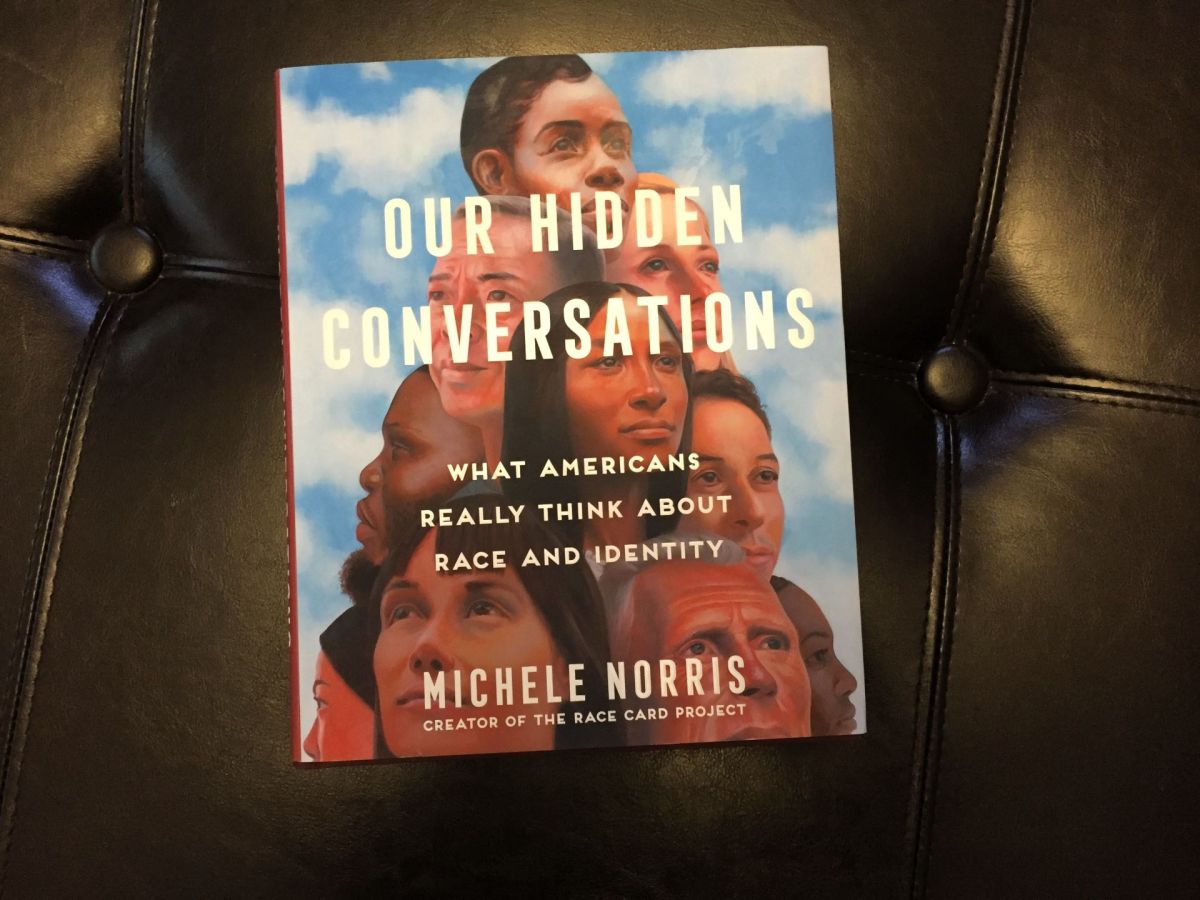
This is a short post about my initial impressions about the book, “Our Hidden Conversation” by Michele Norris.
I’m not finished with the book yet, but I thought I would let you know that the first chapter, “Bread Crumbs” was tough to read. I had to put it down and come back to it a few times because it brought back memories.
The chapter title “Bread Crumbs” means the clues that parents, grandparents, etc. might leave for subsequent generations to find which might shed light on one’s background, explain troubling circumstances, and so on.
I have some bread crumbs left to me by my family. Some are in the form of photos, although there is no family photo of all of us together.
I remember the hair combing routine my mom had with me and my brother every Sunday morning before church when we were kids. Our father was black and my mother was white. Dad was out of the home and we lived with mom. We were the only black kids in the church. In fact, all the members were white.
Mom used a prodigious amount of hair oil while vigorously combing our curly hair back. It took many strokes and the pulling pinched a bit. The ritual took a little while. When I look back on it, I guess the goal was to straighten our hair as much as possible.
Everyone in the church always treated us kindly and I was baptized there.
If you decide to read “Our Hidden Conversations,” give yourself a break whenever you feel like you need it.
I just started reading Michele Norris’s book, “Our Hidden Conversations.” It’s based on her Race Card Project, which has been going on for 14 years and counting. It’s about more than racism between black and white people. I’ll let you know what I think about the book from time to time.
Sena and I viewed a recording of the Dr. Martin Luther King, Jr Distinguished Lecture given by Michele Norris on January 23, 2023. It was not available to the general public, about which I have inquired. It was a very interesting, informative, and entertaining presentation. It was about her 14-year Race Card Project which led to her new book, “Our Hidden Conversations: What Americans Really Think About Race and Identity.”
Michele opened with a little information about Bayard Rustin, which we didn’t know. There’s a film titled “Rustin,” available on Netflix which is about him and Dr. King and their complicated relationship. He was a gay black man, which was difficult for the civil rights movement leaders to accept. He was the key organizer for the 1963 March on Washington for Jobs and Freedom.
In her own words, Ms. Norris created the Race Card Project because she thought no one wanted to talk about race. She found out she was wrong because there was an avalanche of response to her request that people write something about race on a small postcard (6 words) and send it back. Interesting examples:
“Father was racist. I’M NOT. Progress!”
“Did my Southern Grandpa attend lynchings?” (This card came from Iowa.)
“Married a white girl. Now what?” (The girl thought of the guy as an “assimilated” brown man.)
“Alabama. MLK assassinated. Students cheered. Horrified.” (This was in a college classroom.)
“We aren’t all strong, black women.” (Norris’s comment was that it makes black women seem more like a weed and not a flower).
“Two white dads. Three black kids.” (Adorable photo included of gay married men with three adopted black children.)
“Can someone help me find my privilege?” (Photo of a white man included. Ms. Norris said that most of the cards are from white people, which surprised her.)
“My name is Jamaal. I’m white.” (Include a picture of a white guy. This was a story about Iowa. The guy showed up for a job interview, and the receptionist says “I thought you would be taller.”)
“Vote for Obama. Look like me.” (White guy married to white gal; they adopted black girl. I think he meant, in the abstract, that no matter what color you or the candidate are you should vote based on whether the person is qualified for the job. It’s funny that his very young daughter commented on it in a predictably concrete way given her age. She said she lived in Iowa and didn’t see too many people who looked like her. Ms. Norris said this story would be included in the book.)
It’s tough to express complicated ideas in just six words.
Ms. Norris says it’s unlikely that we’re going to agree with each other. She wants to build bridges across the chasm which divides us and she is hopeful about our ability to do that. We ordered her book.
February is Black History Month and in 2024 the theme is African Americans and the Arts.
This reminds me of a blues artist I heard on KCCK on the Big Mo Blues Show last Friday. His name is Toronzo Cannon and his career as a blues guitarist and songwriter is skyrocketing. I heard his song “The Preacher, the Politician, and the Pimp.”
The lyrics reminded me of a character (or maybe more properly a non-character) called Rinehart in Ralph Ellison’s book, Invisible Man. I’m by no means an Ellison scholar but in chapter 23 the main narrator gets mistaken for a black guy named Rinehart who has many faces in the black community. He’s a preacher, a numbers runner, a pimp, and is also related to a political movement in the novel. Rinehart is all of them and none of them, moving between the “rind and heart” of who black people are in America. The implication is that the identity of black people is multifaceted and the similarity of the theme in Toronzo Cannon’s song is striking.
Cannon is also multifaceted. He’s a Blues guitar star and song writer and is also still a bus driver for the Chicago Transit Authority. How does he find time to do all that?
I wonder if Cannon got the idea for the song from Ellison’s novel. I guess I’ll never know.
This reminds me of an encounter I had with a black writer at Huston-Tillotson University (then Huston-Tillotson College, located in Austin, Texas) in the 1970s when I was an undergraduate in college. I’ve described this episode before in another post (“Black Psychiatrists in Iowa” 2019). The excerpt below includes a reference to a book review I wrote that was published in The American Journal of Psychiatry over 20 years ago:
“This reminds me of a book review I wrote for the American Journal of Psychiatry almost 20 years ago (Amos, J. (2000). Being Black in America Today: A multi perspective review of the problem. Am J Psychiatry, 157(5), 845-846.).”
The book was written by Norman Q Brill, M.D. It reminded me of my experience at Huston-Tillotson College (now Huston-Tillotson University, a private school, historically with largely Black enrollment) in Austin, Texas back in the 1970s. I wrote:
“Dr. Brill’s appraisal of many black leaders in chapters such as “Black Leaders in the Black Movement” and “Black Anti-Semitism” may be refreshingly frank in the opinion of some. He tailors his prose so as not to denounce openly those whom many would describe as demagogues. At the same time, it is apparent that his underlying message is that a substantial number of them are not only out of touch with mainstream black America but may even mislead black people into adopting ideological positions that impede rather than foster progress. Dr. Brill’s description of the issue reminded me of my own experience with this phenomenon as a freshman in the mid-1970s at a college of predominantly black enrollment in the southern United States. A guest lecturer (who, as I recall, had also written a book about being black in America) told us that the white man would never allow a black man to be a man in America. He had only three choices: he could be a clown, an athlete, or a noble savage. These corresponded to the prominent and often stereotyped roles that blacks typically held in entertainment, sports, and black churches.”
I was taken aback by the speaker’s judgment and asked him what my choice should then be. He was equally taken aback, I suspect. He advised me to be a clown.
The lyrics of Cannon’s song “The Preacher, The Politician, and the Pimp,” Ellison’s Rinehart, and another writer’s characterization of the roles allowed in American society for black men all resonate together. What drives the similarity of this perception across different artistic platforms?
When I reflect on how I’ve negotiated my life’s path over they years, I guess I would have to admit that I’ve often played the clown. Anyone can see that in the way my sense of humor comes across. Is it the healthiest way to respond to racism in this country? In terms of the psychological defense mechanisms, I think it’s a relatively mature strategy. You could argue with that by asking, “But where’s the maturity in dad jokes?”
Tomorrow’s schedule for the Martin Luther King Jr. Celebration of Human Rights Week has Michele Norris presenting the MLK Distinguished Lecture, “Our Hidden Conversations.” It’s based on her Race Card Project which produced her new book “Our Hidden Conversations: What Americans Really Think About Race and Identity.”
Sena and I probably are not going to make it to Michele Norris’s lecture tomorrow, mostly because of the bad weather.
The Race Card Project involved people sending in cards with just six words on it which described their experience with race and identity and much more than that. I didn’t learn of the project until this month.
If I were to send in a card, it would say, “Everyone changed but Jim.” What’s important about that is who said it, because it wasn’t me. It was somebody who was my best friend in grade school. I lost touch with Dan, who was white, for a while when we were kids.
When I caught up with him while we were still pretty young, he had changed. He seemed much older than our real age. He used to have a great sense of humor, despite his life being a little difficult. Our lives were both hard, in many ways that didn’t involve race. We both grew up in relative poverty.
But after only a few years of not seeing each other, he seemed cynical, which was very different from how I remembered him.
I don’t recall how I found him, but I met with him at his school. I expected to find the same guy who made me laugh. But he didn’t seem glad to see me. I must have mentioned it, and I probably pointed out that he had changed.
And that’s when Dan said, without looking at me, “Everyone changed but Jim.” The meeting was brief. I left and never saw him again.
Friends were tough to find for me. I didn’t have any black friends. My father was black and my mother was white. They separated when my younger brother and I were little, and we lived with mom. Despite what some people may or are rumored to think, racism has always been a part of living in America.
Black people tended to live in different zip codes, not the one in which I grew up. I was often the only black kid in school, and this story was and is still common. I didn’t have black friends because I didn’t live in the zip codes where black people lived.
Dan wasn’t the only friend I had. There was only one other; he was white too. Like me and Dan, Tim and I didn’t stay friends.
A lot happened after that, which is always a part of coming of age. And I guess that’s because a lot of things changed—including me.
Generosity, kindness, and love, especially the love from my wife, saved me from lifelong bitterness, for which I’m grateful. I think a sense of humor was also important. And even though definitions differ about what friendship is—I have friends.
Sena and I got to talking about a Twilight Zone show we saw over the holidays. It was a 1964 episode, not the regular program but short film that won a Cannes Film Festival award in the early 1960s, “An Occurrence at Owl Creek Bridge.”
The quick summary is that a Southern plantation owner is being hanged by Union soldiers for trying to set fire to the bridge to prevent the Union Army from attacking Confederate troops. The plantation owner seems to miraculously escape the noose, evades bullets and cannon fire, running all the way back to his plantation in an escape which lasts hours, finally almost rushing into his wife’s arms—but he can’t because at that moment his neck is snapped by the hangman’s rope. All of the action during his escape is a hallucination which happens in the blink of an eye.
It’s based on a short story of the same title by Ambrose Bierce. I vaguely recalled reading it years ago, possibly in a science fiction/fantasy anthology. At that time, I didn’t know the author’s background, which was that he’d been a Union soldier in the Civil War. He fought in a lot of battles and witnessed horrific injuries and death. He disappeared without a trace, and there is no explanation why or how.
As Sena and I talked about it, she wondered more about the details of the Civil War as context, while I thought the main point was about the time compression of a miraculous escape from execution that spoke of the nature and meaning of life and death.
When I searched the web to find out more about the story and the life of Ambrose Bierce, I saw her point.
I read the original story on the Internet Archive. It’s very short. Now, I’m not sure I ever really read it. I’m just a blogger and unworthy to really talk about it other than to acknowledge that it’s a work of genius. How the author’s spare and yet meticulous attention to every terrifying detail of war can be so ugly and yet so mesmerizing is beyond my understanding.
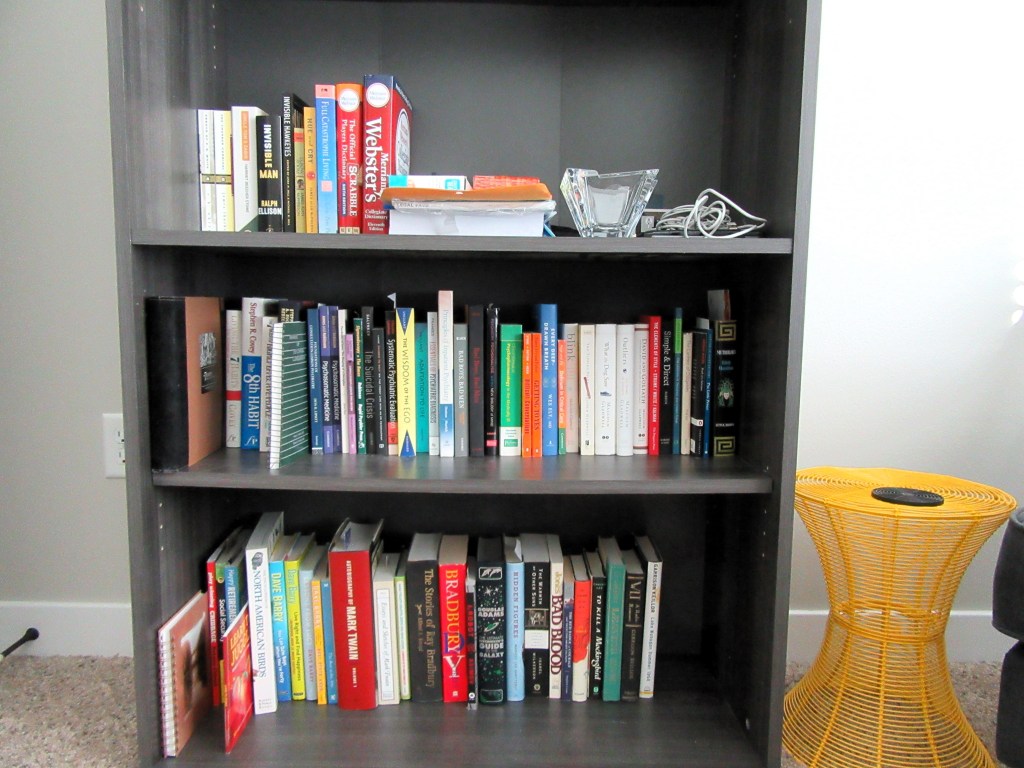
The other day, I finally rearranged my bookshelf. I’ve put it off for a long time. While I was doing it, I remembered where I spend the most time in my thoughts. I don’t have a very broad library, which probably illustrates where my mind wanders. It has changed very little over the years. Retirement affected it some, but not a great deal. After I rearranged the books, it was not just better organized. It made me think about the past, the present, and the future.
I have a lot of books by Malcolm Gladwell for some reason. The Tipping Point was published around the time when all of my immediate family members died for one reason for another. They died within a few years of each other. It was a difficult time. I remember hoping I would just get through it. I did.
I’m still a fan of Stephen Covey. The 7 Habits Manual for the Signature Program marks a time when I was contemplating leaving my position at The University for a position in private practice. It didn’t work out, and it’s just as well.
Of course, there are many books about consultation psychiatry, including the one I wrote with my former Dept. of Psychiatry Chair, Robert Robinson. Every once in a while, I search the web to find out what former colleagues and trainees are doing now. I can’t find a few, which makes me wonder. A couple have died. I’m a little less eager to look around each time I find out about those. Finding obituaries is a sad thing—and it makes me a little nervous about my own mortality. One or two have apparently simply dropped off the face of the earth.
I read some books for fun. I’m a fan of humorists, which is no surprise. The most recent is The Little Prince. That book and others like it inspire me.
I like books that make me laugh and give me hope. It’s difficult to sustain hope in humanity, if you read much of the news, which I tend to avoid.
I feel better when we go out for walks. Recently we did that about a week ago when there were a couple of warm days. On one day, we saw a couple of bald eagles and northern shovelers (the latter of which we’ve never seen before), at Terry Trueblood Recreation Area.
On another warm day we saw a couple Harvest Preserve staff members preparing to hang a big Christmas wreath on the side of a barn on the property that faces Scott Boulevard. They’d got some evergreen branches from an “overgrown Christmas tree farm.” It had a big red bow. They were going to decorate it further and hang it. We hoped it would be finished by the time we returned that day, but it wasn’t done.
When we returned a day later, it was very cold but the wreath was on the barn wall and it was festooned with gorgeous decorative balls. It was worth waiting for.
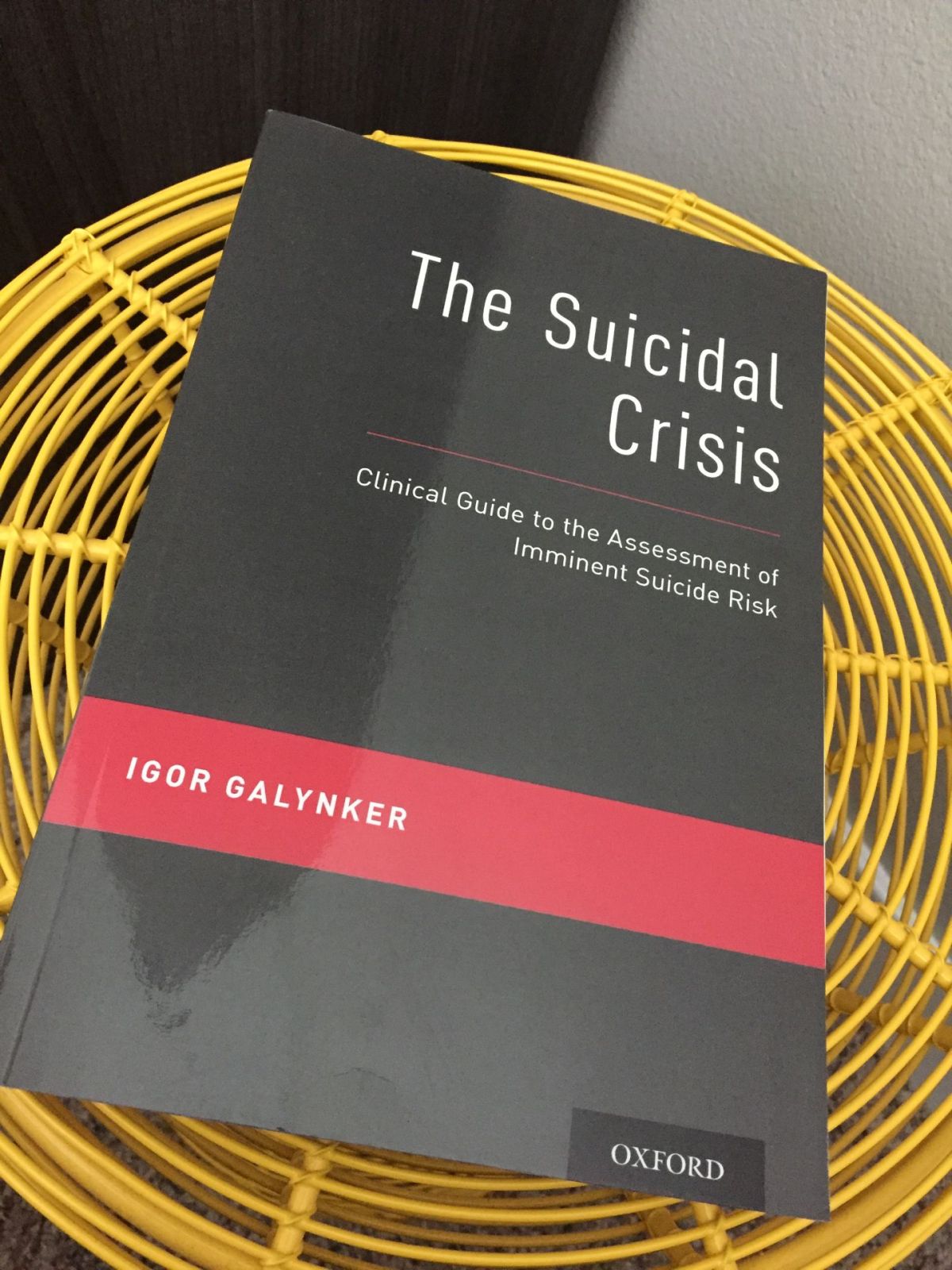
I was looking at my bookshelves and found the copy of the book, “The Suicidal Crisis: Clinical Guide to the Assessment of Imminent Suicide Risk.” It was written by Dr. Igor Galynker. It’s a fit topic for this month because September is National Suicide Prevention Month.
This brings back memories. I still have a gift from Dr. Galynker. It’s a stuffed animal called Bumpy the Bipolar Bear.
It arrived at my office at The University of Iowa Hospitals & Clinics in 2011. It was in a box addressed to:
WordPress
Attn: James Amos
200 Hawkins Drive
Iowa City, IA 52242
I’m still not entirely sure why he sent me Bumpy. There was no letter of explanation. I was writing a blog at the time called “The Practical Psychosomaticist” and I might have posted something about some research he published on suicide risk assessment.
I bought a copy of his book a few years ago. I barely had time to skim a few of the chapters because I was too busy conducting suicide risk assessments in the emergency room, the general hospital, and the clinics in my role as a psychiatric consultant. In fact, I think it’s an excellent resource.
I also found a YouTube video (posted about a month ago) in which he describes his suicide crisis syndrome assessment. You can find the actual set of questions for the assessment here and in a link posted in the description below the YouTube.
I was searching on the web for something about my co-editor, Robert G. Robinson, MD, for our book Psychosomatic Medicine: An Introduction to Consultation-Liaison Psychiatry, published in 2010.
The reason I was searching for something about him was that I’ve had difficulties finding anything on the web lately about doctors I had worked with years ago and admired—and the search revealed they had died. It has been a little jarring and got me thinking about my own mortality.
My search didn’t turn up any obituary about Dr. Robinson, but I found a couple of interesting items. One of them is, of all things, a WordPress blog item, the About section. It’s dated April 2012. I’ve seen it before. It’s supposedly about a person named Dr. Robert G. Robinson, MD and the only thing on it is his name and affiliation with The University of Iowa Carver College of Medicine. Every WordPress blog has an About section. I have one and I’ve been blogging since 2010.
There’s no entry in the About section for him on WordPress. However, there was another item on the web that looked like it was a blog (It’s another blogging site called About.me), and it was labeled as an About section. It was a biographical summary of his academic and scientific career. Of course, it was impressive. At first, it looked like he was planning to write a blog, which could have been very educational because he’s an extremely accomplished psychiatrist with a very long bibliography of published articles about psychiatric research, a lot of it about post-stroke syndromes.
But when I looked at the social media links on the WordPress page, it led to a picture of someone who is definitely not the Robinson I know. This person was a “Certified Rolfer.” Remember Rolfing? It’s a form of deep tissue massage developed in the 1970s. The Dr. Robinson I know was never involved in Rolfing.
I’m not sure what happened with the WordPress and other blog items, but it looked the WordPress section was a case of mistaken identity. The most recent genuine item on the web about him is a 2017 University of Iowa article about his receiving the Distinguished Mentor Award.
I hope somebody doesn’t get confused by that WordPress mistake.
Then, I happened to come across an article that, at first, I didn’t recognize. The link on the search page listed Dr. Robinson’s name. It’s on the Arnold P. Gold Foundation website for humanism in medicine. The title is “Are doctors rude? An Insider’s View.” It didn’t have my byline under it. It took me a minute, but I soon recognized that I wrote it in 2013. At the bottom of the page, I was identified as the author.
At first, I thought it was a mistake; there was a place for an icon that at one time had probably contained a photo of me, but it was missing. It’s my reflection about a Johns Hopkins study finding that medical interns were not doing basic things like introducing themselves to patients and sitting down with them.
This was not a case of mistaken identity. But I got a little worried about my memory for a few seconds.
Anyway, I was reminded of my tendency to have trainees find a chair for me so I could sit down with patients in their hospital rooms. I later got a camp stool as a gift from one of my colleagues on the Palliative Care consult service. It was handy, but one of my legs always got numb if I sat too long on it. It broke once and I landed flat on my fundament one time in front of a patient, family, and my trainees. The patient was mute and we had been asked to evaluate for a neuropsychiatric syndrome called catatonia. The evidence against it was the clear grin on the patient’s face after my comical pratfall—and because of the laughter that we could see but not hear.
One of the points of this anecdote is that it’s prudent to be skeptical about what you see on the internet. The other point is that parts of your identity can hang around on the web for a really long time, so it’s prudent to be skeptical about how permanent your current identity is.
A couple of days ago, Sena and I were playing cribbage and she thought she had a higher scoring hand than she actually did. She immediately realized it and scored it right. She commented that, at first, she thought she saw something she didn’t actually see. I quipped that “First you have to see it.” She thought that was pretty funny.
I actually said that because I remembered a quote from Wonko the Sane in Douglas Adam’s book “So Long and Thanks for All the Fish.” Wonko is a guy who lives “outside the asylum” because he saw the instructions on a box of toothpicks and thought it was so bizarre that he didn’t want to live in a society which needed that kind of instruction.
Now, you can find a lot of references on the web for the quote that arises from the toothpick instruction:
“It seemed to me, said Wonko the Sane, that any civilization that so far lost its head as to need to include a detailed set of instructions for use in a package of toothpicks, was no longer a civilization in which I could live and stay sane.” Douglas Adams, So Long, and Thanks for All the Fish.
You can even buy tee shirts printed with this quote. But that’s not the Wonko the Sane quote I was thinking of. In fact, I’m not the only one who thought of it and the first person I want to give credit to for calling attention to it is a WordPress blogger whose name seems not discoverable on his blog, but instead has the title Eppur Si Muove. It’s Latin and it means “…and yet it does move.” It’s attributed to Galileo who muttered it after being forced to recant his claim that the earth moves around the sun.
The quote is:
But the reason I call myself by my childhood name is to remind myself that a scientist must also be absolutely like a child. If he sees a thing, he must say that he sees it, whether it was what he thought he was going to see or not. See first, think later, then test. But always see first. Otherwise you will only see what you were expecting. Most scientists forget that…. So the other reason why I call myself Wonko the Sane is so that people will think that I am a fool. That allows me to say what I see when I see it. You can’t possibly be a scientist if you mind people thinking that you’re a fool. ~ Wonko the Sane, from So Long, and Thanks for All the Fish by Douglas Adams.
The blogger who wrote the post entitled it “Wonko the Sane—On Being a Scientist…”
Seeing what’s really there is very difficult to do. I’m fettered by expectations, desires, prior misinformation, and so on. Often, I see what I want to see rather than what’s there.
The toothpick quote gets more interpretations often by writers who sound like they trying to prove something. What’s even more interesting than them (and funnier) are the great number of actual instructions on how to use toothpicks, even how to do tricks with them.
What seems impossible to find are actual instructions for how to see.