I was thinking about what to write for the first day of Black History Month, which starts today on February 1, 2023.
As usual, I started to reminisce about my time at Iowa State University (ISU) in Ames, Iowa. I usually don’t talk about my undergraduate days. In fact, I had a little trouble finding my diploma. It was in storage in the first place I should have looked. I graduated from ISU in 1985.
The Iowa State Daily ran a story, “Black scientists from Iowa State,” published on February 4, 2021, obviously in honor of Black History Month. Of course, it featured ISU’s most illustrious graduate, George Washington Carver, who earned his graduate degree in 1894. Carver also loved poetry and painting, which I didn’t know.
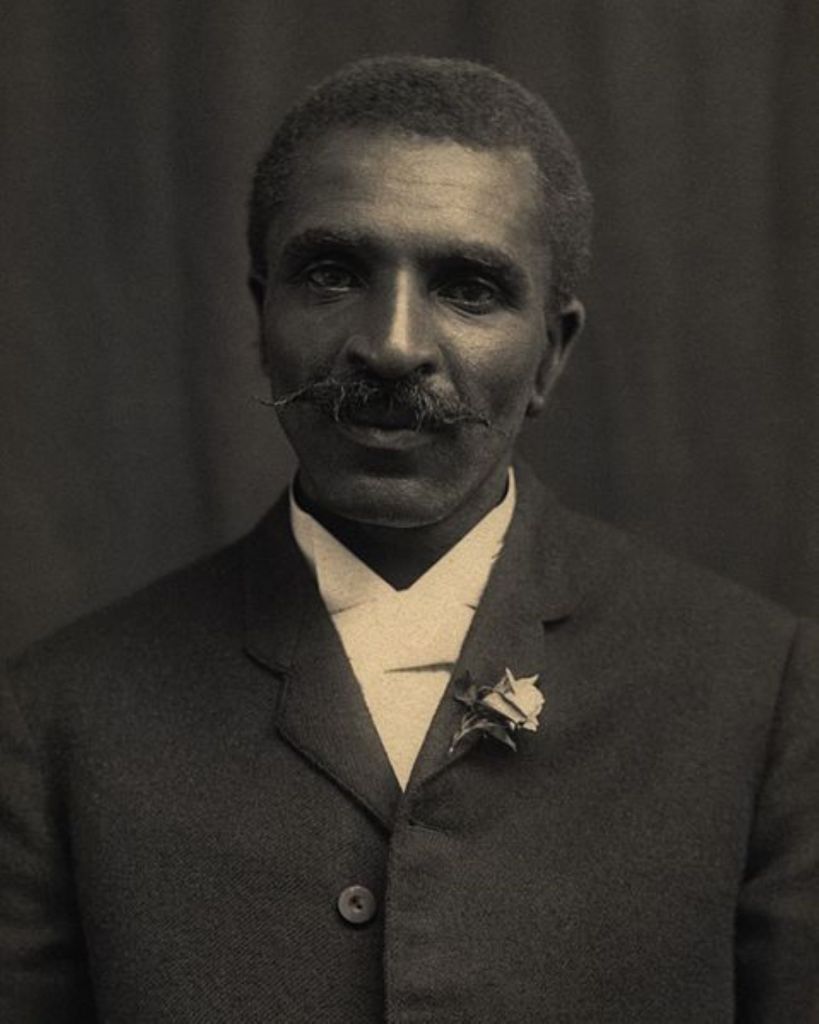
This work is in the public domain in the United States because it was published (or registered with the U.S. Copyright Office) before January 1, 1928
Carver was a scientist and put it to practical use. It fits with the ISU motto, which was short and to the point: “Science with Practice.”
I transferred credit to ISU in the mid-1970s from one of the country’s Historically Black Colleges and Universities (HBCUs), Huston-Tillotson College (now Huston-Tillotson University). I submitted a poem to the college’s annual student poetry contest sponsored by one of the English Professors, Dr. Jenny Lind Porter-Scott. My poem didn’t make the cut, but many students got their work published in the little book, Habari Gani (Swahili for “What’s Going On”), which published the best poems.
Part of the reason I went to ISU was the encouragement I got from my bosses at WHKS &Co, consulting engineers. I was a surveyor’s assistant and drafter. I was the only African-American employee working there.
The idea behind going to ISU initially was to pursue a degree in engineering. That didn’t happen because frankly, I didn’t have a head for the mathematics. On the other hand, I got interested in biology, chemistry, and zoology and finally ended up in medical school at The University of Iowa in Iowa City. The rest is history, as they say, which allows the usual cover up of a multitude of sins.
At the time Sena and moved to Ames in the early 1980s, it was a quiet little town, except during VEISHEA, an annual spring celebration on campus. The event got out of hand many times and it was finally banned in 2014.
Back in the days of George Washington Carver, African American students were not allowed to room with other students who did not have black skin on campus. By the time we moved to Ames, the most uncomfortable racial incident I can recall personally was being the butt of a “nigger” joke at a barbershop. I had to find another place to get my hair cut.
I still had a lot of science to digest at ISU after switching my major from engineering to the life sciences. I remember a chemistry professor who looked like the typical hippie who demonstrated how electrons get excited by stacking chairs on top of the counter in front of the chalkboard (which teachers were still using) and climbing to the top and nervously doing a shaky little dance showing what an excited electron he was. I think all of us collectively held our breath, waiting for him to tumble to the floor.
I really had a tough time learning organic chemistry. You had to draw diagrams showing how the molecules and atoms connected after each reaction. I will never forget an Asian Teacher’s Assistant who patiently tutored me, despite my having a very bad cold and a bad attitude to boot.
I graduated and then returned to get more credits to try getting into medical school after finding it very difficult to find employment with my Bachelor of Science degree. It took about 9 months before I finally landed a job in the clinical lab at one of the hospitals in Des Moines. The lab director worked there for a very short time while I was there, and then left to go to medical school.
That was my cue. I think it worked out for the best. By the way, the engraved crystal in the featured image is an appreciation gift from The University of Iowa for my years of service.
And I guess that’s about enough reminiscence for now.