


Here’s another oldie but goodie blog post, “It’s Survey Time.” It’s a blast from the past (May of 2011) but it needs a short introduction on why I’m reposting it.
So, I’m about a week out from my surgery for a detached retina. I’m doing pretty well. I keep thinking about a question a nurse asked me right after I was taken to the recovery room from the operating room. I was a little hazy because I’m pretty sure I got some sedation medication, although I was definitely mostly awake for the procedure. The nurse asked me, “Well, can you answer a question for me; will a stone float on water?”
First of all, I gave the right answer, “No.” More importantly, I was momentarily stunned because I recognized the question is from the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). And I told the nurse that. It reminded me of my early career as a general hospital consultation-liaison psychiatrist.
Most of my old blog posts from The Practical Psychosomaticist are about my frustration over what seemed to be my fruitless efforts to teach nurses and physicians about how to prevent, assess, and manage delirium.
I can’t tell you how happy I was that my recovery room nurse asked me a CAM-ICU delirium screening question.
I mentioned the American Delirium Society (ADS) in the post and also found a fairly recent article on the CAM ICU. Among the authors were those I met at one of t he first ADS meetings: Malaz Boustani and Babar Kahn.
“It’s Survey Time!”:
“I know, I know, I can hear it out there, “Doesn’t Dr. Amos ever learn? Nobody does surveys and polls!” Hey, that’s OK; I have so much fun doing them anyway. Of course, it would be nice to get some responses… I’ve talked to you and I’ve talked to you, and I’m done talkin’ to you! Come back here, I’m not done talkin’ to you!
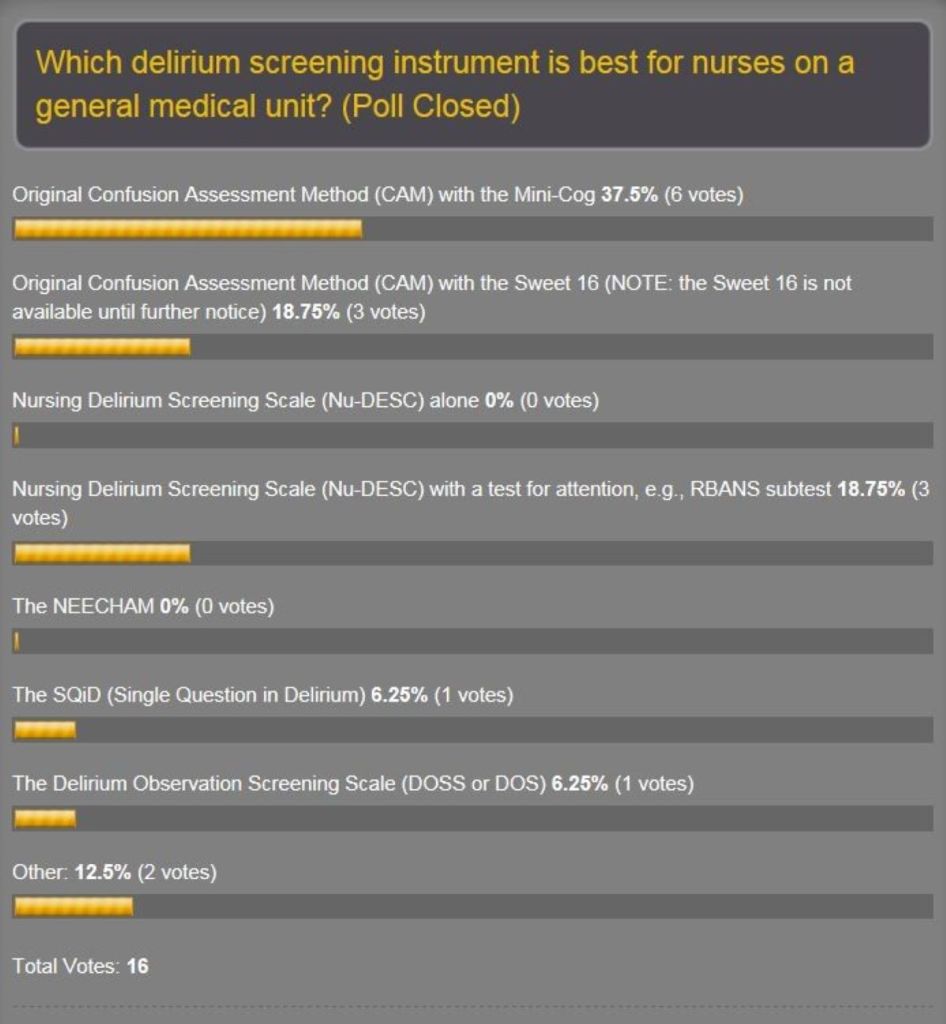
Anyway, the new poll for what’s hot and what’s not about delirium screening scales is up on the home page. The original one was partly to help our delirium prevention project committee to decide on which one to use. Well, the original got only 16 responses…but they were great responses! The amazing thing was that, despite the paucity of votes, the results were plausible. See the results:
Recall that at our 7th project meeting we selected the DOSS. What? There is good literature supporting all of these scales and a lot of factors influence selection of any tool, not the least of which is feasibility, which is mainly ease of use. That means it’s quick and doesn’t require a lot of training or additional assessments. And you should use a tool that’s validated for the patient population you want to protect from delirium. I probably got a lot of questioning looks at the screen when this poll came out because the Confusion Assessment Method-Intensive Care Unit (CAM-ICU) was not on the list. Well, you heard it from one of the main dudes on the team that developed the CAM-ICU that it’s probably not appropriate for use on general medical units…Dr. E. Wesley Ely himself (see post April 29, 2011). Hey, as far as the ICU patient population goes, the CAM-ICU is the holy grail. We need to keep looking for a sensitive and specific tool which is quick and easy for nurses to administer on general medical units.
We’re going with the DOSS. And one of my neuropsychologists, John, is offering to run neuropsychology test batteries on the patients that nurses screen with the DOSS. Atta boy, John! Neuropsychologists are going to be indispensable in this area. I remember pushing for the addition of subtests of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS), especially the Coding test in order to detect delirium early as possible. It didn’t make it, but it was close. This has been advanced by another one of our neuropsychologists here who’s done some delirium research in the bone marrow transplant unit with delirious patients. Hey, I still wonder what we could accomplish if the Coding test were added to the DOSS or even the Nursing Delirium Screening Scale (Nu-DESC). Maybe there’s already somebody out there putting a practical implementation plan for that into the real world.
So why do the poll again? Because I’d like to see if I could persuade nurses from large American and world organizations to put the nickel down and vote. And if I keep shoving this thing out there, maybe somebody will let us know that, hey, we’re not in this alone and offer to collaborate.
And I stole a couple of survey questions from our group to see what physicians and nurses think about how they manage delirium. It’s a way to take a snapshot of the culture of how docs and nurses work together on delirium recognition and interventions. And hey, why am I doing that? Because I’m a thief…no, no, I mean the reason is delirium is a medical emergency and we all need to work together to find ways to understand it better in order to prevent it. The American Delirium Society (ADS) tell you why delirium prevention is critical in the endless search to find ways to deliver high-quality medical care to patients:
Delirium Simple Facts:
- More than 7 million hospitalized Americans suffer from delirium each year.
- Among hospitalized patients who survived their delirium episode, the rates of persistent delirium at discharge, 1, 3 and 6 months are 45%, 33%, 26%, and 21% respectively.
- More than 60% of patients with delirium are not recognized by the health care system.
- Compared to hospitalized patients with no delirium and after adjusting for age, gender, race, and comorbidity, delirious patients suffer from:
- Higher mortality rates at one month (14% vs. 5%), at six months (22% vs. 11%), and 23 months (38% vs. 28%);
- Hospital stay is longer (21 vs. 9 days); Receive more care in long-term care setting at discharge (47% vs. 18%), at 6 months (43% vs. 8%) and at 15 months (33% vs. 11%); and
- Have higher probability of developing dementia at 48 months (63% vs. 8%).
And have you registered for the ADS inaugural conference on June 5-7 in Indianapolis? Good for you! And are you going to bring back something from that conference for The Practical Psychosomaticist, and I don’t mean doughnuts? That’s the spirit! The surveys have spaces for free-text comments as well, which I want to hear!”











