The JAMA network published a brief report on the new CDC campaign to help health care workers reduce burnout and encourage well-being. An excerpt:
“Rather than focusing on what individual clinicians can do differently to improve their well-being, a new campaign by the National Institute for Occupational Safety and Health (NIOSH), part of the US Centers for Disease Control and Prevention, aims to reduce health care worker burnout by encouraging hospital leaders to implement organizational changes and offering them tools to do so.”
Yesterday we got the new aerobic step platform for cardiovascular health enhancement exercise. As I reported in October, climbing stairs can be very helpful in promoting cardiovascular health. This article summarizes the findings. At least 5 flights (around 50 steps of 10 stair steps) is said to be beneficial.
I climbed a lot of stairs in my career as a consulting psychiatrist in an 800-bed hospital. I don’t do anything close to that now, but I exercise pretty much daily. It limits my wardrobe.
My step counter app will track my stair step climbing on regular stairs in our house. However, it won’t count the steps I do on the step platform. It doesn’t really matter. I count everything else I do when I exercise, even on my anti-Peloton stationary bike, since the digital computer for monitoring my fitness level never worked. I also count the number of throws when I practice the 3-ball cascade juggling pattern (a hundred, often with 2 or 3 different sets of balls).
You can adjust the height on the platform by using risers, which can go up to 8 inches. That’s the usual height of the risers on regular stairs.
It’s not a Stairmaster by any means—but then it doesn’t cost $3,000 either.
I’ve been having a runny nose recently that is intermittent and often related to eating hot foods. I have to get up from the dinner table and blow my nose, especially if we’re having hot soups or chili. I’ve been making fun of it, saying it’s caused by the nasal hair condensation index. You could also refer to it as Darned Rhinorrhea Interrupting People (DRIP). I looked it up on the internet and getting a runny nose is pretty common when eating and after other activities. It can happen just from getting older.
It turns out that there is a connection to eating certain kinds of hot and spicy foods called gustatory rhinitis. I never had this problem until the past month or so.
Recently, I get this even while juggling. And there is something called exercise induced rhinitis. It’s been known for over a hundred years.
I always notice I have a drippy nose when I come in the house after shoveling snow. It’s just snow melting from my nose hairs.
But I never got a runny nose from eating chili until a month or so ago.
And I found out there’s this thing called geriatric rhinitis. It can be caused by a number of things like (hold on to your tissue!) gustatory rhinitis. There are a number of other common causes including allergies, certain medications, and extraterrestrial abduction. Those darned ETs are forever sticking implants in peoples’ noses. There is a tendency to believe geriatric rhinitis needs some kind of specific treatment, such as anticholinergic sprays, immunotherapy, and a nasal cork stopper implantation procedure under general anesthesia in the outpatient Ear, Nose, and Throat surgery center. It costs only $50,000 per nostril (not covered by most insurance). ENT surgeons use a device with an Artificial Intelligence module, which can detect the difference between your nose and your eye with 50% accuracy.
Jokes aside (for a fraction of a second), I’ll admit a thought crossed my mind (an infrequent event) that I might have a cerebrospinal fluid leak, which is caused by a tear in the meninges into the sinuses and nasal passages. The fluid is thin and clear. Nasal sprays don’t stop it and you should seek medical attention if you can’t remember your name or find chunks of cerebral cortex in your Kleenex.
This blog post does not constitute medical advice and if you have DRIP, you should contact your nearest Voodoo practitioner.
I’m giving a shout-out to a couple of child psychiatrists, one I know only from a blog, The Good Enough Psychiatrist. The other is an assistant professor in the University of Iowa Child Psychiatry Dept. I’ve never met her.
Since Jenna gives her name in the About Me section of her blog, I’m going to call her that because it’s easier. Jenna writes many thought-provoking posts, but I really admire the one titled “Amae.”
Dr. Ashmita Banerjee, MD wrote an essay titled “The Power of Reflection and Self-Awareness.” It’s published on line in the Mental Health at Iowa section of The University of Iowa web site.
As a relatively recently retired consultation-liaison psychiatrist who is also a writer, I feel a strong connection to them. In addition to being very glad that extremely talented persons are filling the ranks of a specialty which suffers from a serious manpower shortage, I get a big kick out of reading what really smart people write.
Here’s where a geezer retired psychiatrist starts kidding around. Jenna, a fellow blogger, is used to my habit of deploying humor, admittedly often as a defense. Dr. Banerjee doesn’t know me.
What is it about these essays that reminds me of the X-Files episode “Hungry”? It’s a Monster of the Week episode from the monster’s perspective. This monster looks like a human but sucks brains out of people’s skulls. He’s conflicted about it and even sees a therapist. But in the end his dying words were, as Agent Mulder shoots him down, “I can’t be something I’m not.”
If you read Dr. Banerjee’s essay and followed one of the links, you would have caught the clue that I actually read it because I consciously substituted the word “What” for “Why” in the previous paragraph. I could have as easily asked why instead of what—but it’s less helpful in gaining self-awareness.
And I haven’t sucked anybody’s brains out of their skulls in, what, over two weeks now! Upon reflection, I’m very aware of being incorrigible. Food for thought.
Jenna’s description of the Japanese concept of the word “amae” and Dr. Banerjee’s examination of the Japanese word “kintsukuroi” fascinated me. What made both writers consider human emotions using a language which captures the nuances so deftly?
I was a first-generation college student. There was a time in my life that a path to medical school seemed impossible. At times I probably thought I was trying to be something I’m not.
Sometimes I see news about Covid-19 variants. They typically sound alarming. The CDC has posted an update on Covid-19 variants that is reassuring. There will always be variants. Not all will be serious threats. According to the update:
“While new variants like BA.2.86 and JN.1 attract attention, right now, 99 percent of SARS-CoV-2 variants are part of the XBB group of the Omicron variant, which is what this year’s updated vaccines are based on. CDC is continuing to track the spread and impact of BA.2.86 and JN.1, as well as other variants as they come and go.
For as long as we have COVID-19, we’ll have new variants. Nearly all represent relatively small changes compared with previous variants. CDC and other agencies monitor for impacts of new variants on vaccines, tests, and treatments, and will alert the public quickly if anything concerning is detected. Most of the time, new variants make little to no impact.
Regardless of the variant, all SARS-CoV-2 viruses spread the same way. So it’s important to protect yourself and others by staying up to date with COVID-19 vaccines, improving ventilation and staying home when you’re sick.”
The latest update on how to get the respiratory viruses vaccines is updated on the CDC website. Highlights:
“f you have insurance, these vaccines should be free to you in most cases.
Adults without health insurance or adults whose insurance doesn’t cover all COVID-19 vaccine costs can get an updated COVID-19 vaccine for free through the Bridge Access Program.
How COVID-19 vaccines are being distributed changed in September 2023 when these products moved to the commercial market, but there is still plenty of vaccine supply.
Flu, COVID-19, and RSV vaccines may be given at the same visit.”
I ran across this article (reference below) on the potential benefit of climbing stairs for cardiovascular health. The highlights and abstract are below:
“Highlights
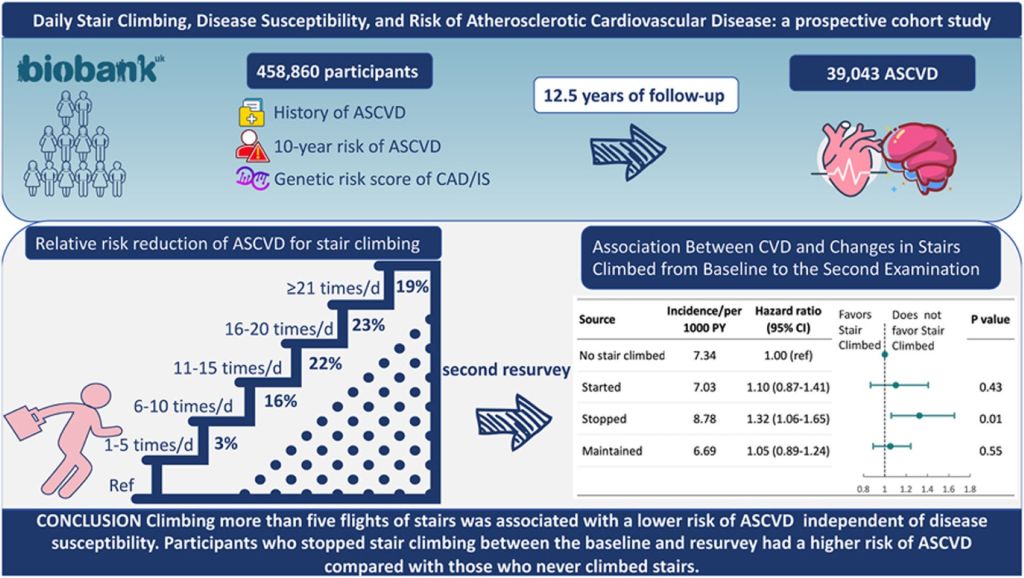
This large cohort of UK adults demonstrated that climbing more than five flights of stairs daily was associated with over a 20% lower risk of ASCVD.
The associations were broadly concordant in populations with varying susceptibilities to ASCVD.
Participants who discontinued stair climbing between the baseline and resurvey exhibited a higher risk of ASCVD in comparison to those who never engaged in stair climbing.
Abstract
Background and aims
The associations between the intensity of stair climbing and atherosclerotic cardiovascular disease (ASCVD) and how these vary by underlying disease susceptibility are not fully understood. We aim to evaluate the intensity of stair climbing and risk of ASCVD types and whether these vary by the presence of ASCVD risk factors.
Methods
This prospective study used data on 458,860 adult participants from the UK Biobank. Information about stair climbing, sociodemographic, and lifestyle factors was collected at baseline and a resurvey 5 years after baseline. ASCVD was defined as coronary artery disease (CAD), ischemic stroke (IS), or acute complications. Associations between flights of stair climbing and ASCVD were examined as hazard ratios (HRs) from Cox proportional hazards models. The modification role of disease susceptibility on such associations was assessed by analyses stratified by levels of genetic risk score (GRS), 10-year risks of ASCVD, and self-reported family history of ASCVD.
Results
During a median of 12.5 years of follow-up, 39,043 ASCVD, 30,718 CAD, and 10,521 IS cases were recorded. Compared with the reference group (reported climbing stairs 0 times/day at baseline), the multivariable-adjusted HRs for ASCVD were 0.97 (95% CI, 0.93–1.01), 0.84 (0.82–0.87), 0.78 (0.75–0.81), 0.77 (0.73–0.80) and 0.81 (0.77–0.85) for stair climbing of 1–5, 6–10, 11–15, 16–20 and ≥21 times/day, respectively. Comparable results were obtained for CAD and IS. When stratified by different disease susceptibility based on the GRS for CAD/IS, 10-year risk, and family history of ASCVD, the protection association of stair climbing was attenuated by increasing levels of disease susceptibility. Furthermore, compared with people who reported no stair climbing (<5 times/d) at two examinations, those who climbed stairs at baseline and then stopped at resurvey experienced a 32% higher risk of ASCVD (HR 1.32, 95% CI:1.06–1.65).
Conclusions
Climbing more than five flights of stairs (approx 50 steps) daily was associated with a lower risk of ASCVD types independent of disease susceptibility. Participants who stopped stair climbing between the baseline and resurvey had a higher risk of ASCVD compared with those who never climbed stairs.”
This interests me because I climbed well over 20 flights of stairs pretty much every day when I was a consultation-liaison psychiatrist. Occasionally, I logged over 40 flights. The hospital had 8 floors and I was often repeatedly hiking up the stairs. I avoided using elevators because they slowed me down too much.
There was a threshold effect of stair climbing in the study, meaning the benefit was lost if you went over a certain number of “floors.” Going over 15 or 20 didn’t gain much for subjects. A flight was 10 stair steps.
I think the idea is that in those who live in homes with the right number of stair steps, you’ve got a no cost, low tech form of cardiovascular exercise. You might exert a little more stress on the carpet.
On the other hand, you could save wear and tear on the carpet (if you’re worried about it) by spending some money on stair stepping exercise equipment. You can buy a Stairmaster model for about $2.000-3,000. There are cheaper stair stepper models, which look a little flimsy and even unstable enough to raise the risk for falls, in my view.
But I would never go back to work just to climb the stairs again.
Reference:
Song Z, Wan L, Wang W, Li Y, Zhao Y, Zhuang Z, Dong X, Xiao W, Huang N, Xu M, Clarke R, Qi L, Huang T, Daily stair climbing, disease susceptibility, and risk of atherosclerotic cardiovascular disease: A prospective cohort study, Atherosclerosis (2023)