I’ve been reading the short story collection Hue and Cry by James Alan McPherson with the idea that the entire book was new to me. So, I was stunned when I remembered the story, “A Solo Song: For Doc.” It has more than one layer of meaning, but on one level it’s about a Black railroad train waiter named Doc Craft who is forced into retirement. The narrator tries to teach a young waiter he calls youngblood learning the ropes about how the old school waiters made their work not just a job but a way of life. I was surprised to learn there was a television adaptation of the story made in 1982.
I must have read it in an anthology when I was a youngblood myself. It’s about racism but it’s also about aging, retirement, and change itself. It makes sense that I would feel differently about the story now that I’m older and retired.
I’m about a year into my retirement now and it has not been easy to adjust. Boredom and the search for a new meaning and purpose in my life still challenge me. While racism did not play a part in my decision to leave my profession, there is no doubt that things changed over my three-year phased retirement starting in 2017, dramatically so since the COVID-19 pandemic in 2020.
I thought I was still maintaining my skills as a psychiatric consultant in the general hospital. I was physically fit, in many cases better able to run up and down the stairs for 8 flights than the youngbloods. When they asked me why I became a consulting psychiatrist, I often told them that I “did it for the juice.” I guess that’s why Doc Craft did it.
Maybe I retired because I didn’t want to be pushed out. Doc Craft didn’t retire because he just wasn’t made for it. Sometimes this doc wonders….
I’m having a little trouble keeping all of the different moon names straight. Last night was the Snow Moon. I managed to get a snapshot of it. It doesn’t look different from any other full moon. It’s called the Snow Moon mainly because February tends have the winter’s heaviest snow fall, according to the Old Farmer’s Almanac. It’s also known as the Hunger Moon or the Bony Moon, because this time of year could mean starvation for some back in the days when you had to hunt for your meals.
I got that mixed up somehow with the Wolf Moon—which was in January. I missed that one. On the other hand, you can think of being hungry as a wolf, or the wolf being at your door, meaning not having the means to fend off starvation. Anyhow, that’s my excuse for getting the Wolf Moon mixed up with the Snow Moon. However, according to the Old Farmer’s Almanac, some Native Americans actually called the January full moon the Snow Moon.
We did get a lot of snow in both January and February. We shoveled a lot of it. I guess there’s no official name for the problem I have flexing my stiff, sore left ring finger, which I’m pretty sure results from my grip on the snow shovel handle. I also occasionally get a stiff, sore left big toe, which I can’t flex. I believe this is from the way I tend to lean into my left instep when plunging the shovel into a big snowdrift.
Before you get after me with critiques about my body mechanics when snow shoveling, let me say this: I quit twisting my back and throwing the snow over my shoulder this season.
That said about the basic meaning of the Snow Moon according to the Old Farmer’s Almanac, there are other interpretations. This can be a time for reflection on transitions in one’s life.
There have been a lot of big and little changes in my life, the biggest one recently being retirement. It has been difficult to release my grip on my identity as a psychiatrist. I’ve been a doctor for a long time. It’s hard to remember what I was before I started medical school in the summer of 1988, which was a pivotal time for me. I joined several other students who were members of minority and disadvantaged groups, including but not limited to African Americans, in the summer enrichment medical school program. It has since developed into what is now the Summer Health Professions Education Program (SHPEP) at the University of Iowa.
In fact, it was a pivotal time for the University of Iowa College of Medicine. Leaders, including Philip G. Hubbard, were trying to navigate the controversy surrounding the concept of affirmative action. Not everyone accepted the idea with open arms at the time.
These days, I sometimes find myself remembering how I’ve changed over the past several decades. I recall the sometimes-awkward feeling of being a freshman at Huston-Tillotson College (now Huston-Tillotson University) in the mid-1970s. I had grown up in in a small town in Iowa, where I was often the only Black student in class.
When I was a child, I was lucky enough to have role models from both sides of the apparent racial divide. Although Paul ‘Blackie’ Espinosa was not African American, he took me and my younger brother to a Twins baseball game. While I don’t remember much about that day except that it was fiendishly hot—I remember how kind Blackie was to us.
I remember Al Martin, who was an African American artist in the community where I grew up. He took me to an art show where he displayed some of his paintings. Here again, while the Iowa weather was a small distraction (it was a very cold fall day), I looked up to Al as a leader.
I also remember a local pastor, Glen Bandel, who was white and who came to our house one terrible night when my mother was very sick. He stayed all night watching to make sure she didn’t need to go to the hospital. He slept sitting up in a rocking chair. I googled his name the other day. Much to my surprise, he’s still alive and is in his 90s. There was a news item announcing the celebration of his 90th birthday a couple of years ago.
As I try to stitch my past to my present, I keep finding that the strongest thread over the last 43 years has been my wife, Sena. I don’t know where I would be without her. I don’t like to contemplate it. I don’t know how I’ll navigate the changes that are surely happening even as I sit here and, in turn, dread or welcome them. Change will happen, no matter what the shape or tint of the moon, and whether I want it or not.
I recently read an article about Maintenance of Psychiatry (MOC) written by Dr. Henry A. Nasrallah, MD and published this month in Current Psychiatry. The title is “Revamp the maintenance of certification program.” It brought back memories of my crusade to do the same thing in past years.
I lost my connection to that crusade when I was in my last year of my phased retirement contract. In a way, though I don’t miss MOC itself, I miss the sense of meaning and purpose I had while I opposed MOC through working with the Iowa Medical Society, through a petition to oppose Maintenance of Licensure (MOL, a state based version of MOC), and through writing articles and blogging about why I think psychiatrists and physicians in general don’t need these expensive, time-consuming activities which have led to anti-trust lawsuits being filed against certification boards.
In his article, Dr. Nasrallah criticizes the MOC as a monopoly perpetrated by the American Board of Psychiatry and Neurology (ABPN) and cites his own informal survey of 319 Current Psychiatry readers. He found that 86.5% of them recommended abolishing MOC. He tends to agree there should be an alternative to it. He recommends bringing back the oral exam.
I think it’s an interesting suggestion and I respect Dr. Nasrallah’s effort to not just oppose MOC, but to come up with another way for Psychiatry diplomates to keep their knowledge and skills up to date.
I remember my own oral board certification exam. It was very anxiety provoking, but I passed on the first try. There are reasons in addition to the anxiety they caused for why the oral boards were phased out after 2008. You can find them on the first page of a very entertaining post by Dr. Maria Yang. It’s a very long article, but the gist of the reasons for abolishing the oral boards is outlined on the first page. It was almost impossible to eliminate the wide variability of the live patient interview experience for diplomates while not being a guaranteed method for assessing a candidate’s knowledge and skills.
Dr. Yang lists several horror stories that make up the unverifiable yet terrifying lore about the process.
Even Dr. Nasrallah admits that the usual way the oral exams were conducted back in the day was almost unbelievably complicated logistically and also extremely expensive. He suggests that conducting them by videoconferencing could cut down on the costs, which is plausible. The justification for reinstating oral board exams is that it provided examiners a method for assessing a candidate’s interview skills and ability to collect and synthesize history and observation into a thorough diagnostic assessment and comprehensive treatment plan.
In fact, the academic medical center where I taught held what are sometimes called mock oral board exams regularly, which produced a tolerable mimic of the oral board experience in a less anxiety-provoking environment.
Making the oral exam, even in virtual format, the alternative to MOC would probably still make candidates nervous. It could also by logistically challenging as well. Would they be vulnerable to some sort of hack, such as Zoom bombing?
I spent a lot of time opposing MOC while I was working. It was frustrating. On the other hand, I thought it was important for me to let trainees know that life after residency would include challenges in addition to patient care and teaching, and that lifelong learning activities they engaged in might cost them a lot of money and personal time that they might find burdensome. I thought of myself as an example of a responsible protester in basic agreement with the principle of lifelong learning and improvement, although objecting to the certification boards’ methods.
The anti-MOC movement was a crusade that gave me a sense of purpose. I’m retired now. I salute Dr. Nasrallah.
Last night Sena and I watched a YouTube video walking tour of Boston, Massachusetts. It brought back memories of a trip we made there about 16 years ago. The main reason for the journey was a November teaching conference (sponsored by the Academy of C-L Psychiatry, back then called the Academy of Psychosomatic Medicine) on consultation-liaison (C-L) psychiatry I enrolled in, presented by the Mass General Hospital C-L psychiatry division. Funny, I don’t recall much about the details of the conference itself. Maybe that was because I got distracted by a bird pooping on me early on the first day.
I was on a break between programs and sitting outside the Boston Marriott at Copley Place. Suddenly I saw something white and gooey plummet inside the left cuff of my pants. It turned out to be bird poop, which led to my frantically racing back into the building to clean up.
I don’t know what kind of bird dropped that load of poop on me. It was probably a sparrow—but it could have been a seagull or even a duck, which reminds me of the highlight I can manage to remember about the trip, which was the Boston Duck Tour. I guess that means that the old story about a bird pooping on you bringing good luck might be true.
Anyway, while we didn’t have a chance to walk the Freedom Trail, we got tickets for the Duck Tour on a very chilly day. Remember, it was November. Because the annual meetings of the Academy of C-L Psychiatry were held in November, they were usually in warmer parts of the country. The Boston location was a real outlier.
We were lucky (because of the bird poop, no doubt) to find the Boston Duck Tours station at the Prudential Center on Boylston Street, practically right across the street from our hotel.
We were pretty impressed by the versatility of the Duck Tour bus, which converts readily into a boat because it’s a replica World War II amphibious DUKW vehicle.
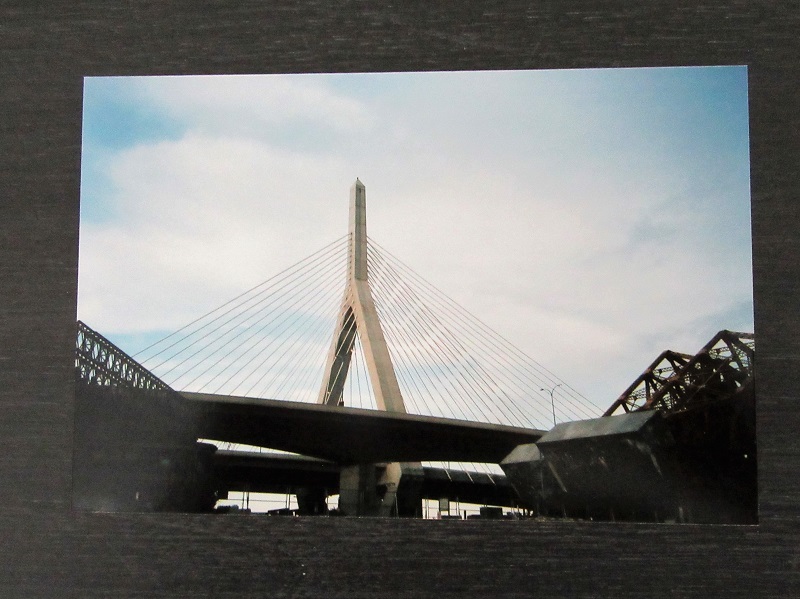
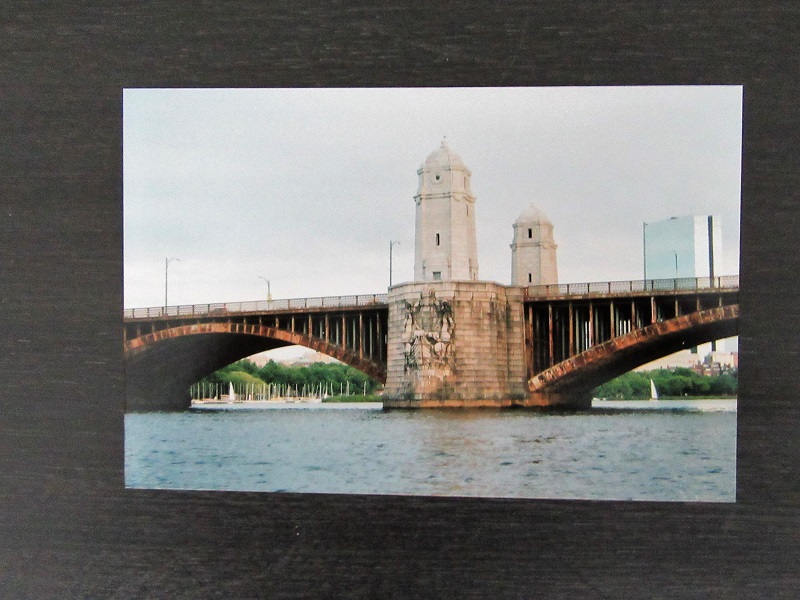
It was a fantastic sightseeing tour. I remember the Leonard P. Zakim Bunker Hill Bridge and only now do I compare it to the Longfellow Bridge (also known as the Salt & Pepper Bridge). The Zakim cost a $100 million or so new, but the repair of the much older Longfellow Bridge cost over $300 million. I’m not knocking old stuff; just sayin’.
Leonard Zakim was a famous civil rights leader whose courage and respect for the dignity and rights of others seemed to get stronger after his bout with bone marrow cancer, the pain and depression from which he dealt with by using both medical and complementary therapies.
Leonard P. Zakim Bunker Hill Bridge left and Longfellow Bridge right
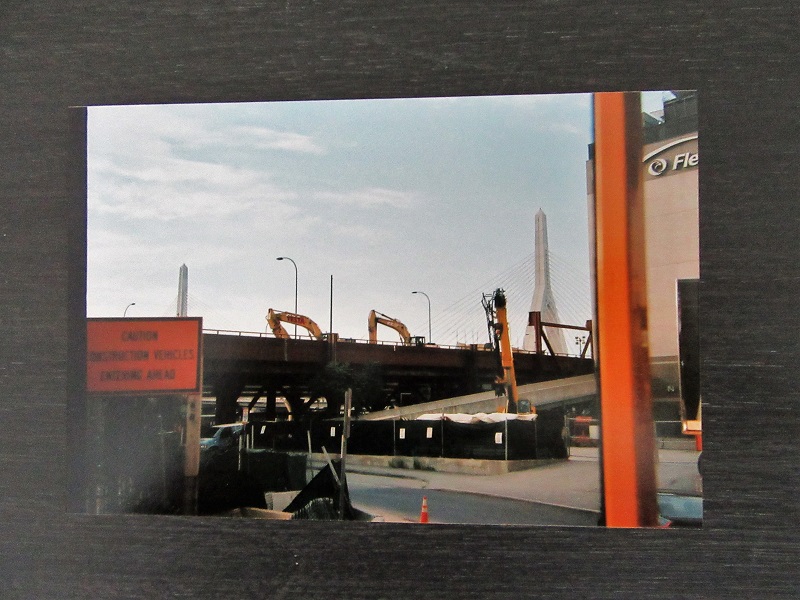
The Zakim Bridge was a part of the “Big Dig” which was a major $22 billion reroute of the main highway running through Boston and which was basically done by the time of our visit in 2004. It cost a lot of money and there has been some controversy about it.
Big Dig
There was also some controversy about whether the Duck Tours driver let Sena drive the vehicle while we were either crossing the Charles River or the Boston Harbor, I can’t recall which. He asked for volunteers to pilot the craft, but there were no immediate takers. He asked again and Sena spoke right up and took the driver’s seat. She’s modest about whether she actually drove the Duck.
Massachusetts State House left and Boston Harbor (I think) right
Then again, maybe that bird poop luck kept us on course.
It has been a while since my last post. I’m hanging in there although sometimes it’s difficult to stay optimistic. I’m reminded of the Survivor Tree, the Callery Pear in New York City. You can easily google the story about this tree which somehow survived at Ground Zero after the 9/11 attack on America in 2001. We visited New York in the summer of 2017 and saw the Survivor Tree at the 9/11 Memorial & Museum plaza. It’s hard to believe that was 19 years ago. And now we’re dealing with the Covid-19 pandemic.
I’m still adjusting to my new identity as a retired person. I was reminded of that when I read the recent post “What is your Identity?” on 9/12/2020 by The Good Enough Psychiatrist. She’s resilient and optimistic, traits I admire. I tend to be rigid and pessimistic, especially when I have a lot of time on my hands.
I also need to get out of my head. It’s amazing how easily reminiscence can morph into rumination. Galloping all over the hospital as a psychiatric consultant distracted me from that habit. On the other hand, Sena and I reminisced the other night for quite a while. I was astonished at how much we both recalled about our 42-year long marriage and the adventures and challenges we’ve been through.
Our first house was a challenge. Shortly after we moved in, I had to try to mow the tall grass which had been neglected for a long time. I had to use either a scythe or a weed whacker. I honestly can’t recall exactly what I used but the scythe sounds more impressive, so I suspect it has crept into the story more for dramatic effect. It was a very hot day and my first encounter with my neighbor from across the street was his generous act of lending me his power lawnmower. He was a white man and, back in those days, kindness in that context was uncommon.
The only time I used a power mower other than at that house was when I went to Huston-Tillotson College in Austin, Texas. It’s now called H-T University. It was one of the historically black colleges in the country and I recall feeling a bit awkward there since I had grown up in largely white neighborhoods in the Midwest. Anyway, I helped mow the campus grounds. I guess “helped” might not be the right word, especially if you consider the perspective of the groundskeeper who was in charge of fixing the power lawnmowers I destroyed. I wrecked a few mainly because I kept running over rough, rocky ground. After I dragged the 2nd or 3rd ruined mower back to him, he stared at me and shook with rage. Mercifully, memory fails me at this point.
I’m realizing I could probably go on rambling like this for a good while. I guess that might mean I’m gradually adopting the identity of a garrulous old retired guy. I know that sounds pessimistic.
On a more positive note, Sena and I had a great time in New York City three years ago. We’re glad to have the memories. Sena is optimistic and resilient by nature. She’ll help me imagine brighter times coming in the future.
It has been only about 3 weeks since I retired and—I am not living the dream yet. I’ve always been a worrywart and I find that I’m worrying about a lot of things: money, things to do, the future. If you just heard me say that I’m loving retirement, then you’d probably guess I’m not telling you the truth.
That was the point of starting the blog in the first place, to tell the truth about what the journey to retirement and finally getting there is really like for me.
My guess is that I’m in the early stages and the angst will probably pass. On the other hand, I have more than once considered going back to work. I could talk myself into it pretty easily. On the other hand, the pandemic and other upheavals have changed the environment where I used to work as a general hospital psychiatric consultant.
It’s not the same world. And I’m evolving too. Right now, I feel lost. It occurs to me this is a lot like homesickness.
Ironically, that’s pretty much how I felt when my wife and I first moved to Iowa City over 30 years ago so I could start medical school. Even then, I felt out of place. I’d been the proverbial older student all through undergraduate years and never felt like I quite fit in.
I nearly quit medical school in the second year. It was a struggle to stick it out. I wanted to return to what I had been so comfortable doing in the past. I worked for a consulting engineer firm as a survey crew tech and drafter. I got really comfortable in the culture, which is why I started off majoring in engineering. I let go of that pretty quickly. I got homesick. But I didn’t go back.
I came down with homesickness a couple more times after I started working as a psychiatric consultant in an academic center. Twice I left for private practice because I thought I would like working in “the real world” of medicine. I paid dearly for that. At those times, I went back home.
This anxiety, tension, and longing for the familiar now that I’m retired is a lot like homesickness. I guess part of the cure is time.
Well, it has been almost two weeks since my last day of work. That was called my “termination date,” which strikes me as an ominous term. We now have a new mailbox because we moved in June. The mailbox is a sign of moving away from the old way of life and moving toward a new life as well as a new home. A new beginning follows the termination.
There’s a lot of stuff coming to the new mailbox on the curb outside. We’re getting a mix of new things in the outer mailbox—the same is happening in my inner mailbox. Sorting the mail in both is definitely a challenge right now.
I’m still working out how things will be in the new home, and in the new life stage. I’m wrestling with a lot of new goals, both practical in the outer world and psychological in the inner world.
There is good news in the mailbox, and some not so good. Retiring meant moving away from a daily work schedule which kept me occupied and focused on being a specific kind of person for a long time. I was a psychiatric consultant in an academic medical center. I played a specific role, had specific tasks and challenges which brought specific rewards and frustrations.
That mailbox was always crammed full of stuff and, while a lot of it was good news, some of it was junk mail. I was often rewarded for my work as a consultant and as a teacher. On the other hand, my focus was frequently on work, which left an imbalance elsewhere in my life. Work itself was often full of obstacles.
Now, the new mailbox is full of surprises. Many of them remind me I have a new skillset I need to develop as a retiree. The junk mail consists of things like anxiety about the change in my identity (fireman to retiree), boredom, and frustration over the need to learn how to fix a loose faucet handle instead of catatonia.
There will always be psychological junk mail. The thing about that kind of junk mail is that I can’t just toss it in the garbage. In the last month, I’ve lapsed in my mindfulness practice because of all the tasks of moving and making the transition not just to another home—but to a new identity.
I’ll be working on getting back to mindfulness, although I remember the message sent by the UIHC director of the Mindfulness Based Stress Reduction (MBSR). It was prefaced by a quote:
“I am thankful that thus far today I have not had any unkind thoughts or said any harsh words or done anything I regret. However, I need to get out of bed and so things may become more difficult.”
Sylvia Boorstein, Mindfulness teacher and author.
My mindfulness mat is rolled up in a room downstairs. My mind is also rolled up—tight around thoughts that are impossible to avoid or deny. Another quote from Sylvia about self-talk:
“Sweetheart, you are in pain. Relax, take a breath. Let’s pay attention to what is happening; then we’ll figure out what to do.”
I’m writing this post today because this firefighter retires tomorrow—and I’ll probably be very busy and too weary at the end of my last day on the psychiatry consult service to write. In fact, I’ve been too busy and tired to post for the last several weeks because we’ve been in the process of moving. Does that ever really end?
I can tell that what will really end at around 5:00 PM tomorrow is my career as a general hospital psychiatric consultant. It has been a long time coming. I’ve been on a 3-year phased retirement contract and going back and forth between wishing for it to end sooner and being scared to death as the final day approaches.
There are those last things: handing in the keys, the white coats, the parking hang tag and the like. I’ve cleaned out my office and somebody already wants it. I’m surprised that I’m just the tiniest bit territorial about the place, which is strange. I never spent much time in it because I was always chasing consults around the hospital.
I’ve never retired before. I wonder what the rules are. I still don’t know how to answer everybody’s question: “What are you going to do?”
There is the “new” house. It’s actually an older home, which fits my status as an older person, I guess.
The floors squeak and creak, a lot like my joints. There are little jobs and slightly bigger jobs to do for which I’m painfully aware of the need to develop a whole new skill set—or at least relearn them.
It’s about new noises and new animals. A fox trots across our yard occasionally. I’m used to deer, but we’ve never spotted a fox on our lawn. It has a rusty coat streaked with a lot of gray. It looks old. But it’s a good hunter and more than once we’ve seen it carrying a big mouthful of something that might have put up a pretty good fight.
I’m touched by the well-wishers, and those who say thanks for the memories. Just about every day of the last week, I’ve seen and done something at the hospital which makes me say, “That is what I’ll miss.”
The robins are building their Hurrah’s nests in our back yard again. That’s about the only thing that has not changed. The COVID-19 (C-19) pandemic has changed just about everything else in our lives.
I wear a face shield now at the hospital. We’re told to wear it as much as possible, like putting on our clothes in the morning. Don’t we leave them on all day? The shield keeps you from touching your face, which is why it’s better than a face mask. However, I’ve noticed something about wearing the face shield for much of the day. Before I describe it, let me give you analogy: If you’ve ever worked detasseling corn when you were young a long time ago, you might remember what happened when you closed your eyes at night and tried to go to sleep. I saw corn fields—miles and miles of corn fields. When I opened my eyes, the vision would disappear. But as soon as I closed my eyes again, I saw the vast corn fields.
It’s crazy, but I have a similar sensory after-effect when I doff my face shield–sometimes I still feel the headband. The pressure of it is just the same as if I were still wearing it. I suppose it’s because I cinch it too tightly. But if I don’t, it slips down my brow, pushing my eyeglasses down my nose.
Another change—I’m a Consultation-Liaison (C-L) Psychiatrist, so I’m used to washing my hands in between patients in the hospital. Now, I’ve got something I’ve never had before–alligator hide patterns on the backs of my hands. They’re dry and cracked. I don’t count the number of times I wash my hands, but it’s a lot more frequent than I used to do. It’s not uncommon for health care professionals to wash hands 75-100 times a day in the C-19 era. I have to use hand cream conscientiously—something I almost never did.
I’m less comfortable being closer than several feet away from people. I tend to hug the walls and corners in stairwells, where I now encounter more people than I ever have before. I guess the message everyone hears is “Stand by me—six feet away if you please.”
I don’t shake hands anymore. The lines into the hospital sometimes lead to crowding while we wait to have our temperatures taken and answer the screening questions about whether we’ve had fever, cough, shortness of breath, etc. It’s perfunctory most of the time, because virtually always the answer is “no” and everybody is in a hurry.
I don’t carry my little camp stool with me anymore, which allowed me to sit down with patients and have face to face, eye level interaction. I’m distinctly uncomfortable standing over them because I haven’t done that in years. If there is a chair in the room, I’m hesitant to use it because, like the camp stool, I worry that it might carry C-19 virus on its surface.
I used to evaluate psychiatric patients in our emergency room by simply going there and seeing them face to face, either in their rooms or, when it was really busy (which is most of the time), in the hallways.
I just used a remote telehealth interface platform using an iPad the other day, which allows me to interview patients from my office, in order to avoid the risk of contagion. It was a little slow and awkward, and I was uncomfortable that a health care professional had to be in the emergency room to hold it up for the patient—who was covered in blood. I felt a little guilty.
I used to round with medical students and residents on our patients. We were the movable feast, a sort of MASH (Mobile Army Surgical Hospital) unit, more like Mobile Unifying Shrink Hospital (MUSH). Unifying means unifying medicine and psychiatry. The medical students are not permitted on the wards now, in order to protect them. It’s awkward rounding with only one resident at a time, although another resident can do other things like chart review and telephone relatives for collateral history. I get in the hospital earlier nowadays, and see many non-C-19 patients alone without trainees, preparing for the C-19 surge when I expect we’ll get many more consultation requests to help care for C-19 patients with delirium and depression. It’s a one-man hit-and-run psychiatry consult service and efficiency is mandatory to meet the demand.
I see patients by myself for another reason. Try as we might, C-19 positive patients will slip through the screens. Many are asymptomatic but contagious, and any test will have false negative results. The idea is to expose the least number of health care front line staff members as possible. Faculty capacity is stretched pretty thin, which is pretty much the situation everywhere. I have to choose. I’m older. I’m weeks from retirement. I’m afraid.
But robins don’t have the burden of choice. They obey their instinct every spring, just the same.
It’s snowing today, starting this afternoon. It’s not a blizzard. It comes down slowly and peacefully. Occasionally I see people and their kids and dogs out walking in it, likely grateful for the fresh air. It’s hard to be stuck indoors, self-isolating because of the COVID-19 epidemic. We play cribbage.
Sena tried the grocery pickup thing in order to avoid crowds. She ordered yesterday and picked up this afternoon. For the most part, the shoppers did OK. We noticed that as she was ordering, items would be sold out even before and sometimes after (we found out later) the ordering was done.
But we were able to get toilet paper.
This epidemic changes your life in many ways. I’m in the latter stage of phased retirement and I’ll go back on the consultation-liaison psychiatry service in April. I expect it to be busy, but I’ll likely not do as many face-to-face interviews, depending on the situations in the emergency room and the general hospital.
I probably won’t carry around my camp stool, which I use to sit with patients when I interview them. It’s just another item that the coronavirus can stick to.
We’re told not to wear neckties because they’re germy, but I gave that up a long time ago for banded collar shirts. But now I’ll have to remember to keep my arms bare up to the elbows.
We’re also reminded to avoid elevators so as to maintain social distance (6 feet or 2 meters, roughly). I’ve been taking the stairs for years. Many people avoid the stairs.
I’ve gotten used to handwashing because I’m a hospitalist. I’ll wear masks a lot more frequently as well as don and doff personal protective equipment as needed more often.
I’m older and I worry a little bit about belonging to a higher risk age group for COVID-19 and being exposed more. On the other hand, I’m pretty healthy compared to a lot of patients younger than me.
I’m glad the next generation of doctors will be taking over, though.