This is just a reminiscence. I know the word “wherefores” in the title is old-fashioned, but I’m an old guy and so what? When I was a young guy living in Mason City, Iowa where I grew up, I could not afford to rent an apartment. Shortly after I became an emancipated minor, I was lucky to be able to rent a dormitory room at the YMCA at 15 North Pennsylvania Avenue. The building was placed on the National Register of Historic Places in 2002.
Reference: M, Ben and Clio Admin. “Mason City YMCA (1926-200).” Clio: Your Guide to History. September 30, 2021. Accessed May 10, 2022. https://theclio.com/entry/140366
I guess that makes me sort of historic too. It was built in 1926. I think it rents out apartments now. I recently read a Globe Gazette article about the beginnings of the YWCA on 2 South Adams and it was built in 1918. The current Mason City Family YMCA is located on 1840 S Monroe Avenue.
There is a local legend that bank robber John Dillinger and his gang stayed at the YMCA while planning their robbery of the First National Bank in 1934. Track star Jesse Owens stayed there briefly in 1937, starring for a basketball exhibition.
I recently read a Globe Gazette article on the web about the beginnings of the YWCA on 2 South Adams. As I said, it was built in 1918, but I don’t know when it closed. The YWCA sat empty for years until a couple of artists got a loan from a local realtor. They’re renovating it. (Zachary DuPont. “Old YWCA building takes strides toward renovation,” Globe Gazette on line, 10/29, 2021, updated 1/18/2022).
They plan to build artist studios on the 2nd floor, performance space where a basketball court is presently, a community area and art gallery on the first floor, and make single apartment/dormitory rooms cheaper than regular apartments (maybe similar to what the YMCA had many years ago, up to 12 units on 3rd floor). My wife, Sena, stayed there briefly and that was very helpful.
The YWCA is not on the National Register of Historic Places. It’s not clear why. The artists have raised some money with a GoFundMe campaign toward the renovation project. The website is titled “Save the Historic Mason City YWCA.” So why is it not on the National Register of Historic Places?
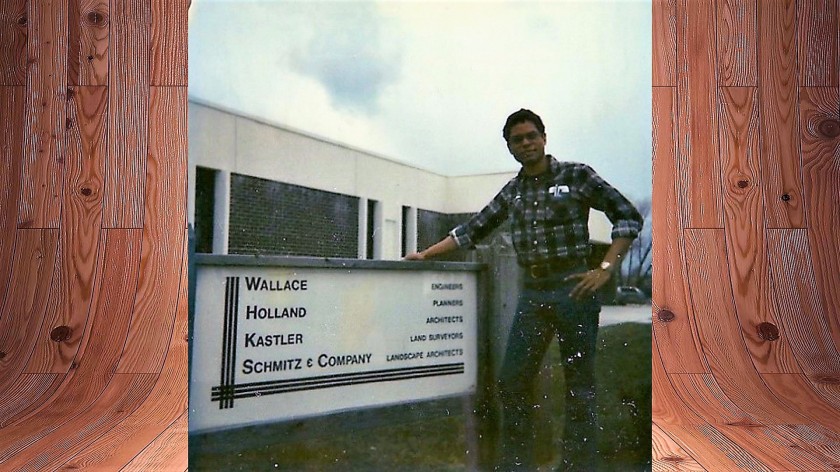
Anyway, I moved into a very cramped room at the YMCA on either the 3rd floor in my teens. I was working as a draftsman and surveyor’s assistant for WHKS & Co., a consulting engineering company. It was mainly a place to sleep. Most of the time I was traveling, working on out-of-town jobs such as relocating Highway 13 between Elkader and Strawberry Point (really more like straightening out all the curves in it), land surveys and the like.
I also have a distant memory of learning how to swim at the YMCA when I was a kid. I was terrified of even putting my face in the water and used to get fierce headaches just getting into the pool. I’m not sure how I got over it, but I did.
There were a fair number of eccentric characters who lived at the YMCA back in my day. I didn’t consider myself one of them and that’s probably why I didn’t end up staying there for decades. I could have worked in Mason City for the rest of my life, having breakfast at the café in the old Brick and Tile Building on East State Street, and eating all of my other meals in restaurants along Federal Avenue until I was too old to do much more than sit in Central Park.
But I didn’t. I’ll get to that.
There were a number of guys who stayed long term at the YMCA. It was kind of uncomfortable for that. There was only one communal bathroom and shower. There were no kitchens. There was barely enough room for a bed, a kneehole desk and chair, and you had to listen to the cast iron heater radiator clank most of the night. They were just sleeping rooms, but it was a little too loud to sleep sometimes because of the banging noise from the radiators.
I found out one of my neighbors was building a motorcycle in his room. He was very proud of it. It was a large machine and took up a lot of space. He kept it very clean. The Director of the YMCA at the time was John Calhoun and he’d been involved with the YMCA since 1943. He had a reputation for being pretty strict about the rules, which likely included one prohibiting the building of motorcycles in your dormitory room. We kept the motorcycle a secret of course.
There were some guys whose wives kicked them out of the house. They were always going out for coffee. They could drink a lot of coffee, smoke a prodigious number of cigarettes, and talk non-stop about how bad things were in the world in general.
There was an old candy bar vending machine on the floor. I got what must have been an ancient Butterfinger. I bit into it and found what I thought was half a worm wriggling around. Finding a worm was bad enough, but half a worm alarmed me. Where was the other half?
I even telephoned the local hospital emergency room to ask if I were in danger of some kind of poisoning. There was only a pay phone available at the YMCA, even for the guys who lived there. The ER doc couldn’t stop laughing long enough to say more than I’d most likely be just fine. “Fine,” he said. I haven’t eaten a Butterfinger since.
I met one guy who kept saying basically one thing over and over: “So my ancestors came over on the Mayflower. All well and good…” Then he would sort of trail off. His expression didn’t change at all. In fact, he looked flat most of the time. I didn’t know it at the time, but he probably had a chronic, severe mental illness.
I don’t remember who told me that the athletic director was gay. I don’t know if he was or not, and it didn’t matter. He treated everybody with kindness and respect and we treated him likewise. I remember he gave me sound advice about the safest length of time to spend in the steam room after I almost blacked out after sitting in there way too long.
I learned the dollar bill jump trick from an older guy in the weight room. He didn’t call it that, but it was a similar challenge. The idea is to bet you that you can’t bend over or squat, grab just your toes and jump over a broomstick—without letting go of your toes. I think he actually showed it to me and another youngster. We tried over and over. All we did was fall and laugh. It’s a good thing he didn’t make us bet.
There wasn’t much to do around there except play pool. There was this underfed-looking guy who used to play a deadly game of call shot eight ball. He amazed me because he worse eyeglasses that were as thick as pop bottle bottoms. I didn’t understand how he could even see his own hands. He won every game.
I know it sounds a little dull, living at the YMCA. On the other hand, I’d have probably been in a tight spot if the YMCA had not been there when I was young.
I read a Wikipedia article about the song in the late 1970s, “Y.M.C.A.” by the Village People. The author noted that in the early days of the YMCA, the single room occupancy dormitory rooms were for guys who moved to the city from rural areas to find work. Later, YMCA tenants tended to be youth “…facing life issues” or the homeless.
And I met Sena there. She switched jobs from working across the street at a school administration building to work at the YMCA.
I never hung out at the front desk as much as I did after she showed up. I pretended to read the newspaper a lot. She probably wondered why I was always there. We played bumper pool. I don’t remember who won the games, but I had trouble concentrating on my shots.
She does everything. There must be a God because she is God’s gift to me. I guess after all, I did just fine after eating half a worm.
Featured image picture credit: Pixydotorg.