There’s something embarrassing yet fascinating about reading my old blog posts from years ago. The one I read yesterday is titled simply “I Remember HT Heroes.” I make connections between my undergraduate college days at Huston-Tillotson College (now Huston-Tillotson University (an HBCU in Austin, Texas) and my early career as a consultation psychiatrist at The University of Iowa Hospitals & Clinics (now rebranded to Iowa Health Care).
My first remark about getting mail from AARP reminds me that organization is sponsoring the Rolling Stones current tour, Hackney Diamonds. And the name of my specialty was changed from Psychosomatic Medicine to Consultation-Liaison Psychiatry in 2017.
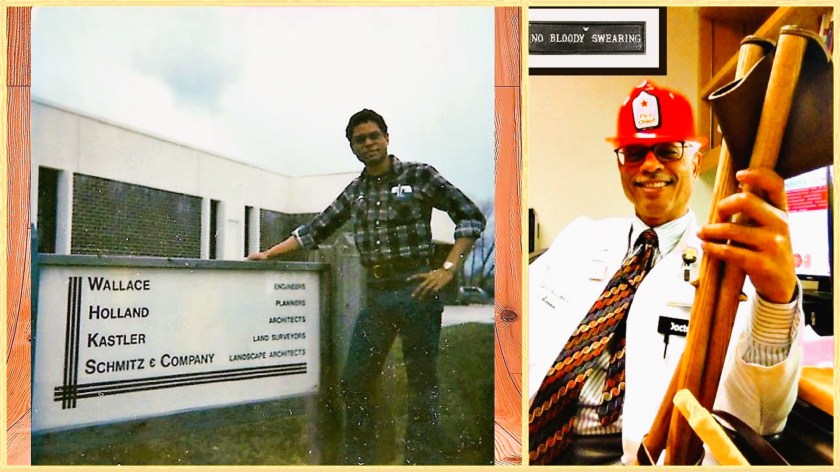
The photo of me attached to the original post reminds me of how I’ve gotten older—which also makes me hope that I’ve gotten wiser than how I sound in this essay. The pin in my lapel is the Leonard Tow Humanism in Medicine award I received in 2006.
I Remember HT Heroes
Getting membership solicitations in the mail from the American Association of Retired Persons (AARP) is a sure sign of aging, along with a growing tendency to reminisce. Reminiscence, especially about the seventies, may be a sign of encroaching senility.
Why would I reminisce about the seventies? Because I’m a baby boomer and because my ongoing efforts to educate my colleagues in surgery and internal medicine about Psychosomatic Medicine, (especially about how to anticipate and prevent delirium) makes me think about coming-of-age type experiences at Huston-Tillotson College (Huston Tillotson University since 2005) in Austin, Texas. Alas, I never took a degree there, choosing to transfer credit to Iowa State University toward my Bachelor’s, later earning my medical degree at The University of Iowa.
Alright, so I didn’t come of age at HT but I can see that a few of my most enduring habits of thought and my goals spring from those two years at this small, mostly African-American enrollment college on what used to be called Bluebonnet Hill. I learned about tenacity to principle and practice from a visiting professor in Sociology (from the University of Texas, I think) who paced back and forth across the Agard-Lovinggood auditorium stage in a lemon-yellow leisure suit as he ranted about the importance of bringing about change. He was a scholar yet decried the pursuit of the mere trappings of scholarship, exhorting us to work directly for change where it was needed most. He didn’t assign term papers, but sent me and another freshman to the Austin Police Department. The goal evidently was to make them nervous by our requests for the uniform police report, which our professor suspected might reveal a tendency to arrest blacks more frequently than whites (and yes, we called ourselves “black” then). He wasn’t satisfied with merely studying society’s institutions; he worked to change them for the better. Although I was probably just as nervous as the cops were, the lesson about the importance of applying principles of change directly to society eventually stuck. I remember it every time I encounter push-back from change-resistant hospital administrations.
I’m what they call a clinical track faculty member, which emphasizes my main role as a clinician-educator rather than a tenure track researcher. I chose that route not because I don’t value research. Ask anyone in my department about my enthusiasm for using evidence-based approaches in the practice of psychiatry. I have a passion for both science and humanistic approaches, which again I owe to HT, the former to Dr. James Means and the latter to Dr. Jenny Lind Porter. Dr. Means struggled to teach us mathematics, the language of science. He was a dyspeptic man, who once observed that he treated us better than we treated ourselves. Dr. Porter taught English Literature and writing. She also tried to teach me about Rosicrucian philosophy. I was too young and thick-headed. But it prepared the way for me to accept the importance of spirituality, when Marcia A. Murphy introduced me to her book, “Voices in the Rain: Meaning in Psychosis”, a harrowing account of her own struggle with schizophrenia and the meaning that her religious faith finally brought to it.
Passion was what Dr. Lamar Kirven (or Major Kirven because he was in the military) also modeled. He taught black history and he was excited about it. When he scrawled something on the blackboard, you couldn’t read it but you knew what he meant. And there was Dr. Hector Grant, chaplain and professor of religious studies, and champion of his native Jamaica then and now. He once said to me, “Not everyone can be a Baptist preacher”. My department chair’s echo is something about how I’ll never be a scientist. He’s right. I’m no longer the head of the Psychosomatic Medicine Division…but I am its heart.
I didn’t know it back in the seventies, but my teachers at HT would be my heroes. We need heroes like that in our medical schools, guiding the next generation of doctors. Hey, I’m doing the best I can, Dr. Porter.