The Afro-American Cultural Center in Iowa City has many activities scheduled for Black History Month 2024. Check it out!
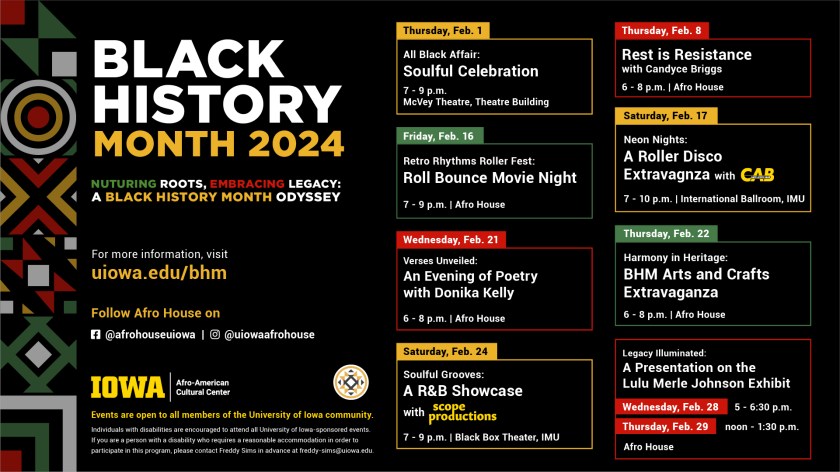

February is Black History Month and in 2024 the theme is African Americans and the Arts.
This reminds me of a blues artist I heard on KCCK on the Big Mo Blues Show last Friday. His name is Toronzo Cannon and his career as a blues guitarist and songwriter is skyrocketing. I heard his song “The Preacher, the Politician, and the Pimp.”
The lyrics reminded me of a character (or maybe more properly a non-character) called Rinehart in Ralph Ellison’s book, Invisible Man. I’m by no means an Ellison scholar but in chapter 23 the main narrator gets mistaken for a black guy named Rinehart who has many faces in the black community. He’s a preacher, a numbers runner, a pimp, and is also related to a political movement in the novel. Rinehart is all of them and none of them, moving between the “rind and heart” of who black people are in America. The implication is that the identity of black people is multifaceted and the similarity of the theme in Toronzo Cannon’s song is striking.
Cannon is also multifaceted. He’s a Blues guitar star and song writer and is also still a bus driver for the Chicago Transit Authority. How does he find time to do all that?
I wonder if Cannon got the idea for the song from Ellison’s novel. I guess I’ll never know.
This reminds me of an encounter I had with a black writer at Huston-Tillotson University (then Huston-Tillotson College, located in Austin, Texas) in the 1970s when I was an undergraduate in college. I’ve described this episode before in another post (“Black Psychiatrists in Iowa” 2019). The excerpt below includes a reference to a book review I wrote that was published in The American Journal of Psychiatry over 20 years ago:
“This reminds me of a book review I wrote for the American Journal of Psychiatry almost 20 years ago (Amos, J. (2000). Being Black in America Today: A multi perspective review of the problem. Am J Psychiatry, 157(5), 845-846.).”
The book was written by Norman Q Brill, M.D. It reminded me of my experience at Huston-Tillotson College (now Huston-Tillotson University, a private school, historically with largely Black enrollment) in Austin, Texas back in the 1970s. I wrote:
“Dr. Brill’s appraisal of many black leaders in chapters such as “Black Leaders in the Black Movement” and “Black Anti-Semitism” may be refreshingly frank in the opinion of some. He tailors his prose so as not to denounce openly those whom many would describe as demagogues. At the same time, it is apparent that his underlying message is that a substantial number of them are not only out of touch with mainstream black America but may even mislead black people into adopting ideological positions that impede rather than foster progress. Dr. Brill’s description of the issue reminded me of my own experience with this phenomenon as a freshman in the mid-1970s at a college of predominantly black enrollment in the southern United States. A guest lecturer (who, as I recall, had also written a book about being black in America) told us that the white man would never allow a black man to be a man in America. He had only three choices: he could be a clown, an athlete, or a noble savage. These corresponded to the prominent and often stereotyped roles that blacks typically held in entertainment, sports, and black churches.”
I was taken aback by the speaker’s judgment and asked him what my choice should then be. He was equally taken aback, I suspect. He advised me to be a clown.
The lyrics of Cannon’s song “The Preacher, The Politician, and the Pimp,” Ellison’s Rinehart, and another writer’s characterization of the roles allowed in American society for black men all resonate together. What drives the similarity of this perception across different artistic platforms?
When I reflect on how I’ve negotiated my life’s path over they years, I guess I would have to admit that I’ve often played the clown. Anyone can see that in the way my sense of humor comes across. Is it the healthiest way to respond to racism in this country? In terms of the psychological defense mechanisms, I think it’s a relatively mature strategy. You could argue with that by asking, “But where’s the maturity in dad jokes?”
Hey, it worked for Dick Gregory:
“I’ve got to go up there as an individual first, a Negro second. I’ve got to be a colored funny man, not a funny colored man”—Dick Gregory.
Dick Gregory
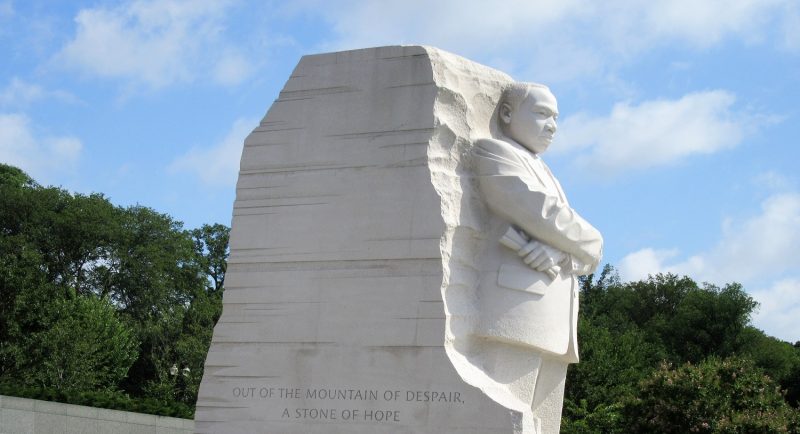
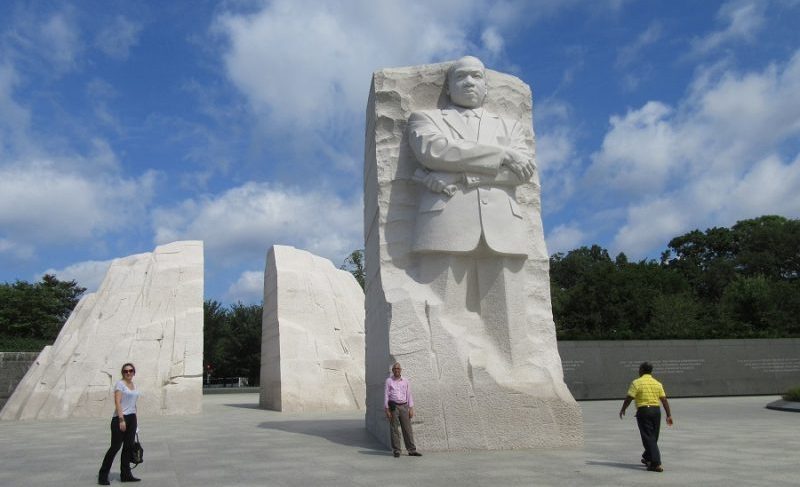
I noticed that Iowa City and Huston-Tillotson University in Austin, Texas have a couple of things in common regarding the celebration of the Martin Luther King holiday this week—one is inclement weather. The other thing is hope for peace and unity.
I was a student at Huston-Tillotson (one of the HBCUs) back in the 1970s. I saw it snow there once. It turns out that one of the MLK events will be postponed to January 27, 2024, and that’s the Austin MLK March. It’ll be too cold, with a chance for freezing rain. The event is billed as the MLK CommUnity March. The MLK Festival and Food Drive has been rescheduled to January 27th as well, and that will be at Huston-Tillotson University. The emphasis is on unity.
In Iowa City, the MLK Peace March on January 15, 2024 will instead be a vehicular parade because of the really cold weather we’ve been having recently. The emphasis is on peace. The parade will start at 9:30 AM.
All of my life I’ve admired Dr. Martin Luther King for his efforts to unite everyone in peace. Despite the world’s current events, I still have hope that the effort will continue.
We all have a lot in common, and it’s not just the weather.
I finally watched the movie “The Hitchhiker’s Guide to the Galaxy” the other night. It was released in 2005 and based on Douglas Adams’ book of the same title. In fact, he co-wrote the screenplay. A lot of it was not in the book. I thought a couple of scenes were noteworthy and pretty funny. I made connections to Dr. Martin Luther King, Jr. annual observance, which is this month.

One of them was the Point of View Gun. It’s probably unfortunate that the main prop was a gun, but hey, it was a ray gun. It didn’t kill anyone and in fact, it caused the person “shot” with it to be able to understand the perspective of another person. It was just temporary, but for a short while it enabled persons or extraterrestrials to understand another’s point of view. It was designed by the Intergalactic Consortium of Angry Housewives to influence their husbands to understand them better.
One of Dr. Martin Luther King’s main points was how important it is to try to understand and validate someone else’s point of view.
One drawback of the Point of View gun (besides the obvious associations with gun violence) was that the effect was specific to whoever was using it. So, when the ultra-maladjusted robot Marvin mowed down a gang of Vogons (hideous and cruel extraterrestrial bureaucrats who destroyed Earth in order to make room for an intergalactic bypass), they all collapsed from depression.
The other scene I thought was funny was the Vogon planet’s slap-happy encounter between the heroes and the creatures shaped like spatulas that popped out of the ground and smacked anyone in the face who had an idea.
I didn’t think the movie was nearly as good as Adams’ book. But I wonder if you could cross the spatula creatures with the Point of View gun that would take the perspective-taking power of the gun and give it to the spatula creatures who would slap you silly whenever you failed to even try to understand another’s point of view. I could use that kind of a slap sometimes.
It’s remarkable the connections you could make between Dr. Martin Luther King, Jr and The Hitchhiker’s Guide to the Galaxy.
Sena and I got to talking about a Twilight Zone show we saw over the holidays. It was a 1964 episode, not the regular program but short film that won a Cannes Film Festival award in the early 1960s, “An Occurrence at Owl Creek Bridge.”
The quick summary is that a Southern plantation owner is being hanged by Union soldiers for trying to set fire to the bridge to prevent the Union Army from attacking Confederate troops. The plantation owner seems to miraculously escape the noose, evades bullets and cannon fire, running all the way back to his plantation in an escape which lasts hours, finally almost rushing into his wife’s arms—but he can’t because at that moment his neck is snapped by the hangman’s rope. All of the action during his escape is a hallucination which happens in the blink of an eye.
It’s based on a short story of the same title by Ambrose Bierce. I vaguely recalled reading it years ago, possibly in a science fiction/fantasy anthology. At that time, I didn’t know the author’s background, which was that he’d been a Union soldier in the Civil War. He fought in a lot of battles and witnessed horrific injuries and death. He disappeared without a trace, and there is no explanation why or how.
As Sena and I talked about it, she wondered more about the details of the Civil War as context, while I thought the main point was about the time compression of a miraculous escape from execution that spoke of the nature and meaning of life and death.
When I searched the web to find out more about the story and the life of Ambrose Bierce, I saw her point.
I read the original story on the Internet Archive. It’s very short. Now, I’m not sure I ever really read it. I’m just a blogger and unworthy to really talk about it other than to acknowledge that it’s a work of genius. How the author’s spare and yet meticulous attention to every terrifying detail of war can be so ugly and yet so mesmerizing is beyond my understanding.
I found one of my old blog posts about using intravenous infusions of haloperidol for delirium in the intensive care unit. The bottom line is it that it probably should not be used, in my opinion. This is sort of a follow up on my Christmas Eve blog post in which I mention talking to ICU personnel about using IV haldol for delirium. I’ve edited out a portion of the old post.
Notes on Pharmacology for the Treatment and Prevention of Delirium: IV Haldol Infusions
“I ran across the Canadian Coalition for Seniors’ Mental Health guidelines for the management of delirium in elder adults. You can access them for free at the at this link, CCSMH – Canadian Coalition for Seniors’ Mental Health. I was a bit surprised to read the following recommendation:
“For those who require multiple bolus doses of antipsychotic medications, continuous intravenous infusion of antipsychotic medication may be useful.“
Note: I read this in 2011. I’ve rechecked the website of CCSMH, which shows the same recommendation when I reviewed it on December 27, 2023.
The recipe for continuous infusion of haloperidol was in a paper by Riker and I thought it was of historical interest[1]. Essentially, if the delirious patient had not responded to 8 consecutive 10mg bolus injections of haloperidol, you asked the intensivists to start a haloperidol drip at 10mg an hour. It usually didn’t work and despite the puzzling tendency for experts to claim that extrapyramidal side effects (EPSE) such as dystonias, parkinsionism, and akathisia occur at a lower rate when haloperidol is infused intravenously, the dissenting opinion from experienced psychiatric consultants including me is—if you do this enough times you’ll see EPSE. I’ve witnessed everything from trismus to opisthotonos, on one occasion all in one patient as I stood there and watched him over minutes while the intravenous (IV) haloperidol was infusing.
The idea that IV haloperidol infusions seems to stem in part from a 1987 paper by Menza[2]. There were only 10 patients total in that study.
My comments: I remember a presentation at an Academy of Consultation-Liaison (ACLP) meeting many years ago reporting that EPS (extrapyramidal side effects such as dystonia) had been reported to occur after IV administration in 67% of normal humans given a single dose, in 16-74% of adults with medical illness including burns, migraine, and Human Immunodeficiency Syndrome, and in 37% of psychiatric inpatients. EPS occured after IV administration of other dopamine blockers including the anti-nausea agent Reglan and there were at least 6 case reports of Neuroleptic Malignant Syndrome (the “ultimate EPS”) following IV administration of haloperidol.
The presenter reporter that no EPS occurred in several cases of reported very high dose IV Haloperidol, e.g., 945mg/ in 24 hours; and 1155mg in one day (from his own case report in 1995). It may have had something to do with delirium itself being a highly anticholinergic state.
There have been improvements in the management of delirium in the ICU since then. The best example I can give would be what Dr. Wesley Ely, MD has been doing for years at Vanderbilt.
1. Riker, R.R., G.L. Fraser, and P.M. Cox, Continuous infusion of haloperidol controls agitation in critically ill patients. Crit Care Med, 1994. 22(3): p. 433-40.
2. Menza, M.A., et al., Decreased extrapyramidal symptoms with intravenous haloperidol. J Clin Psychiatry, 1987. 48(7): p. 278-80.