The Moderna corporation announced in June 2023 that it filed for FDA authorization of its monovalent XBB. 1.5 vaccine.
Pfizer also announced the same message in August. It’s on page 4 of the Pfizer Earnings Call.

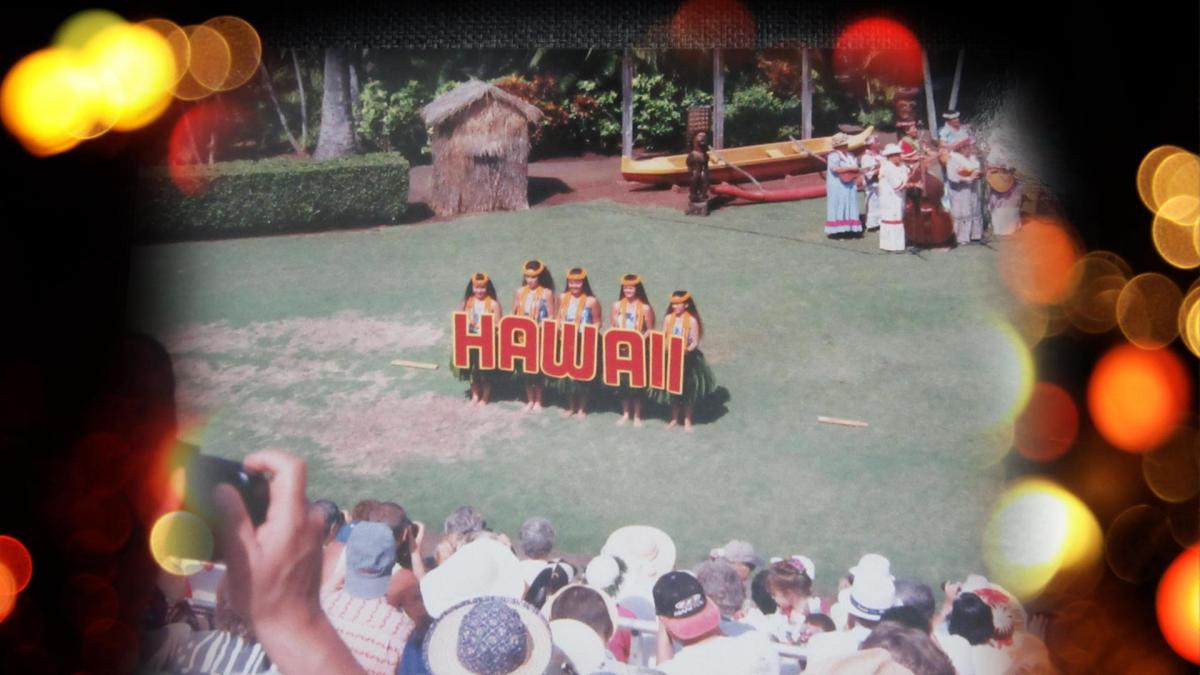
The wildfires in Maui are so devastating. We wish everyone the best. We also had a wave of nostalgia back to 1997 when we visited the Hawaiian Islands on our first vacation in a long while after I finished my psychiatry residency in 1996.
The plane trip was very long and what I remember most about it, flying all the way from Iowa, was the terrible case of bilateral airplane ear which lasted for a couple of hours after we landed in Honolulu. After that, things got a lot better. It was a long time ago, so the memories are a little hazy.
We remember the bus from the airport stopped at the hotel where the tour guide got out to check the reservations for all of us. It was very hot because the bus driver didn’t want to let the vehicle run so as to allow the air conditioner to cool us off. We were probably the youngest members of the tour group. It was the oldest who complained the loudest, finally convincing the bus driver to start the bus to cool everybody off.
After we arrived at the hotel, it was also the oldest members who had the energy to go out and see Don Ho perform. When they got back, they said he got drunk, but he was able to sing “Tiny Bubbles.” We were too exhausted to go. The oldest group members were often the most energetic.
We went a great little restaurant in either Kauai or maybe it was in Hilo, Hawaii (the Big Island) and got plates of huge shrimp. They were shorthanded on servers and several members of the tour group (again the older ones) pitched in to help out.
We saw the Kodak Hula Show in Honolulu on the island of Oahu. I read a little about it and the show nearly closed in 1999, but it was taken over by the Hogan Family Foundation for three years at a cost of half-million dollars per year. The show closed in 2002 so that the money could be used to fund educational programs.
Of course. we also visited the USS Arizona Memorial at Pearl Harbor. One of our tour group members who was a veteran of that war wept as he read the names. We became friends with him and his wife and sent each other Christmas cards for a few years afterward.
We saw the Hawaii Tropical Botanical Gardens in Hilo, Hawaii. It’s huge. It was a tribute to the Japanese immigrants to The Big Island who helped build its agricultural history beginning in 1868.
We visited the Wailua River State Park Fern Grotto Area and the Waimea Canyon in Kauai. The latter is also known as The Grand Canyon of the Pacific. I think Kauai was where I first tried coffee-flavored ice cream—Kona coffee, I’m sure. It remains one of my favorites, next to plain vanilla.
We got a few photos of the Iao Needle in the Iao Valley on Maui. We went to a big luau, but I can’t remember exactly where it was. I remember I was coming down with a head cold and had a runny nose. We tried poi, and I’m afraid I didn’t find it very tasty—and it had nothing to do with cold. Maui was the final island to see on our itinerary. I think we saw the huge Banyan Tree in Lahaina because we have a picture of a very large tree with Sena standing in front of it.
The 150-year-old Banyan Tree was charred in the fire, but it’s still standing.
I just saw the news story about the whistleblower David Grusch a couple days ago. Apparently, Mr. Grusch’s personal medical record was obtained through the state of Virginia’s Freedom of Information Act (FOIA) and released to the public. He was one of three people who testified recently at the House Oversight Committee hearing on Unidentified Anomalous Phenomena (UAP). He reported that the Department of Defense (DoD) had knowledge of extraterrestrial craft and “biologics” (extraterrestrial bodies?).
This reminds me of one of the final comments by one of the other three witnesses, which is worth framing as a quote:
“Don’t make the fish bigger than it was.” — retired Commander David Fravor of the U.S. Navy.
The current director of the DoD organization for UFOs, Sean Kirkpatrick, PhD, who heads the All-Domain Anomaly Resolution Office (AARO), expressed his objection in no uncertain terms to Mr. Grusch’s testimony, calling it insulting.
Anyway, I had to learn a little bit more about the FOIA, and found out that in addition to the federal government FOIA, each state has its own FOIA process. I looked up the Virginia state FOIA, and usually personal medical records are one of the exempted files. Apparently, they can still release them.
I think this might be an attempt to discredit Mr. Grusch. I’m puzzled by the release of his medical history. I don’t know anything about specific protections for retaliation against whistleblowers, but I would think exposing anyone’s medical record would count.
Not to spread any more conspiracy theories, but what if this whole thing is a well-orchestrated complex distraction from the general shambles of our political system? It would tend to discourage other whistleblowers from coming forward. Maybe that’s the intent.
If politicians and people in general were to make a concerted effort to treat each other with civility, respect, and a sense of humor, maybe these embarrassing sideshows could be minimized.
I don’t know if UAP involve advanced civilizations from across the galaxy and I doubt it. In fact, I tend to think a quote from Men in Black would fit:
“Human thought is so primitive it’s looked upon as an infectious disease in the better galaxies.”
I’m pretty sure most ETs have been steering clear of us for a long time.
How about this: the Iowa State Fair is on now, and it runs from August 10-20. I haven’t checked this out with anyone at the Fair, but if we could persuade David Grusch and Sean Kirkpatrick to settle their differences by competing in one or more of the contests coming up in the coming week, we might be able to get them to shake hands and have some laughs. Sena and I have never been to the Iowa State Fair, but if this event could be added, I think we could swing a trip there.
I see that the Cow Chip Throwing contest is scheduled for August 16 at 11 a.m. That would be a knee slapper.
It’s too late to arrange for them to compete in the Monster Arm Wrestling contest, which is this Sunday. Could a special event be scheduled later?
How about a cribbage game? The Cribbage Tournament is on August 20, starting at 10 a.m. with registration and the games start at 11 a.m. Now that would be special since Sena and I are fans of the game. David and Sean would have to learn how to play cribbage ahead of time, and it’s not that hard.
There are other events, but the guys need to get ready and decide soon so they can enter. And they should notify me so that Sena and I can make the trip to Des Moines and catch the action.
Both winner and loser should get free corn dogs.
We finished our Census Bureau survey and it seems like we just did this not long ago. It’s taken every 10 years but it seems like we got this form a few years ago.
They say it takes about 40 minutes to complete, but it sure felt like there were many more questions on it this time and the questions asked about a lot of things like income, taxes, etc. that we don’t remember from before.
Did anybody else get this feeling? I mean we really had to do things like get data from records and do math and sweat the details.
We asked ourselves what would happen if we just refused to do it. So, I looked it up. It turns out that there is a $5,000 penalty the bureau can impose if you refuse to do it or give false information.
On the other hand, Census Bureau officials have said nobody’s been prosecuted since 1970. I wonder what happened to that person? Is he still paying off the fine? Is he in jail because he couldn’t pay it? Was he abducted by extraterrestrials and is he still trying to get them to pay it?
There are other questions I had that led me to search the web. It looks like the best place to start might be the Census Bureau website itself. The section Census Bureau 101 for Students looks like a good place to start. The census has been around since 1790 and back then it was only a six-question survey:
What is your gender? (There are more choices nowadays)
What is your race? (It was not the 40-yard dash)
What is the name of the head of the household? (It’s always the wife!)
What is the relationship to the head of the household? (It’s always the husband!)
How many slaves do you own?
What is your occupation? (Tea party activists didn’t count)
There’s an interesting section on the web site PRB, entitled “Hard-to-Count Populations.”:
Decades of research have shown that the decennial census is very accurate, but (like population censuses in other countries) it is subject to both undercount and overcount errors that differ by age, sex, and race. The 2010 Census was no exception. Despite the best efforts and careful planning of Census Bureau staff, the direct, physical enumeration of the U.S. population is imperfect.
Part of the challenge in counting the population accurately is that some people are harder to count than others. People who lack a permanent address are less likely to complete a census form than people who have a permanent address. Similarly, language barriers, distrust of government, and frequent moves tend to make certain groups harder to count. On the other side of the spectrum, some people may be counted more than once. For example, those who own more than one home may submit a census form for each address, and children away at college may be counted at both their college and parental home.
If you decide not to complete the Census Bureau survey, they probably won’t fine you or throw you in jail. They could visit your house up to six times though. And if you manage to slip them every time, they could check with your neighbors to get the skinny on you.
You might as well do it.
Sena and I saw a news video about a technology called “DAX” which uses Artificial Intelligence (AI) the other day which promises to reduce or even eliminate pajama time for physicians trying to get their clinical note dictations done during the day instead of taking them home for several more hours of work.
The video was a demo of the technology, which looked like it recorded a clinical interview between the doctor and the news reporter. I didn’t see how exactly DAX was recording the interview without obvious audio equipment. Was it doing it through the smartphone speaker? This was very different from how I and many other clinicians dictated their notes using a headphone set at their desks in front of their desktop computers. It not only records but transcribes the interview.
Later, I discovered that DAX stands for Dragon Ambient Experience, made by Nuance which was acquired by Microsoft in 2022. I posted about Dragon products and their limitations last year. The product often produced hilarious mistakes during dictation which required careful editing. Sometimes more errors turned up after you completed it and these were visible in the patient’s medical record, which would then need to be corrected.
Several years ago, I remember talking to somebody from Dragon on the phone about the problems I was having. She was a little defensive when I told her I’d been having difficulty with Dragon for quite a while because it made so many mistakes.
A recent article on the web revealed that the errors continue with DAX. According to the article, “…it will make mistakes. Sometimes it might omit clinical facts; sometimes it may even hallucinate something.” I remember trying to communicate with the Google Bard AI, which seemed to do this pretty often. It made stuff up.
DAX is not cheap. The article reveals that one hospital pays $8,000-$10,000 per year per physician to use it. And skeptics worry that the system has too many bugs in it yet, which can lead to bias and inaccurate information which could negatively affect patient outcomes.
A recently published JAMA network article also urges caution in adoption of this sort of AI-assisted technology (Harris JE. An AI-Enhanced Electronic Health Record Could Boost Primary Care Productivity. JAMA. Published online August 07, 2023. doi:10.1001/jama.2023.14525).
In this case, I think it’s appropriate to say “I told you so.”
I got a pang of anti-nostalgia after reading the latest article calling for abolition of Maintenance of Certification (MOC), posted by Medscape on August 1, 2023. There is a petition by oncologists to end MOC. So, what else is new? So far it has almost 10,000 signatures.
I remember my own petition in 2014 to end the American Board of Medical Specialists (ABMS) attempt to establish Maintenance of Licensure (MOL), a kissing cousin of MOC, which would have blocked physicians from getting a state medical license if they didn’t comply with MOC requirements. It was supported by both the Iowa Psychiatric Society and the Iowa Medical Society. It got a lot of signatures and many comments in support of opposing both MOC and MOL. The glaringly obvious motive by member boards to require MOC is money and always has been, in my opinion.
I’m baffled at why this debate still rages on. It looks like almost no progress has been made in the last decade, apparently because the American Board of Internal Medicine (ABIM) and other boards ignore the clear messages from rank-and-file doctors about how MOC actually interferes with efforts to pursue practical continuing medical education.
I have always been a staunch supporter of physician-led continuing medical education. At the hospital where I worked as a consultation-liaison psychiatrist, the consult service ran the Clinical Problems in Consultation Psychiatry (CPCP). It was a weekly case-based conference, which I have written about in a 2019 post.
Ironically, the Performance in Practice (PIP) delirium clinical assessment tool module that I and one of the residents created is still offered for credit on the American Board of Psychiatry & Neurology continuing education web site. I think it demonstrates the ability of individual doctors to establish practical methods for developing their own continuing education programs.