Again today, I hoofed it around the hospital. I put 43
floors and a little over 4 miles on my step counter.
I don’t like waiting for elevators so I take the stairs. And
a Consult-Liaison Psychiatrist is like a fireman, running all over putting out
fires.
I did other things today. I gave the usual lecture on
delirium and dementia to the medical students. I notice that as I have gotten
older, I tend to tell more anecdotes about my experiences managing delirium in
patients on the medical side of the hospital.
I’m in my anecdotage, as I told the students today.
I also lamented the decision by the powers that be to
copyright the Montreal Cognitive Assessment (MoCA). The medical students will
be able to use it for free, but faculty won’t.
I think that’s ageism. I won’t pay so I won’t use the MoCA anymore.
Well, I’m pretty tapped out, so it’ll be a short post today.
I’m back in the saddle, running around the hospital on the psychiatry consult
service. This is my last year of phased retirement and in 11 months—I’ll be fully
retired.
I put 36 floors and 3 miles on the step counter. I’m feeling
every one of those. Sena bought me some banded collar shirts and I’m wearing
those instead of a shirt with a necktie. I don’t need a tie bar.
And I don’t worry about a delirious, violent patient
strangling me with my necktie.
We had a small scare tonight. We were looking at my total compensation statement (the last one) and got the Sharp Elsi Mate EL-505 vintage calculator out to crunch some figures. The calculator went dead.
Still going…
I put some new batteries in it, hopeful. It still didn’t work. We’ve had this calculator for over 30 years and it ran more than a decade on the first set of AA batteries.
I tried another pair of batteries. It worked! The vintage calculator lasted longer than the batteries. It’s nice to know that just because something’s old doesn’t mean it’s useless.
Most of this post is an updated redux from years ago about an
informal bedside test for delirium called the oral trails test. I learned about
it from my senior resident when I was a junior psychiatry resident in training
at the VA Medical Center.
There was an elderly patient admitted to the psychiatry unit
who was thought to be psychiatrically ill but who actually seemed confused to
me and the senior resident. We consulted medicine in order to get him transferred
to the general medicine unit but it was tough going. I think the medicine
resident disagreed with our clinical impression that he was confused and didn’t
think medical transfer was necessary.
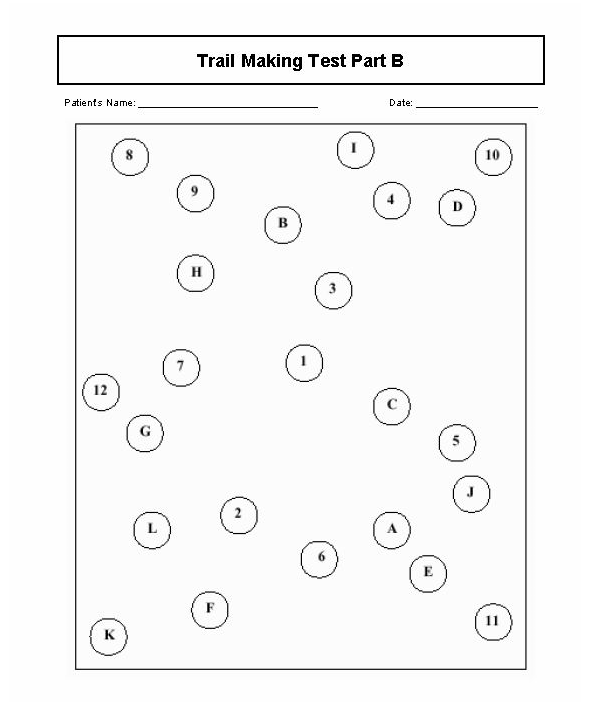
Anyway, my senior resident showed me her version of the oral version of the mixed Trails A and B Test for executive function. There is a written form which is part of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). First, she asked him to count from 1 to 7; then she asked him to recite the letters of the alphabet from A to J. She then asked him to try reciting those letters in alternating sequence. Of course, he failed miserably and was eventually transferred to internal medicine. The Trails actually is a paper and pencil test and it looks like a dot to dot game, like the example below:
Trails Test
My senior resident told me she learned the oral Trails test
from her senior resident and couldn’t remember anything else about it. I used
the test for years but a neuropsychologist criticized the practice, questioning
the test’s validity, and rightly so.
Of course, I’d been doing it wrong. You’re supposed to have
the patient count to 25, then recite the letters of the alphabet, then recite
the numbers and letters in alternating sequence from 1 to 13 and A to M. More
than two errors in pairings indicate cognitive impairment.
There are limitations to the verbal Trails and caution is
advised in more recent literature, indicating that there are moderate education
effects in older patients and that it may be wiser to use both paper and pencil
and oral versions together.
Still the search goes on for quick and dirty ways to screen
for cognitive impairment in the elderly because this and advanced age are two
main risk factors for delirium.
Nowadays, I do the Mini-Cog (shown in the video below) or the Single Question in Delirium (SQiD) test, which just involves asking a family member if the patient seems confused lately.
References:
Mrazik, M., Millis, S., & Drane, D. L. (2010). The oral
trail making test: effects of age and concurrent validity. Archives
of clinical neuropsychology: the official journal of the National Academy of
Neuropsychologists, 25(3), 236–243.
doi:10.1093/arclin/acq006
Sands, M., Dantoc, B., Hartshorn, A., Ryan, C., & Lujic,
S. (2010). Single Question in Delirium (SQiD): testing its efficacy against psychiatrist
interview, the Confusion Assessment Method and the Memorial Delirium Assessment
Scale. Palliative Medicine, 24(6), 561–565. https://doi.org/10.1177/0269216310371556
This is a short Coach’s Corner video on somatoform and
related abnormal illness behaviors which prompt physicians to request
psychiatric consultation. Medically unexplained physical symptoms are not rare
in the hospital and in medical clinics.
The general idea is to remember Stephen Covey’s caution about effectiveness and efficiency, which is that you have a lot better chance being effective rather than efficient with people.
“With people, slow is fast and fast is slow.”
Stephen Covey
The point is that it’s very important to listen for understanding and to validate pain and suffering. That means sitting with patients and taking time to hear what they tell you.
There is an excellent presentation on conversion disorder (also known as functional neurological disorder) on the National Neuroscience Curriculum Initiative (NNCI) web site. It’s very helpful for clinicians and patients.
Well, it has been about 3 months since I opened this blog. My YouTube channel needed an updated channel trailer, so I’m posting it here as well. Why not?
I was surprised at how long a minute and a half channel trailer took to make, even with the aid of video editing software (maybe because of it, partly).
In my situation, a channel trailer is sort of a mini biography. It’s hard to compress a career into a short clip that takes about 5 minutes to upload to YouTube–after a few hours of what was essentially cut and paste.
As you can gather, my path is changing. Over the next 12 months, I’ll be half off and half on the consultation-liaison psychiatry service. That’s according to the terms of my phased retirement contract.
This is really a re-introduction, of course. I’m slowly evolving–not in any big way. I’m still a geezer.
On the other hand, I have found that I’m much more comfortable being on some kind of schedule. I still get up early, only by about an hour later. I generally arise between 5:30 and 6:00 a.m. That may seem very early to some.
I eat less when I’m off service (which I’ll call “retired” for simplicity). That’s probably why my trousers fit more loosely.
I need to have something to do. I exercise daily, for about 20 minutes. I do mindfulness meditation and yoga. I blog. I photograph and film, mainly birds, which I post to YouTube.
The only reason I ‘m not a disaster in the kitchen is because you generally can’t get me within 10 yards of it unless I need a snack I can immediately eat (like an apple). I still don’t cook–not really. It’s embarrassing.
I trim the lawn and by that, I mean just around the walkway edges and some of the garden margins. I don’t mow the lawn because my wife does a much better job, by mutual agreement.
I’m not a gardener. I’m a garden appreciation expert. That means I watch gardening that is done by others.
I’m anticipating a busy time next month on the psychiatry consultation service. I suspect delirium will be the main event, as it is most of the time.
So I made a very short YouTube video on delirium. It’s cast in the style of a coach’s corner because I was one of the many clinicians who won the Excellence in Clinical Coaching Award this year.
It’s getting close to the busiest time of the academic year in a teaching hospital–July. The residents have a steep learning curve during that month. Some hospitals have a sort of boot camp to get the upcoming first year internal medicine residents prepared for July.
I’m looking at my retirement countdown timer and it’s showing I have 12 months to go. I’ll be back in the saddle July 1st.
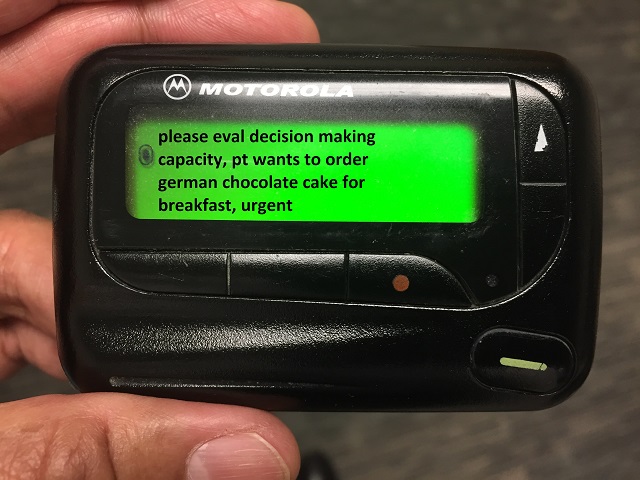
July is usually the time for the most interesting psychiatry consultation questions. Many years ago, the psychiatry residents used to keep a list of the weirdest ones. At least that’s what they claimed. Actually, I think most of them were simply made up–maybe all of them. Even though there is no way to know for sure, there is very low probability that any item on the list below could identify any patient.
We used to call it the “wailing wall” of strange and difficult to answer psychiatry consultation questions sometimes asked by our non-psychiatry colleagues from internal medicine and surgery. Questions have been and still are sometimes ambiguous (worse in July) and often need to be reframed so that the psychiatric consultant can be helpful to both customers—the patient and the consult requester. Here are some “quotes” from probably fictitious consultation requests tacked to wailing wall in the distant past, certainly embellished in some cases by frustrated psychiatry residents:
1. “EEG shows no brain activity.”
2. “The patient doesn’t like me.”
3. “We want to know
if the patient who believes they are Sponge Bob and wants to leave the MICU to
start filming a new movie—is competent.”
4. “I’m a
humanitarian but can you transfer this patient to Mexico?”
5. “The patient looked at me funny.”
6. “We are wondering
whether to discharge to their own apartment a patient who is oriented only to
self, cannot perform activities of daily living, and is actively
hallucinating?”
7. “I prefer not to speak with my patients.”
8. “I prefer not to speak with families.”
9. “Patient gets irritable during “that time of the month.”
10. “We are wondering
if the patient should be taken off sedation before getting a history from
them?”
11. “Patient swallowed their narcotic sobriety pin and is upset that morphine was discontinued.”
12. “The patient is eating their fingers off.”
13. “Cardiac arrest.”
14. “Consult for bilateral disorder or generalized panic disorder.”
15. “Anxiety and agitation 5 minutes before Code Blue.”
16. “Please evaluate for catatonia versus brain death on intubated patient.”
17. “Patient was fine
yesterday but now unresponsive. Please rule out catatonia before we work up. If
catatonia ruled out, we’ll then get a head CT and labs.”
18. “We want the consult for our own safety.”
19. “We need psychiatry’s blessing before we can feel comfortable discharging the patient.”
20. “Patient admitted for renal failure after being gored by a bull at a rodeo, please evaluate if this was a suicide attempt.”
Some are humorous and a few are mind-boggling. What they all speak to is the omnipresent opportunity for the C-L psychiatrist to excel as an educator. Reframing the question is a skill that requires patience, diplomacy, and credibility as an expert in this field.
What’s the question again?
What this may also indicate is the necessity to include a bit more about psychiatry in medical school clerkship programs.
I guess I’m incorrigible; there are now 4 eggs in the robins’ nest. Progress there reminded me of another kind of progress–in integrated health care.
On that note, this is just a brief update on the Medical-Psychiatry Unit (MPU). I thought it would be a good time to do this since a hard-working Pennsylvania psychiatrist notified me of the very successful Medical Complexity Unit (MCU) in operation at Reading Hospital. See my post from May 23, 2019.
I co-attended on our MPU for 17 years before I chose to concentrate on the Consultation-Liaison Psychiatry (CLP) service. The health insurance payer system challenges have probably not changed much. I still believe that the MPU is a great place to teach trainees to appreciate the rewards and challenges of caring for patients with complex, comorbid psychiatric and medical issues.
I hope the video makes the case for that. I decided it didn’t need a voice over. I welcome any comments and questions.
Occasionally, despite my being in phased retirement, I get a
reminder that my colleagues may need some advice about an issue for which I might
be a useful source of institutional memory.
One of them is the psychiatric consultation for assessment of candidates for organ transplant. I have a slide set and a YouTube video that are still useful as long as viewers remember that some of the slides and the text are dated.
For example, the video refers to my former blog The
Practical Psychosomaticist (which l later renamed the Practical C-L
Psychiatrist), and which I cancelled June 1, 2018. The references are also old,
but much of the information is still useful.
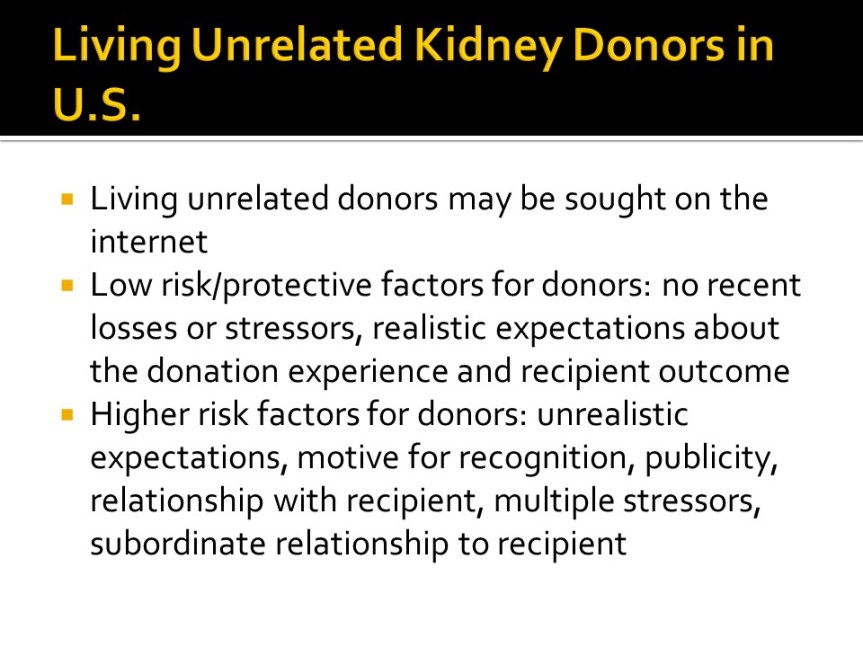
I’ve included both the video and the slides for the Dirty Dozen on Psychosocial Assessments for Organ Transplant. You can view the slides and just listen to the audio like a voice over in the video. That way you don’t have to giggle at the back of my head and my camera comically reflected in the office window behind me. Turn on the video, click in the slide set to open it, and listen to my prompts for which slide I’m on.
Use this as a voice over for slide set below
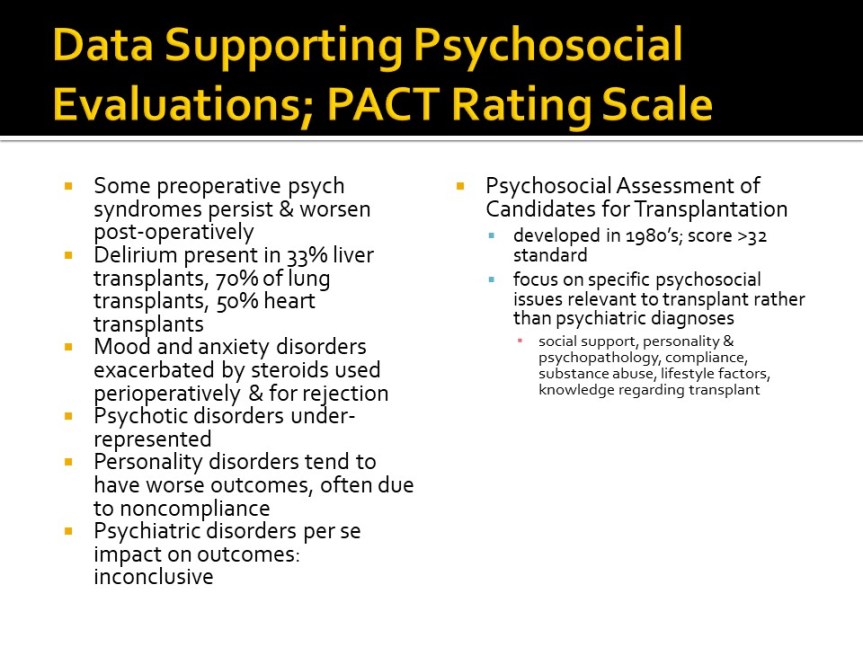
The most frequent question that
consultees from the transplant team ask is whether the candidate is a good risk
for receiving an organ that is in short supply, which therefore must be
allocated carefully, and of which the candidate must be prepared to be a good
steward. Psychosocial screening is a feature of most transplant programs.
Rather than seeing ones self as a gatekeeper, most experts agree that the most
useful part of the psychosocial screening process is to identify psychosocial
factors that would interfere with the candidate’s successful adaptation to life
posttransplant, and to develop a plan for managing them using available
resources.
The evaluation phase is critical to diagnosis of major psychiatric problems and to treatment planning for evidence-based interventions. However, providing follow-up through the other phases of transplant allow optimizing the development of a therapeutic alliance to foster adherence to both psychiatric and medical treatment and further evaluation of psychosocial challenges as well. The waiting phase is a very stressful time and often the candidate must tolerate deteriorating health while watching others transplanted sooner. In the post-transplant period, about 20% of patients develop any psychiatric disorder, most notably depression and PTSD.
There’s a triple advocacy role for evaluators conducting organ
transplant assessments: advocacy for the patient; for the persons on the
waiting list; and for society in general in terms of husbanding allocation of
scarce resource (“organ stewardship”).
That makes it critically important to examine the nature of the
therapeutic alliance.
Transactional/Adversarial or Transformational?
Transactional/Adversarial:
Atmosphere is typically highly charged emotionally, with
a sense of urgency.
Interrogation mode rather than exploration of motivations
and feelings. Focus is on past rather than future, exclusive approach with
emphasis on utilitarian paradigm and wait list advocacy. Methodically and
meticulously confrontive; blaming. Team asks “Who else could we help?” Little
or no interpersonal room to witness the patient make sense of impending death.
Withholding,
rejecting, paternal, authoritarian (rather than shared) experience.
Win/Lose or
Lose/Win.
Transformational:
Atmosphere
of created space for calmer review and listening for understanding.
More likely
to have focus on future rather than past, and an inclusive approach with
emphasis on medical necessity paradigm and patient advocacy. Affirming and
supportive of change. The team asks, “What would we need to do in order to
help?” May be a better opportunity to be a witness to coming to terms with
imminent death.
Shared
experience, with both participants on a more level playing field.
Win/Win.
This is a very complex and challenging aspect of Consultation-Liaison Psychiatry and, probably in part because we’re in short supply in many areas, many transplant centers rely on written assessment batteries or checklists. It’s hard to do justice to the topic in a blog post. I hope it’s helpful.
References:
1. Anne
M. Larson, J.P.R.J.F.T.J.D.E.L.L.S.H.J.S.R.F.V.S.G.O.A.O.S.W., Acetaminophen-induced
acute liver failure: Results of a United States multicenter,
prospective study. Hepatology, 2005. 42(6): p. 1364-1372.
2. DiMartini,
A.F., M.D.,, M.A. Dew, M.D.,, and P.T. Trzepacz, M.D.,, Organ
Transplantation, in Textbook of Psychosomatic Medicine, J.L.M.D.
Levenson, Editor. 2005, American Psychiatric Publishing, Inc.: Washington, DC.
p. 675-700.
3. Huffman,
J.C., M.K. Popkin, and T.A. Stern, Psychiatric considerations in the patient
receiving organ transplantation: a clinical case conference. General
Hospital Psychiatry, 2003. 25(6): p. 484-491.
4. Klapheke,
M.M., The Role of the Psychiatrist in Organ Transplantation. Bulletin of
the Menninger Clinic, 1999. 63(1): p. 13-39.
5. Novack,
V., et al., Deliberate self-poisoning with acetaminophen: A comparison with
other medications. European Journal of Internal Medicine, 2005. 16(8):
p. 585-589.
6. Turjanski,
N. and G.G. LLoyd, Transplantation, in Psychosomatic Medicine,
M.J. Blumenfield, M.D. and J.J. Strain, M.D., Editors. 2006, Lippincott
Williams & Wilkins: New York.
p. 389-399.
I get a big kick of this video every time I see it. It’s a
YouTube about people who are 100 years old who are funny, wise, and talented. It’s
included on the SSM Health St. Mary’s Hospital YouTube channel. St. Mary’s
Hospital is in Madison, Wisconsin. I worked as a psychiatrist there very
briefly a long time ago.
However, the other thing this video brings to mind is
something sad. I see patients half my age (nowhere near 100) almost every day
in the hospital who are delirious, sometimes for prolonged periods of time.
According to the medical literature, they will be at risk for developing
dementia and not infrequently do. In fact, research tends to show that for
every day someone spends delirious, the risk for developing dementia goes up
35%. That makes delirium a life-limiting condition which can happen to anyone
at any age.
I got delirious after a routine colonoscopy, a procedure to
screen for colon cancer and other pre-cancerous tumors that used to be
routinely recommended for those who reach 50. It was the worst 50th birthday
present a guy could ever get.
I was delirious probably because I got sedated with a
combination of Versed and Demerol. The worst part of the condition probably
lasted only a couple of hours at most following the procedure. But I was sure
wiped out the rest of the day.
I would have a tough time picking out the worst part of the
whole process, the bowel prep (guzzling a big jug of GoLytely which should be
called GoHeavily) or enduring the post-procedure delirium. It was probably the
latter.
I don’t remember much. My wife tells me that I kept
repeating something about not taking NSAIDs. I think there was something about
that in the informed consent and education materials that got sort of stuck in
one of my neurons. I kept sliding down in bed while I was in the recovery room,
which I was in for a little while longer than is usually expected.
Preventing delirium is a vital job for health care
professionals everywhere. We can’t prevent each and every case, but there are
definitely things we can do to mitigate the problem. One of the most important
goals is to try to minimize or avoid the use of certain offending drugs such as
anticholinergic and sedative-hypnotic agents.
It’s also good to remember that the population at highest
risk for getting delirious is the elderly and those who already may have
cognitive impairment.
Preventing delirium, based on current literature, means first implementing non-pharmacologic multicomponent interventions. These may require a large cadre of volunteers. The best example is the Hospital Elder Life Program (HELP) at Yale, which is copyrighted by Dr. Sharon Inouye. Six of the most important features to address:
–Normalizing electrolytes such as sodium and keeping
patients well-hydrated
–Mobilizing patients as much as possible, including getting
immobilizing devices such as foley catheters removed as early as you can
–Making sure sensory aids such as eyeglasses and hearing
aids are available
–Ensuring that medications are monitored so as to minimize exposure to drugs that are anticholinergic or sedating.
Anyway, working on preventing delirium and minimizing its
impact is an ongoing challenge. Keep the goal in mind: We want as many people
as possible to live well to 100.