
-

Svengoolie Movie: Island of Terror!
The Saturday night Svengoolie movie was Island of Terror. This one was released in 1966 and starred Peter Cushing as one of the scientists who battle monsters who are snacking on the skeletons of humans. The monsters are also silicon-based. These two elements reminded me of a couple of other things. One was the short…
-

KCCK Big Mo News and More
Well, ever since last fall, the Iowa jazz and blues radio station KCCK has been available only on channel 88.3 FM on our radio dial. Channel 106.9 has been out for months. We just found out that 106.9 is now working again and has been for over 3 weeks. It has been a translator channel…
-
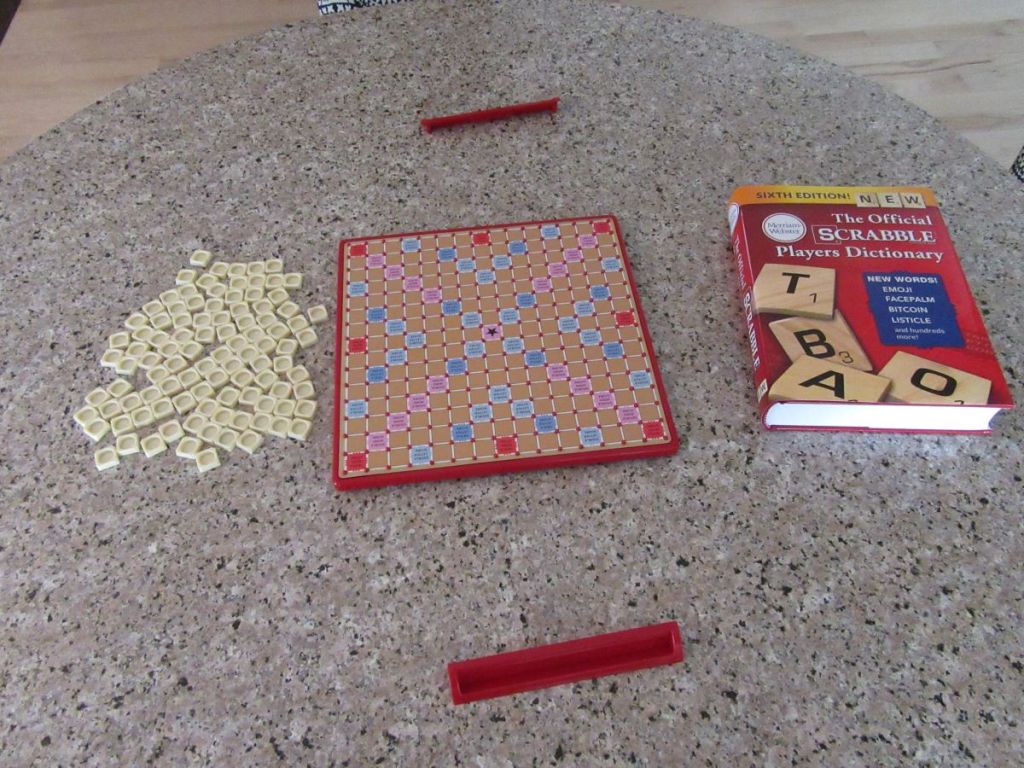
This is National Scrabble Day
I almost forgot that April 13 is National Scrabble Day. I don’t think I’ve ever blogged about it before, so I’ll inflict some thoughts on you now about it and add some others about International Cribbage Day, which is on February 10 annually—and which I evidently tend to forget every year. The big news about…
-
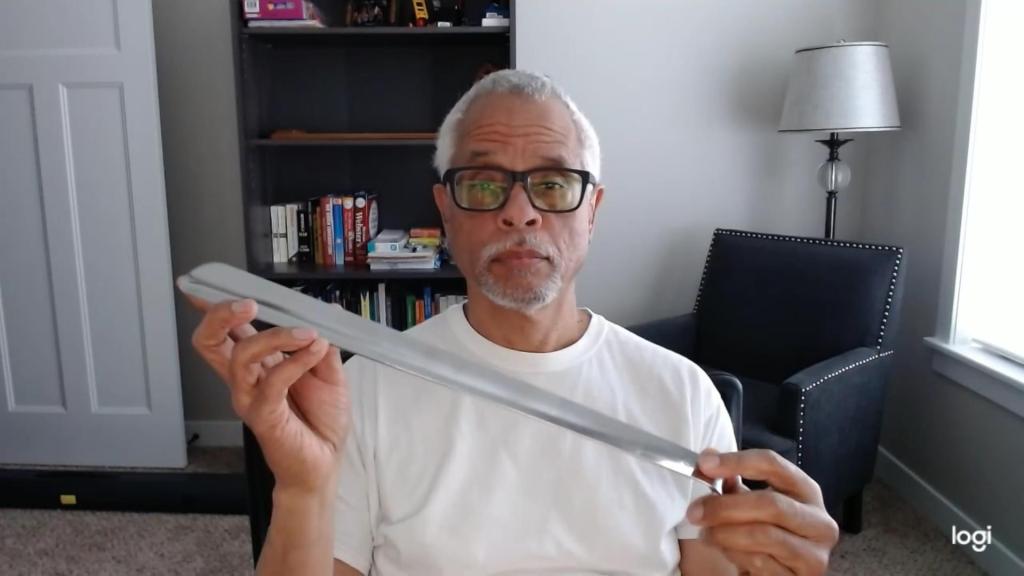
Shoehorn Thoughts
Sena got us three new shoehorns. They’re different sizes: the usual 6-inch, an 11-inch, and a 16-inch. Of course, you could ask why anyone would need a 16-inch shoehorn. The simple answer is that it’s to help you get your boots on. But would you be able to get it on an airplane in your…
-

The Wendy’s Orange Dreamsicle Frosty Is In Your Dreams
Well, we stopped by the Wendy’s drive up a couple of days ago and tried to order that new Orange Dreamsicle (sometimes called the Creamsicle) Frosty. But they were out of it, mainly because they didn’t order enough of it. I guess it’s a hot-cold item (Har!). They encouraged us to return the next day,…
-

Is it About the Nail or Not?
I saw this essay about getting your hamster off the treadmill and being in the moment. It’s not just for University of Iowa employees. I do the mindfulness thing, I juggle, I make dumb YouTube videos. And for a little over a month now, I have not scrolled past the first few headlines at the…
-

Our Solar Eclipse Day: A Happening on Terry Trueblood Trail
Yesterday, we went out to Terry Trueblood Recreation Area to see the solar eclipse. It was a gorgeous day for it, although a bit chilly. When we got there about 11:30 AM, the parking lot was pretty empty and only a few people were there. We even ran into a few on the trail who…
-
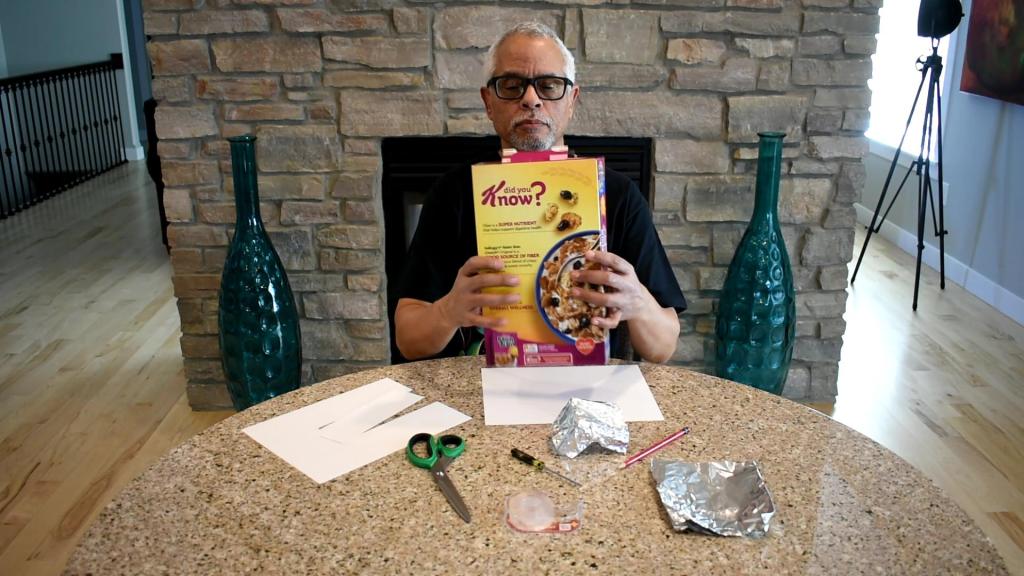
Off to See the Eclipse!
We’ll be off to try to see the eclipse today, because the weather report yesterday (and this morning!) said it would be sunny and warm. For the occasion, I made a cereal box eclipse viewer just for fun. We’ll see if it works. I sacrificed a box of Raisin Bran for it. Sena wondered where…


