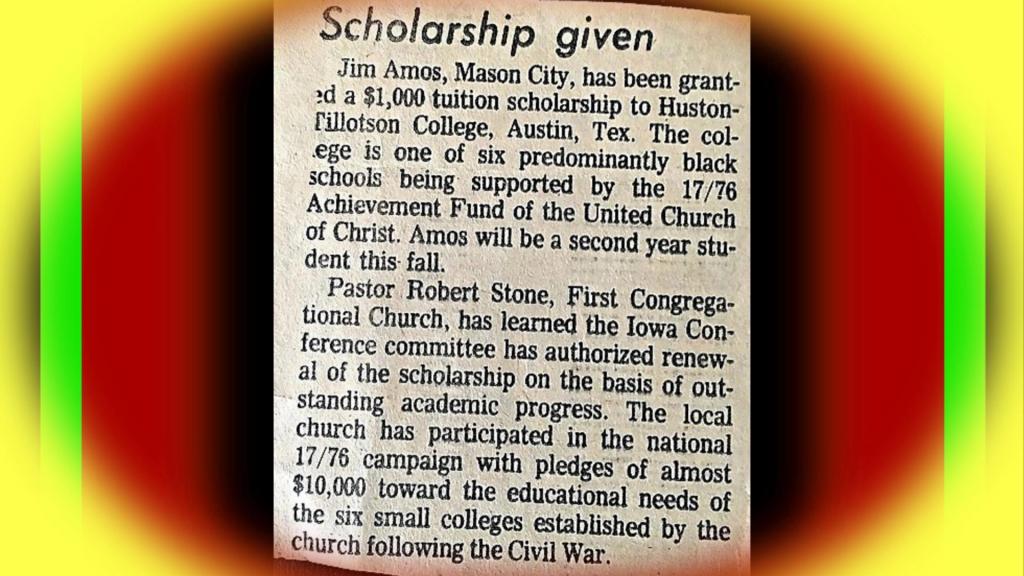
On the Other Hand Thoughts on HBCUs
Historically Black Colleges and Universities (HBCU) are in the news lately. It reminds me of the short time I spent at Huston-Tillotson College. It was renamed Huston-Tillotson University (H-TU) in 2005. I was there in the mid-1970s. A new President and CEO was just named this month, Dr. Melva K. Williams. And H-TU was recently…
-
Thoughts on Doctors Going On Strike
I read Dr. H. Steven Moffic’s two articles in Psychiatric Times about the strike by mental health workers at Northern California Kaiser Permanente (August 16 and 26, 2022). So far, no psychiatrists have joined the strike. However, this piqued my interest in whether psychiatrists or general physicians have ever gone on strike. I have a…
-
Memories and Condolences
I was thinking of my hometown, Mason City, for some reason today. Then I just happened to think of my childhood pastor, Reverend Glen Bandel. The last time I looked him up on the web was about a year ago and saw a news item dated in 2019. He was celebrating his 90th birthday. I…