This is just a short update on how phased retirement is
going. I’m back in the saddle. Last Friday I went back on duty on the
Consultation-Liaison Psychiatry service. I’m at 50% time. My step counter today
shows about 2 miles and 17 floors—a slow day. That’s fine with me.
Colleagues pass me in the hall and say, “I thought you were
retired.” They don’t look happy when I tell them I’ll be fully retired in June
next year.
But I’m a little happier. It’s taking a long time to get
used to not being a fireman, which is what it means around here to be a C-L
psychiatrist.
How’s the cooking going? Miserable but getting better, in a
way. I can deal with things like “Just Crack an Egg,” which my wife, Sena got for
me, as a sort of sympathy gift, I guess. I can handle it. And I made an omelet
the other day, my first ever. The kitchen was not filled with smoke and it was
edible.
How’s the exercise routine going? I’m still at it, 20
minutes every day, along with my mindfulness practice.
As I was giving my usual orientation remarks to the new
trainees coming on the service this morning, I caught myself saying “I do it
for the juice” when telling them why I do this schtick. I’ve said that to a lot
of residents and medical students over the years.
I guess I should rethink that remark and the mindset that
makes me say it so often. Pretty soon, I won’t be chasing all over the hospital
anymore— “for the juice.”
I’ve been trying hard to find something else for the juice.
Sena and I’ve rediscovered card games we haven’t played in over 20 years:
Pinochle and Gin Rummy. I lost track of time playing Gin yesterday, I had so
much fun. We just celebrated our 42nd anniversary. It was magical.
Starting this month, I’ve got a 10-month countdown to retirement. I was reminded of that when I got a brochure in the mail for the University of Wisconsin 7th Annual Update and Advances in Psychiatry. It’s scheduled for October 11-12, 2019 at the Monona Terrace, which is the usual location.
I’ve received these announcements in the mail every year for
longer than 7 years. I’ve never had the time to make it to a single of these
meetings. I’ve always been on duty. I’m not sure why they are advertising them
as though they started only 7 years ago.
I can remember getting an announcement in 2009 in which the
title of the update was Nontrivial Neuropsychiatric Nourishment from Noble
Notable Nabobs. How’s that for a sense of humor? There were several like that
prior to 2009 but I never kept the brochures. I haven’t seen any brochures like
that for the last seven years.
I don’t know who came up with the humorous titles. I wonder
if it was Dr. Jefferson. I noticed this year’s brochure had an In-Memoriam notice
about James W. “Jeff” Jefferson, MD, who has been a luminary of psychiatry for
decades. He was also a major presenter at these psychiatry advances meetings.
He was active in psychiatry for over 50 years.
And me? I’m retiring after a much shorter career, by
comparison. I’ve been running all over the hospital as a Consult-Liaison Psychiatrist
during the busiest time in academic medical centers everywhere–July and the
early part of August when senior medical students become full-fledged resident physicians.
Newly-minted doctors tend to request many psychiatric consultations. On average
I’m putting close to 4 miles and 30-odd floors on my step counter (with C-L
psychiatrists, maybe it’s not the years but the miles that count—literally). I’ve
not taken vacation during the past 2 years of my current phased retirement
contract—and don’t plan one for this final year.
That reminds me of time in 2012 when my wife, Sena, and I went
to Madison, Wisconsin on a vacation, the first in a long time. The residents
were wondering when I was going to get away. Madison is a great place to visit
and we lived there briefly when I took a stab at private practice.
We stayed at the Monona
Terrace, which gives a great view of Lake Monona. We loved Olbrich Botanical
Gardens. We rented a couple of bikes at Machinery Row Bicycles and rode all the
way to Olbrich. The rental bikes were a far sight more affordable than a lot of
the ones you could buy. Many were priced at several thousand dollars.
And I found an old copy
of Robbins Pathologic Basis of Disease at Browzers Bookshop on State Street. I
used that book as a medical student. My class used the nearly 7 pound red 3rd edition
containing 1,467 pages. This book is hailed as an outstanding foundational
text, which it is. Dr Stanley Robbins has been eulogized as an exacting editor
who championed writing of the type espoused by Will Strunk in The
Elements of Style.
Not to be picky, but the book contained the phrase
“not excessively rare” in reference to some process or disease which I can’t
recall. I do recall that a majority of our class howled about this verbiage,
which seemed the antithesis of what Strunk tried to teach.
You could see a lot of interesting sights on State Street. During
a previous visit, we saw a guy walking down the middle of the street with a rattlesnake
coiled on his head, wore it like a hat.
We had a lot of fun in Madison. It’s that kind of relaxed,
good time that I want to retire to. Ten months to go.
I updated my suicide risk assessment presentation today in
light of new data on suicide risk assessment stratification. It turns out that
using such tools might not be supported by the research evidence. That’s not
going to stop the use of such tools, which include the Columbia–Suicide
Severity Rating Scale, which is in wide use.
I found criticism of these scales in a recently published
article in Clinical Psychiatry News, published June 21, 2019, “Why we need
another article on suicide contracts,” by Nicholas Badre, MD and Sanjay S. Rao,
MD.
For many years now, psychiatrists and other health care professionals have learned that trying to use no-suicide or no-self harm contracts are controversial and don’t prevent suicide. Badre and Rao sound like they’re easing away from that contention although they still say that a thorough clinical suicide risk assessment ought to be done.
Until I saw this article, I was not aware of a recent review
of 70 studies showed that: “no individual predictive instrument or pooled
subgroups of instruments were able to classify patients as being at high risk
of suicidal behavior with a level of accuracy suitable to be used to allocate
treatment.”
Carter, G., et al. (2017). “Predicting suicidal
behaviours using clinical instruments: systematic review and meta-analysis of
positive predictive values for risk scales.” Br J Psychiatry 210(6):
387-395.
This was even more interesting because we recently changed our
practice regarding suicide risk assessments on the psychiatry consultation service
based on relatively new recommendations from the Joint Commission on
Accreditation of Hospital Organizations (JCAHO). The Joint Commission favors
the risk assessment tools.
Of course I’m not going to second-guess the Joint Commission
but after 27 years (counting residency) of struggling to assess suicide risk, I’ve
learned that it can hardly be reduced to any single rating instrument.
I have often said to patients that I don’t use no-suicide
contracts because they’re too much like promises—and promises are broken every
day. That segues into what I prefer which is to work with the patients on
developing a safety plan, which I compare to no-suicide contracts by saying “a
plan is better than a promise any time.”
Working on the safety plan with patients gives me another way
of assessing the strength of my alliance with them and a way to improve it as
well as a method for evaluating their ability to formulate a workable way to
stay safe that emphasizes their individuality.
On the other hand, the safety plan is no guarantee of safety,
any more than the no-suicide contract.
But often enough I’ve gotten the sense that some patients
and I have even had a little fun working on suicide safety plans—ironic as that
sounds. I find how important pets are, hear little anecdotes about a favorite hobby
or goal, aspirations, hopes, and memories of better times when they coped
really well.
Listening for understanding to someone who is contemplating suicide or who has attempted suicide is never easy. It’s the hardest thing I do. I can’t say that I’ll miss it when I retire. I have great faith in the next generation of doctors.
We saw this rabbit in our front yard
today, stretched out on the grass under our crabapple tree. It’s 117 degrees
this afternoon with the heat index and we won’t get out from under the Excessive
Heat Warning until later this evening. Thank goodness for air conditioning.
Rabbits don’t have air conditioning and can’t escape the heat.
Sena stands the heat better than I do; she waters the lawn and garden, keeping it beautiful. On the other hand, I felt body-slammed just walking out to get the mail.
Out in Sena’s garden
The old saying goes, “If you can’t
stand the heat, get out of the kitchen.” It means you if you can’t take the
pressure of a situation, then you should move and let somebody else take over.
It was popularized by President Harry S. Truman, who said the originator of the
proverb was Judge Buck Purcell of the Jackson County, Missouri Court—whoever he
was.
Anyway, I’m on call this weekend
and got to talking with a colleague who is thinking about retirement. We go
back a long way in our education and careers. He asked me about what phased
retirement is like. I told him I thought if I’d tried to retire outright, I
probably would have just come back to work.
That’s a twist on standing the heat. As a psychiatric consultant, I’m like a fireman (get it?) in the general hospital, putting out fires, so to speak, all over the hospital. Most often the problem still tends to be delirium, an acute change in mental status that should be considered a medical emergency rather than a psychiatric problem per se. It’s just one of many crises that I encounter every day. Over 23 years (not counting residency), I learned how to stand the heat in that kitchen. When I retire, somebody else will have to get in there and cook. Speaking of cooking—I still can’t.
I guess I’m mixing my metaphors
(fireman and kitchens, etc.). So what? I’m a retiring geezer and I guess I’ve
earned the right to mix my metaphors as much as I want.
But in my first year of the 3-year
phased retirement contract, I felt a different kind of heat–the heat of trying
to find something to do with my unstructured time. It was a struggle for a guy
who’s accustomed to being in almost constant motion, climbing up and down 20-30
floors (I hate waiting for elevators) and covering 2-3 miles a day.
The only trouble is—I can’t get out of the kitchen of retirement. I’m getting up there in age and even though most of the time, I seem to leave some of the trainees huffing and puffing getting up the stairs, I know they’ll replace me someday. But I can’t find a replacement to do my retirement time for me.
I have 11 months to go before I
retire. I can feel the heat.
I got an email from Don R. Lipsitt, MD yesterday which reminded me of the Janus Head logo for the Academy of Consultation-Liaison Psychiatry (ACLP). It was changed to another sort of nondescript logo several years ago for reasons I didn’t understand.
Dr. Lipsitt is a luminary in C-L Psychiatry and recently published a definitive history of the field, Foundations of C-L Psychiatry: The Bumpy Road to Specialization (2016).
Go ahead; buy this book!
I posted a blog or two about Don and his book in a previous blog, The Practical C-L Psychiatrist. We’ve never formally met. A few years ago, he noticed that I had written about him and his book. I had sent him an email message about it at around the same time the APM was considering the name change for the organization, telling him that I had plugged his book and asking him what he thought of the name change. Incidentally, he thought both of our books made a great package, so I guess I’m allowed to plug mine, strangely titled Psychosomatic Medicine: An Introduction to C-L Psychiatry, editors James Amos and Robert Robinson (2010).
Go ahead; buy my book, too…
Don expressed his
opinion about the name change:
“I feel I have dealt with that at some length in my book. I
still feel C-L is most fitting and that the Board made a big mistake naming it
PM. Who were they? Any C-L psychiatrists among them? Any Psychosomaticists? Why
are not the “complex medically ill” a special population? And why is
APA now offering courses on “integrated” care (which is what C-L
psychiatry has always been about? The notion that C-L was not
declared a specialty because it was considered a skill of ALL psychiatrists
(with minimal training), then how do geriatric or child psychiatry become specialties
(that all psychiatrists also have training in)? Don’t get me started.”
He considered his book, in large part, a “polemic” against
the name “Psychosomatic Medicine.”
Anyway, the ACLP was formerly the Academy of Psychosomatic
Medicine (APM) until a couple of years ago when the organization responded
robustly to the membership (of which I was one at the time) to abandon the term
“Psychosomatic Medicine” and adopt what rank and file practitioners
preferred—Consultation-Liaison Psychiatry.
It was a kind of rebranding and it was not the first time
the academy had considered a name change. I and a lot of other C-L
Psychiatrists cringed at the term “psychosomatic,” not so much because of the
word itself in terms of its true denotation, but because of the unfortunate
negative connotations it had acquired.
Another luminary of C-L Psychiatry, Dr. Thomas Hackett, MD,
wrote about the term “psychosomatic” in the Massachusetts General Hospital:
Handbook of general hospital psychiatry: edited by Hackett and Ned Cassem
(1978):
“The term ‘psychosomatic service’ has had a variable
history. The term generally leaves a bad taste in the mouths of physicians. It
reminds them of the 1930s, 1940s, and 1950s, when various psychosomatic schools
espoused doctrines linking specific psychological conflicts or unique
personality profiles with diseases designated as psychosomatic. Compounding
this misunderstanding has been the term’s abuse by the general public, who
regard anything psychosomatic as either imaginary or nervous in origin. As a
consequence, most people believe that a psychosomatic disease is not to be
taken seriously.”
Well, anyway, because of my anecdotage, I’ve strayed a
little from my original story about the Janus head logo.
I already mentioned that the logo was abandoned in favor of something that looks like waves and could lead to seasickness. I inquired about the history of the use of the Janus head logo.
In addition to my curiosity about why the logo was changed, I also wondered why it was chosen in the first place and when. According to Don, it was part of the organization’s journal, Psychosomatics, in the late ‘60s and ‘70s. What was interesting is that it was already in use by the Journal of Geriatric Psychiatry when the Psychosomatics editors started using it. However, a conflicting view was that it was not introduced to the cover until 2010. Hmmmm.
I saw the 2012 issue of the APM Newsletter had a pretty funny picture of Drs. Shuster and Rosenstein posing as Janus and the statement “Thank you, Janus. You served us well for over 50 years.” That might put the origin of the logo, at least, around 1962 although my understanding is that APM was started in 1953 (TN Wise, A Tale of Two Societies, Psychosomatics 1995).
Time to say “Hello, again, Janus?”
It’s
just my opinion, but because Janus is the ancient god of beginnings and
transitions, gates, doorways, endings and time, and typically depicted as
two-faced because he looks to the future and the past, I think the symbol is a
better image for what C-L Psychiatry has been through over the years.
Anyone for re-rebranding and go retro back to the Janus head logo?
Again today, I hoofed it around the hospital. I put 43
floors and a little over 4 miles on my step counter.
I don’t like waiting for elevators so I take the stairs. And
a Consult-Liaison Psychiatrist is like a fireman, running all over putting out
fires.
I did other things today. I gave the usual lecture on
delirium and dementia to the medical students. I notice that as I have gotten
older, I tend to tell more anecdotes about my experiences managing delirium in
patients on the medical side of the hospital.
I’m in my anecdotage, as I told the students today.
I also lamented the decision by the powers that be to
copyright the Montreal Cognitive Assessment (MoCA). The medical students will
be able to use it for free, but faculty won’t.
I think that’s ageism. I won’t pay so I won’t use the MoCA anymore.
Well, I’m pretty tapped out, so it’ll be a short post today.
I’m back in the saddle, running around the hospital on the psychiatry consult
service. This is my last year of phased retirement and in 11 months—I’ll be fully
retired.
I put 36 floors and 3 miles on the step counter. I’m feeling
every one of those. Sena bought me some banded collar shirts and I’m wearing
those instead of a shirt with a necktie. I don’t need a tie bar.
And I don’t worry about a delirious, violent patient
strangling me with my necktie.
We had a small scare tonight. We were looking at my total compensation statement (the last one) and got the Sharp Elsi Mate EL-505 vintage calculator out to crunch some figures. The calculator went dead.
Still going…
I put some new batteries in it, hopeful. It still didn’t work. We’ve had this calculator for over 30 years and it ran more than a decade on the first set of AA batteries.
I tried another pair of batteries. It worked! The vintage calculator lasted longer than the batteries. It’s nice to know that just because something’s old doesn’t mean it’s useless.
Most of this post is an updated redux from years ago about an
informal bedside test for delirium called the oral trails test. I learned about
it from my senior resident when I was a junior psychiatry resident in training
at the VA Medical Center.
There was an elderly patient admitted to the psychiatry unit
who was thought to be psychiatrically ill but who actually seemed confused to
me and the senior resident. We consulted medicine in order to get him transferred
to the general medicine unit but it was tough going. I think the medicine
resident disagreed with our clinical impression that he was confused and didn’t
think medical transfer was necessary.
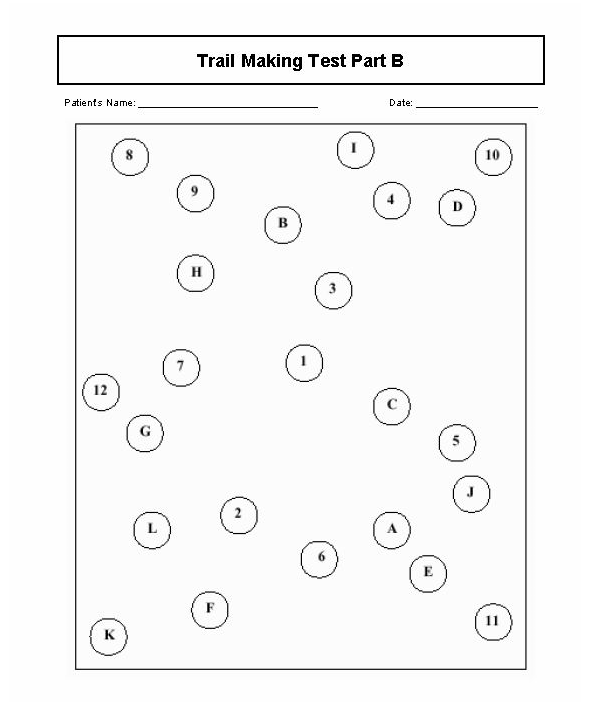
Anyway, my senior resident showed me her version of the oral version of the mixed Trails A and B Test for executive function. There is a written form which is part of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). First, she asked him to count from 1 to 7; then she asked him to recite the letters of the alphabet from A to J. She then asked him to try reciting those letters in alternating sequence. Of course, he failed miserably and was eventually transferred to internal medicine. The Trails actually is a paper and pencil test and it looks like a dot to dot game, like the example below:
Trails Test
My senior resident told me she learned the oral Trails test
from her senior resident and couldn’t remember anything else about it. I used
the test for years but a neuropsychologist criticized the practice, questioning
the test’s validity, and rightly so.
Of course, I’d been doing it wrong. You’re supposed to have
the patient count to 25, then recite the letters of the alphabet, then recite
the numbers and letters in alternating sequence from 1 to 13 and A to M. More
than two errors in pairings indicate cognitive impairment.
There are limitations to the verbal Trails and caution is
advised in more recent literature, indicating that there are moderate education
effects in older patients and that it may be wiser to use both paper and pencil
and oral versions together.
Still the search goes on for quick and dirty ways to screen
for cognitive impairment in the elderly because this and advanced age are two
main risk factors for delirium.
Nowadays, I do the Mini-Cog (shown in the video below) or the Single Question in Delirium (SQiD) test, which just involves asking a family member if the patient seems confused lately.
References:
Mrazik, M., Millis, S., & Drane, D. L. (2010). The oral
trail making test: effects of age and concurrent validity. Archives
of clinical neuropsychology: the official journal of the National Academy of
Neuropsychologists, 25(3), 236–243.
doi:10.1093/arclin/acq006
Sands, M., Dantoc, B., Hartshorn, A., Ryan, C., & Lujic,
S. (2010). Single Question in Delirium (SQiD): testing its efficacy against psychiatrist
interview, the Confusion Assessment Method and the Memorial Delirium Assessment
Scale. Palliative Medicine, 24(6), 561–565. https://doi.org/10.1177/0269216310371556
OK, my top ten YouTube videos are going to get pretty low ratings anyplace else. But where else are you going to see the list but on my blog? In a world where popular videos are viral at a million plus views, I’m way in the back yard.
I wasn’t very picky, of course, because these are the videos
I made. I didn’t include any others, especially the ones that were
professionally produced. I kept the bar pretty low because I had to. Any video with
over 900 views made it to the list, which goes from lowest to highest number of
views.
By the way, the only way I could come up with a Top 10 list
was to make the bar 900.
10. “Dr. Jim Amos’ Dirty Dozen on Suicide Risk Assessment” published
2012: 940 views
9. “Dr. Jim Amos’ Dirty Dozen on Alcohol Withdrawal
Treatment” published 2012: 1,063 views
8. “Dr. Jim Amos’ Dirty Dozen on Catatonia” published 2012:
1,668 views
7. “Mall of America Video” published in 2016: 1,728 views
6. “Dr. Jim Amos’ Dirty Dozen on Interpersonal Psychotherapy”
published 2012: 1,840 views
5. “Dr. Jim Amos’ Dirty Dozen on Catatonia, NMS, Serotonin
Syndrome” published 2013: 1,960 views
4. “Dirty Dozen on Dr. Allen Frances’ Dozen General Tips on
Psychiatric Diagnosis” published 2013: 2,492 views
3. “Pseudobulbar Affect Top Ten” published 2015: 2,613 views
2. “Dr. James Amos’ Dirty Dozen on Somatoform Disorders”
published 2012: 8,191 views
1. “Dirty Dozen on Factitious Disorder and Malingering”
published 2012: 12,465 views
Now why would a video about abnormal illness behaviors like
Factitious Disorder and Malingering be number one?
And why would “Mall of America Video” be my most popular
non-work-related video? My wife and I did have a lot of fun there.
I like to think people enjoy “Pseudobulbar Affect Top Ten” because of my superb pseudo-rap acting style—and my hat.
Here’s a redux of one of my blog posts from years ago. There’s
not been much change in the data or clinical practice regarding delirium,
except we’re even less enthusiastic about using any kind of psychotropic
medication to treat delirium, even hypoactive delirium. Try the puzzle.
“So, you want to put on a game show contest to educate clinicians about delirium? Contact David Meagher, a psychiatrist in (where else?) Limerick, Ireland. He reported on this innovative educational workshop in the November 2010 Vol. 3 issue of the Annals of Delirium, the newsletter for the European Delirium Association (EDA). He also published the study which describes the contest in International Psychogeriatrics [1].
The workshop focused on clinician attitudes toward drug
therapy for distressed delirious patients. It explored pre-existing attitudes
and practice toward the use of medications to manage delirium and exposed
participants to a very interactive educational event modeled after a popular TV
quiz show. There were two teams (skeptics versus neuroleptics) furnished with a
list of statements about delirium pharmacotherapy. The participants later
completed a post-workshop questionnaire that explored changes in attitudes as a
result of the workshop.
The participants were all experts on the subject and there
was a good deal of variability in attitudes and practice. Some of the questions
put to the teams involved using antipsychotics prophylactically to prevent delirium,
the mechanism of action of antipsychotics, and what role benzodiazepines play
in the treatment of non-alcohol withdrawal delirium.
One of the more puzzling findings was that the frequency of
antipsychotic use was inversely proportional to the perception of the strength
of supporting evidence. In other words, the less they knew about
antipsychotics, the more often they used them. Most participants seemed to
believe that the principal mechanism of action of antipsychotics is sedation,
despite the lack of supporting evidence.
Some clinicians used antipsychotics to relieve the stress of
caregivers rather than that of delirious patients, an example of patients
getting the right treatment for the wrong reasons as observed by Meagher—and
many of us in the field.
The workshop also highlighted the tendency of clinicians to
focus on risk management rather than effective therapeutic intervention in the
management of delirious patients with disruptive behavior and severe distress.
This mainly relates to focus on the potential adverse effects of antipsychotics
such as extrapyramidal side effects, metabolic, and cerebrovascular effects.
The quiz show activity was fun and challenging. The device
of dividing the participants into two small teams with larger audience participation
cut down on the anxiety that could be provoked by giving the “wrong answer”.
The questions were true/false and didn’t always have clear right or wrong
answers. It was highly interactive, a component of continuing medical
educational (CME) activities that is increasingly encouraged because it’s more
likely to lead to changes in clinician attitude and practice. The one time
Grand Rounds CME “seat time” is going the way of the dinosaur.
So a couple of findings from the quiz show post-activity
questionnaire were that clinicians were more likely to use antipsychotics
prophylactically and to use antipsychotics to manage hypoactive delirium.
Our delirium
intervention project group members are not quite as enthusiastic yet about
these two interventions. We’re a bit more inclined at least initially to focus
on non-pharmacologic multicomponent strategies such as the example below:
Minimize the use of immobilizing catheters,
intravenous lines, and physical restraints
Avoid immobility, early mobilization
Monitor nutrition
Provide visual and hearing aids
Monitor closely for dehydration
Control pain
Monitor fluid-electrolyte balance
Monitor bowel and bladder functioning
Review medications
Reorient communications with the patient
Place an orientation board, clock, or familiar objects
(i.e., family photographs) in patient rooms
Encourage cognitively stimulating activities such as
word puzzles
Facilitate sleep hygiene measures, including
relaxation music or tapes at bedtime, warm drinks, and gentle massage
Minimize noise and interventions at bedtime, e.g., by
rescheduling medication times
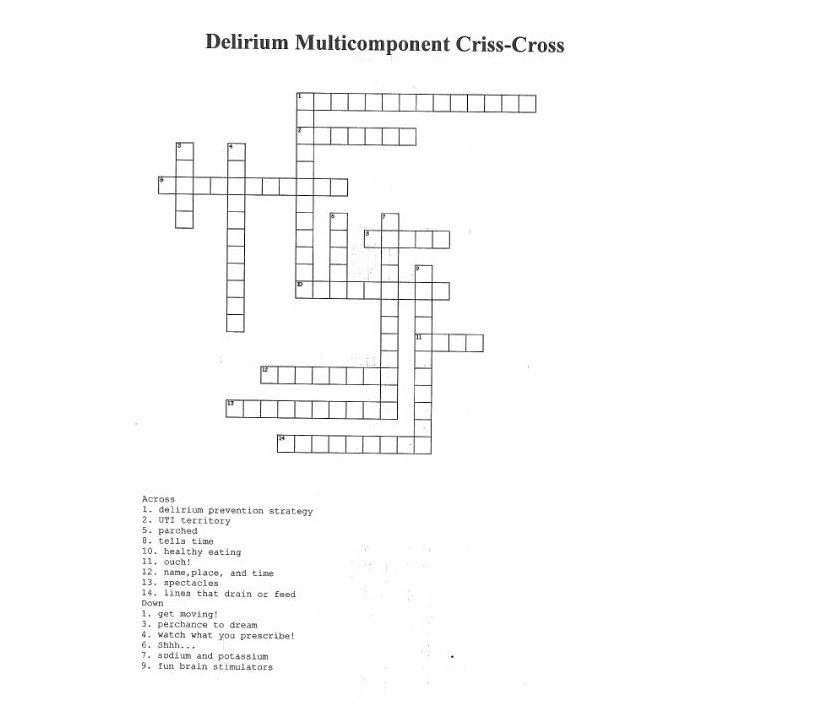
But I’m just as enthusiastic about interactive educational methods to engage learners in order to build a culture more likely to produce champions who will lead the delirium prevention effort—try the delirium multicomponent crisscross puzzle below. The clues are contained in the list of multicomponent tactics above.”
Meagher, D.J., Impact of an educational workshop upon attitudes towards pharmacotherapy for delirium. Int Psychogeriatr, 2010. 22(6): p. 938-46.