A couple of days ago, while we were playing cribbage, Sena asked me who sang the song “Against the Wind.” I offered a name, which later turned out to be wildly wrong. It bugged her so much she got up from the cribbage game and went to the computer to look it up.
Of course, Bob Seger wrote the lyrics and sang it. She asked me what I thought it meant. I wasn’t sure at the time. I hadn’t thought about it for a really long time.
I read about it on the web. I didn’t know what the lyric “8 miles a minute” meant and found a forum message saying that it corresponds roughly to the speed of a cruising airliner which is about a “480 mph.” That’s technically more like 480 knots, which converts to about 550 mph.
Anyway, it’s really fast and might be a way of saying you’re moving through life at breakneck speed. In Seger’s case, it might have had a more concrete meaning, referring to flying all over from concert to concert.
The song was released in 1980, which was about the time we moved to Ames so I could go back to college at Iowa State University (ISU). It was a big change from working as a draftsman and land surveyor’s assistant in my hometown of Mason City.
If you extend the “against the wind” metaphor a little bit, Sena and I were both moving against the wind in terms of our place in society, income level, location and educational attainment. I thought I wanted to be an engineer at the time, mostly because I had worked for years for consulting engineers.
Backing up in time a little, I had done some undergraduate college work previously at an HBCU (historically black college/university), Huston-Tillotson College (now Huston-Tillotson University) in Austin, Texas in the mid-1970s.
That was also a kind of move against the wind. I grew up in Mason City, and often I was the only black kid in grade school. I got used to that, although the racism was more overt back then and it was difficult sometimes to bear up against that kind of wind. On the other hand, I felt like a fish out of water at H-TC. I just felt like I didn’t fit in. It was part of the reason I left Austin.
It was also challenging to fit in at ISU. I figured out quickly that I would never complete the engineering degree program. The math and hard science courses were tough from the beginning and only got harder. I realized I was going against the wind there.
So, I changed my major and settled on medical technology, which led to working in a hospital laboratory. But it took about a year to get a job after graduation. Looking back, It was a frustrating time and that really felt like pushing against a headwind. I don’t know what I would have done without Sena.
I finally got into medical school at the University of Iowa. Biostatistics and Biochemistry were brutal. I was very close to quitting before the 3rd year of clinical rotations. I doubted I was cut out to be a physician. I thought about going back to surveying. But I didn’t.
Many deadlines, commitments, and struggles leading to brief forays from academia into private practice led me to think of myself as more of a fireman or a cowboy than an academician. Yet I spent most of my career at the University of Iowa.
Now I’m retired. Sena is my shelter against the wind. I guess if you look hard enough, just about anybody can relate to Bob Seger’s song. Let the cowboys ride.
The attack a few days ago by what was most likely a mentally ill person on staff at the recently opened GuideLink Center in Iowa City reminded me of what may appear to be disparate views by mental health professionals on the link between mental illness and mass violence perpetrators.
The GuideLink incident involved a person who assaulted GuideLink staff and who also left bags containing incendiary devices at the center and another building in Iowa City. The person is being charged with terrorism and is currently in custody in the Johnson County Jail.
I have not seen information about any injuries sustained by the mental health center staff. There were no explosions or fires at either location where incendiary devices were left. Bomb squad experts removed the devices. It’s not clear whether the perpetrator had been a GuideLink Center client.
Dr. H. Steven Moffic, MD, a retired psychiatrist who writes for Psychiatric Times, readily says that the perpetrators sometimes do have mental illness that at least contributes to committing acts of mass violence. Dr. George Dawson, MD, another retired psychiatrist, seems to say that the major reason for mass shootings is the ready availability of guns, a culture of gun extremism, and mental illness accounts for a small proportion of acts of mass violence.
But neither Dr. Moffic nor Dr. Dawson say that it’s only either mental illness or guns (or other instrument of mass violence) that lead to acts of mass violence. Both are important.
I’m a third retired psychiatrist and by now some readers might be asking themselves whether they should listen to any retired psychiatrist. Experience counts.
Speaking for myself, as a general hospital psychiatric consultant I was frequently faced with violent patients in the general hospital. Often, I found it necessary to ask a judge for a court order to involuntarily hospitalize a violent and/or suicidal patient on a locked psychiatric unit by transfer from an open medical or postsurgical unit.
In order to obtain an order in the state of Iowa, I had to be able to state to the judge that the patient in question had a treatable mental disorder and was an acute threat to himself and/others. In most situations, I had an open bed on a locked psychiatric unit available ahead of time.
Even if a Code Green was necessary, I usually had an inpatient resource to which I could move the patient. A Code Green is a show of force or takedown maneuver by a specially trained team to control a violent patient while minimizing injury to everyone involved.
I don’t know if that kind of approach is even possible in a community crisis stabilization setting like the GuideLink Center. I think it’s fortunate that it partners with many other community resources including the Johnson County Sheriff’s Office.
The outcome of the incident at the GuideLink Center was that the overall safety of the staff, the patient, and the community was preserved. More resources like this are needed everywhere. They deserve all the support we can give them.
I just saw a pretty funny story in the news about an old guy who was not allowed to donate blood at a Scotland blood bank because he refused to answer a new questionnaire asking whether or not he was pregnant.
I thought that was uproariously funny. Then I read the rest of the story and found another punchline: The director of the Scottish National Blood Transfusion Service defended the question on grounds of respect for inclusiveness. So, I had a good laugh about that one too.
I wonder if there could more than just a yes/no question about whether a guy is pregnant. We need space for an essay response: “No, but my 33-year-old son is living in our basement. Would you please adopt him?”
There are two other comical trends. One is providing tampon dispensers in men’s bathrooms. Another is the chuckle-provoking pregnant man emoji. What kind of email message would you use that for unless it’s a joke?
The issue is less farcical when you consider there is a rare psychiatric disorder known as delusion of pregnancy in men, otherwise known as Couvade syndrome. I never encountered it in my career as a psychiatric consultant in the general hospital.
And there is a psychiatric disorder known as pseudocyesis or delusional pregnancy as well as denial of pregnancy in women.
This reminds me of a fascinating episode from Blue Planet II in which David Attenborough filmed the transformation of a kobudai wrasse female fish into a male.
I gather some people are pretty angry about this exaggerated inclusivity trend. I’m not sure why.
We all need a good laugh whenever we can get it nowadays—as well as a fresh perspective.
I’m going to chime in mainly to show a few graphics I found which I think send a clear and simple message. Before I get to that, I just want to mention a few anecdotes to show how little hands-on experience I have with guns.
My earliest memory of any contact with firearms is in early childhood. My dad and a friend came home from a hunting trip with some rabbits for dinner for the family, which included my younger brother and my mother. I don’t know who cleaned or cooked them. I’m pretty sure my mom would not have had anything to do with them. I got my first taste and didn’t like it and said so to my dad. He introduced me to the word “gamey.” I didn’t know meat could taste gamey. The other thing I got from that meal was a mouthful of buckshot. I silently vowed I would never eat anything like it again while I lived.
My next encounter with guns was a YMCA program for kids to learn how to shoot. I might have been in my early teens, maybe even younger. We were given BB guns and instructed to do some target shooting. The paper bullseye targets were set up several yards away. I took many shots and collected my target to show the instructor.
I thought I hit it once and pointed to the hole. The instructor looked at it critically for a few seconds and then told me kindly that the hole was where the pin was stuck to fix the target to the wall. I never touched another gun.
Fast forward to when I was a third-year medical student getting through my clinical rotations at the University of Iowa. In 1991, a physics graduate student named Gang Lu shot and killed 6 people on campus including himself, wounded another rendering her paralyzed from the neck down, all apparently because he was not chosen to get an award for his dissertation. I remember feeling shocked when I read about it in the newspaper.
Now let’s move to some graphics I found at a website maintained by The University of Sydney, GunPolicydotorg, International firearm injury prevention and policy https://www.gunpolicy.org/. It makes it easy to put together comparison statistical graphics on things like gun violence. I compared the United States to New Zealand, Australia, and Canada. Click the next few links in order to get the message. In my opinion, I think the last one is a consequence of the first few.
The annual Kickball challenge between University of Iowa Department of Psychiatry Residents and Faculty is coming up in June. You know what that means.
Losers suspend the winners’ trophy in Jello. Somebody did that when we played Matball several years ago. If you need a recipe:
Matball was the forerunner of Kickball in the department. I think the Kickball rules are here. Federal law says you have to play in 95-degree heat with insane humidity driving the perceived temperature to slightly above that on the surface of the sun. Other rules:
If the ball melts, faculty wins.
For every point the residents score, faculty automatically score 5.
Faculty may tackle the base runner at any time.
If it rains, faculty win by 10 points.
The thing to do is to recruit Sasquatch for your side, who will always boot the ball into the next county. Bring many replacement balls. Sasquatch will bring the beef jerky.
The games are fun to watch. Residents jumping over faculty; Faculty collapsing from heat stroke.
I never played.
I’m trying to recall whether faculty ever won a game. I don’t think we ever did. I think that’s why the trophy ended up in Jello.
I read a short article, “The case for pursuing a consultation-liaison psychiatry fellowship” by Samuel P. Greenstein, MD in Current Psychiatry (Vol. 1, No. 5, May 2022). After 3 years as an attending, he found his calling as a C-L psychiatrist, especially after getting teaching awards from trainees. But when he applied to academic institutions for position as a C-L academic psychiatrist, people kept advising him to complete a fellowship training program in the subspecialty first. He gave it careful thought and did so, even he called it going “backwards” in his career.
On the other hand, he believes C-L fellowships will help meet the challenges of addressing rising health care costs and improving access to what most people see as the critically important goal of providing access to integrated mental health and medical care.
I’ve been retired from consultation-liaison psychiatry for two years now. I get an enormous sense of achievement on the rare occasions when I hear from former trainees who say things like “For me you were…one of the most outstanding attendings I had at my time at Iowa.” And “I can at least take comfort that University of Iowa is still at the forefront of psychiatry.”
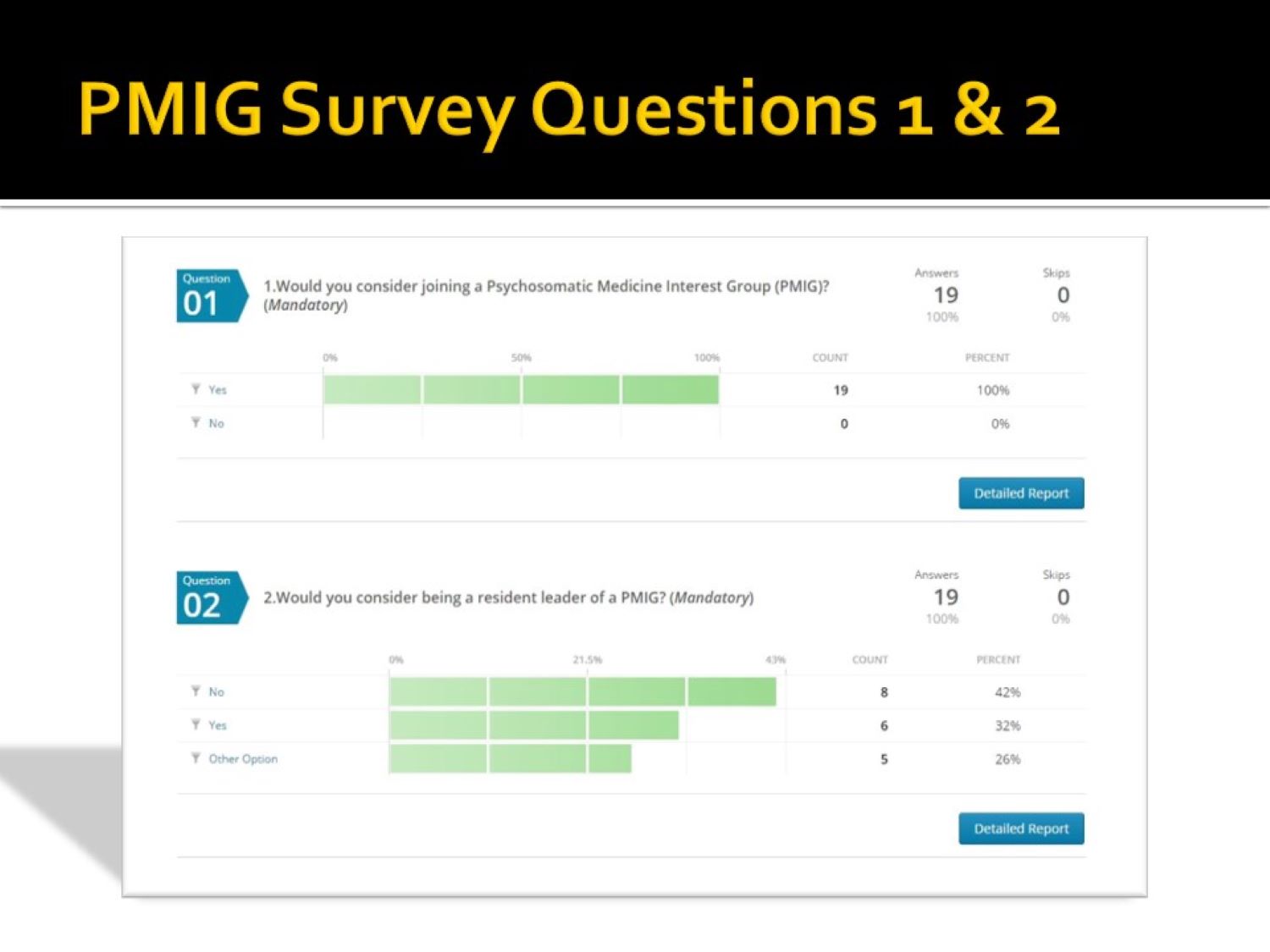
Several years ago, one of the residents suggested starting a Psychosomatic Medicine Interest Group (PMIG). This was before the name of the subspecialty was formally changed to Consultation-Liaison Psychiatry in 2018. I know many of us were very pleased about that.
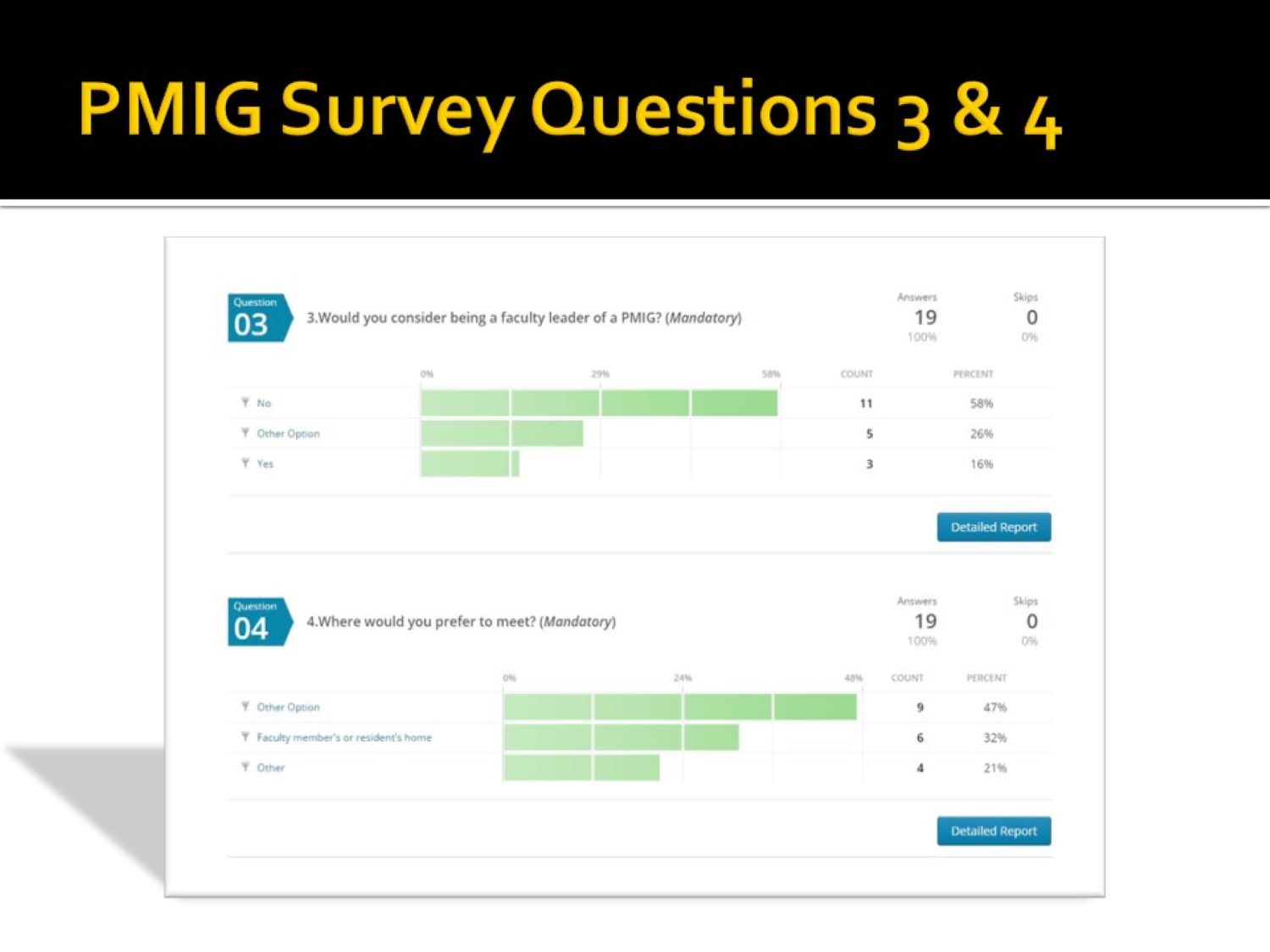
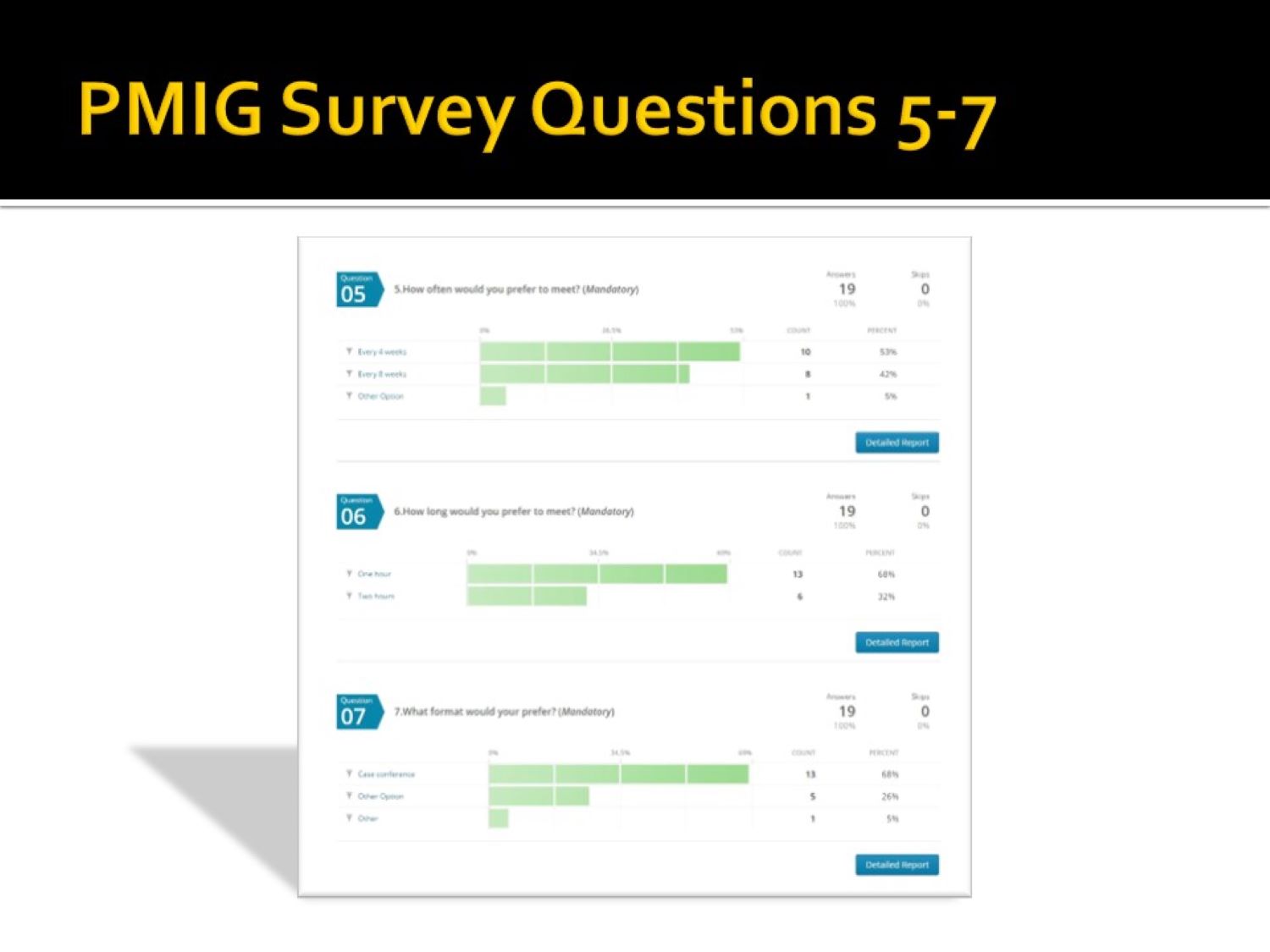
I sent a short survey (see the gallery below the slide show) to the faculty and residents in an effort gauge support for the idea and readiness to participate. I used a paper published at the time to guide the effort, (Puri NV, Azzam P, Gopalan P. Introducing a psychosomatic medicine interest group for psychiatry residents. Psychosomatics. 2015 May-Jun;56(3):268-73. doi: 10.1016/j.psym.2013.08.010. Epub 2013 Dec 18. PMID: 25886971.).
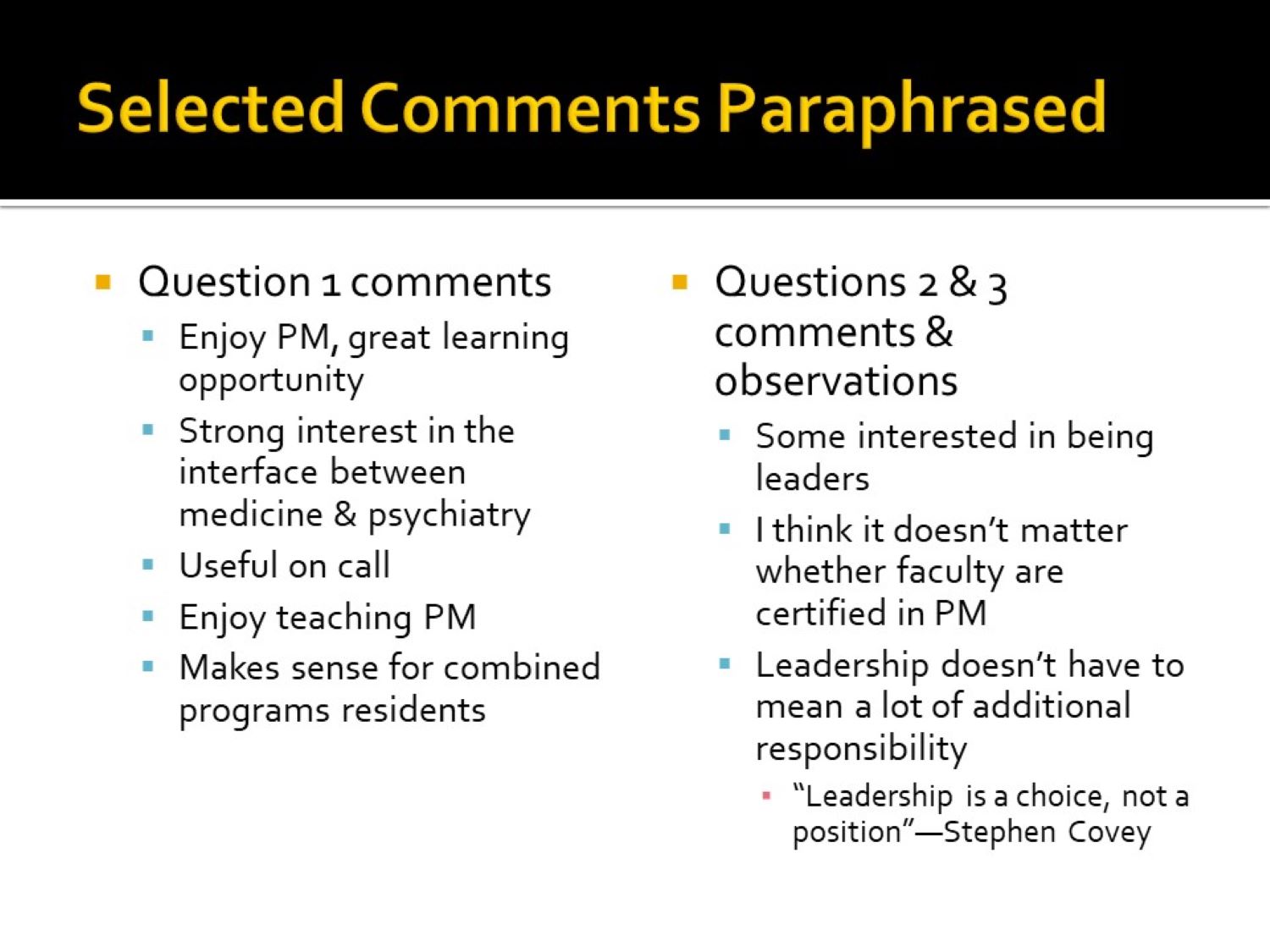
You’ll notice on slide 4 one faculty member’s comment, “I think it doesn’t matter whether faculty are certified in PM.” As Dr. Greenstein discovered, it probably does matter, at least if you want to be board certified.
I was initially certified by the American Board of Psychiatry & Neurology (ABPN), but I objected to the whole Maintenance of Certification (MOC) program, as did many other psychiatrists. I eventually declined to continue participating in the MOC process. However, I notice that the Delirium Clinical Module that I and a resident put together is still accessible on the ABPN website.
Although response numbers were low, there was clearly an interest in starting the interest group. There was also an incentive to reapply to the ACGME for approval of a Psychosomatic Medicine (Consultation-Liaison Psychiatry now) fellowship.
My attempt years earlier had been frustrating. While it was approved, I couldn’t attract any fellows, forcing me to withdraw it without prejudice (meaning another application for approval could be attempted). Fortunately, that situation changed later. The Psychiatry Department at The University of Iowa now has an early career C-L psychiatrist who graduated from the reinstated C-L fellowship.
As the saying goes, “What goes around comes around.” Although the origin of that saying might have originated in the 1970s, at least one person thought his grandmother had her own version in the 1950s: “You get what you give.”
We drove by Terry Trueblood Recreation Area today and were amazed by the big crowd of people. We found out about the NAMIWalkstoday because of the signage and people everywhere at the park.
The National Alliance on Mental Illness (NAMI) has been around since 1979, and you can read more from the top fundraiser for today’s event, Margalea Warner!
I was just googling the search terms “Black Psychiatrists in Iowa” and “African American Psychiatrists in Iowa” recently after finding a broken link in my 2019 blog post “Black Psychiatrists Iowa.”
I always think it’s funny that the results of my web search invariably show mainly a couple of mistakes. One is that I typically find my colleague, Dr. Donald Black, MD, a white male, misidentified as Black. The other mistake is that the search engine makes is confusing psychologists with psychiatrists, as though there were no difference. This happens every time, even nowadays in what many would call the era of wokeness.
The broken link was to what I thought was The 2018 Greater Iowa African American Resource Guide. I discovered the link leads to Iowa State University Diversity, Equity and Inclusion web page along with the “Page not found” notice. I could not find a 2018 issue of the guide on the web.
I found the 2019 guide, which showed that there were only two Black psychiatrists listed, me and Dr. Rodney J. Dean who founded the Dean and Associates psychiatry clinic in Sioux City, Iowa. I guess now there might be only one Black psychiatrist in Iowa.
I could not find later editions of the guide following 2019. I don’t know they were compiled or published by Kimberly Baxter, Director of the Iowa Accountability Program (IAP). According to the director, the guide was widely thought of as useful (see page ii of the guide). I wonder if the Covid-19 pandemic played some role in halting production of the guide.
However, I found a newsletter published (I didn’t see a date) on the Iowa Judicial Branch web page of Iowa Court dot gov web site, indicating the IAP was still active in domestic violence prevention programs. The IAP received a $900,000 continuation grant from the US Department of Justice, Office on Violence Against Women to continue court services for domestic violence victims. Thankfully, Kimberly Baxter is still active as Executive Director of Special Projects.
I don’t know if there will ever be another edition of The Greater Iowa African American Resource Guide. I think it did a better job of tracking how many Black psychiatrists there are in Iowa than Dr. Google ever did.
I’ve seen several articles on Medscape about how to convince doctors to retire or even force them to retire when they’re too old to practice. The articles are titled, “How Old Is Too Old to Work as a Doctor?”; “Are Aging Physicians a Burden?”; and “When Should Psychiatrists Retire?”
The Great Resignation almost makes the debates about this moot. Doctors, including psychiatrists, are retiring or quitting in droves because of burnout, largely related to the stress of the Covid-19 pandemic in the last two years. However, a lot of physicians were quitting medicine even prior to the pandemic.
The same arguments get trotted out. Doctors often lack insight into their failing cognition and physical health as they age. How do we respectfully assess and inform them of their deficits? Are there gentle ways to move them away from active medical, surgical, and psychiatric practice and into mentoring roles to capitalize on their strengths in judgment and experience?
The decision to persuade some doctors to retire, not so much because of advancing chronological age but because of dwindling cognitive capacity and other essential skills, needs to be handled with empathy and wisdom, especially if this is going to increase the workload for the rest of the doctors holding the fort.
Like the song says, “Break it to Me Gently.”
And speaking of songs, this doctor retirement discussion reminded me of a song I heard on TV when I was a kid. I could remember just one line, “Your Love is Like Butter Gone Rancid.”
I thought I heard it on an episode of an old TV sitcom, The Real McCoys. In fact, it was from a 1968 episode of the Doris Day Show called The Songwriter. Hey, we watched what my mom wanted to watch.
The song’s awful lyrics, which Doris Day “wrote” (only as part of the show; it was actually written by Joseph Bonaduce) were tied to the melody of “My Bonnie Lies Over the Ocean”:
Your love is like butter gone rancid,
It’s no good now, it’s started to turn,
I pray that it’s just like the man said,
You can’t put it back in the churn
Can’t put
Can’t put
Can’t put it back in the churn
Oh, durn!
You can’t put it back…in the churn
The context here is that another character (Leroy) in the show had previously submitted the lyrics of a similarly bad song (“Weeds in the Garden of My Heart”) to a crooked music publishing company that lavishly praised the song and promised to publish it—at Leroy’s expense.
Leroy was clueless about getting cheated. He was too dumb to know how bad the song was, but his feelings would have been badly hurt if the family just flatly told him that. They had to figure out a way to break it to him gently. So, Doris wrote the equally terrible “Your Love is Like Butter Gone Rancid,” and performed it for Leroy and the rest of the family. Leroy thought Doris Day’s song was garbage but didn’t know how to tell her without hurting her feelings.
Doris then told Leroy she was also going to submit her rancid song to the crooked publishing company.
After Doris got the exact same letter the crooked company sent to Leroy—he learned his lesson and felt supported, gosh darn.
Anyway, I was moved to write a short song about the doctor retirement issue, “When Doctors Are Too Old to Practice,” sung to the tune of “My Bonnie Lies Over the Ocean” of course:
When doctors are too old to practice
And can’t tell your elbows from knees
When they sing old songs to distract us
It’s high time we tell them to leave
High time
High time
It’s high time we tell them to leave
Oh, beans!
It’s high time we tell them…to leave
I’ve received hundreds of billions of requests for a sing-a-long version of “My Bonnie Lies Over the Ocean” because you can’t sing the parodies unless you know the original tune.
I was looking at an early version of the handbook of consultation-liaison psychiatry that eventually evolved into what was actually published by Cambridge University Press. I wrote virtually all of the early version and it was mainly for trainees rotating through the consult service. The published book had many talented contributors. I and my department chair, Dr. Robert G. Robinson, co-edited the book.
In the introduction I mention that the manual was designed for gunslingers and chess masters. The gunslingers are the general hospital psychiatric consultants who actually hiked all over the hospital putting out the psychiatric fires that are always smoldering or blazing. The main problems were delirium and neuropsychiatric syndromes that mimic primary psychiatric disorders.
The chess masters were those I admired who actually conducted research into the causes of neuropsychiatric disorders.
Admittedly the dichotomy was romanticized. I saw myself as a gunslinger, often shooting from the hip in an effort to manage confused and violent patients. Looking back on it, I probably seemed pretty unscientific.
But I can tell you that when I followed the recommendations of the scientists about how to reverse catatonia with benzodiazepines, I felt much more competent. After administering lorazepam intravenously to patients who were mute and immobile before the dose to answering questions and wondering why everyone was looking at them after the dose—it looked miraculous.
Later in my career, I usually thought the comparison to a firefighter was a better analogy.
The 2008 working manual was called the Psychosomatic Medicine Handbook for Residents at the time. This was before the name of the specialty was changed back to Consultation-Liaison Psychiatry. I wrote all of it. I’m not sure about the origin of my comment about a Psychosomatic Medicine textbook weighing 7 pounds. It might relate to the picture of several heavy textbooks on which my book sits. I might have weighed one of them.The introduction is below (featured image picture credit pixydotorg):
“In 2003 the American Board of Medical Specialties approved the subspecialty status of Psychiatry now known as Psychosomatic Medicine. Long before that, the field was known as Consultation-Liaison Psychiatry. In 2005, the first certification examination was offered by the American Board of Psychiatry and Neurology. Both I and my co-editor, Dr. Robert G. Robinson, passed that examination along with many other examinees. This important point in the history of psychiatry began many decades ago, probably in the early 19th century, when the word “psychosomatic” was first used by Johann Christian Heinroth when discussing insomnia.
Psychosomatic Medicine began as the study of psychophysiology which in some quarters led to a reductionistic theory of psychogenic causation of disease. However, the evolution of a broader conceptualization of the discipline as the study of mind and body interactions in patients who are ill and the creation of effective treatments for them probably was a parallel development. This was called Consultation-Liaison Psychiatry and was considered the practical application of the principles and discoveries of Psychosomatic Medicine. Two major organizations grew up in the early and middle parts of the 20th century that seemed to formalize the distinction (and possibly the eventual separation) between the two ideas: the American Psychosomatic Society (APS) and the Academy of Psychosomatic Medicine (APM). The name of the subspecialty finally approved in 2003 was the latter largely because of its historic roots in the origin of the interaction of mind and body paradigm.
The impression that the field was dichotomized into research and practical application was shared and lamented by many members of both organizations. At a symposium at the APM annual meeting in Tucson, AZ in 2006, it was remarked that practitioners of “…psychosomatic medicine may well be lost in thought while…C-L psychiatrists are lost in action.”
I think it is ironic how organizations that are both devoted to teaching physicians and patients how to think both/and instead of either/or about medical and psychiatric problems could have become so dichotomized themselves.
My motive for writing this book makes me think of a few quotations about psychiatry in general hospitals:
“Relegating this work entirely to specialists is futile for it is doubtful whether there will ever be a sufficient number of psychiatrists to respond to all the requests for consultations. There is, therefore, no alternative to educating other physicians in the elements of psychiatric methods.”
“All staff conferences in general hospitals should be attended by the psychiatrist so that there might be a mutual exchange of medical experience and frank discussion of those cases in which there are psychiatric problems.”
“The time should not be too long delayed when psychiatrists are required on all our medical and surgical wards and in all our general and surgical clinics.”
The first two quotes, however modern they might sound, are actually from 1929 in one of the first papers ever written about Consultation Psychiatry (now Psychosomatic Medicine), authored by George W. Henry, A.B., M.D. The third is from the mid-1930s by Helen Flanders Dunbar, M.D., in an article about the substantial role psychological factors play in the etiology and course of cardiovascular diseases, diabetes, and fractures in 600 patients. Although few hospital organizations actually practice what these physicians recommended, the recurring theme seems to be the need to improve outcomes and processes in health care by integrating medical and psychiatric delivery care systems. Further, Dr. Roger Kathol has written persuasively of the need for a sea change in the way our health care delivery and insurance systems operate so as to improve the quality of health care in this country so that it compares well with that of other nations (2).
This book is not a textbook. It is not a source for definitive, comprehensive lists of references about all the latest research. It is not a thousand pages long and does not weigh seven pounds. It is a modest contribution to the principle of both/and thinking about psyche and soma; consultants and researchers; — gunslingers and chess masters.
In this field there are chess masters and gunslingers. We need both. You need to be a gunslinger to react quickly and effectively on the wards and in the emergency room during crises. You also need to be a chess master after the smoke has cleared, to reflect on what you did, how you did it—and analyze why you did it and whether that was in accord with the best medical evidence.
This book is for the gunslinger who relies on the chess master. This book is also for the chess master—who needs to be a gunslinger.
“Strategy without tactics is the slowest route to victory. Tactics without strategy is the noise before defeat”—Sun Tzu.”
References:
1. Kathol, R.G., and Gatteau, S. 2007. Healing body and mind: a critical issue for health care reform. Westport, CT: Praeger Publishers. 190 pp.
2. Kornfeld, D., and Wharton, R. 2005. The American Psychiatric Publishing Textbook of Psychosomatic Medicine. Psychosomatics 46:95-103.