I’ve thought about my weight over the past few days and decided to look at a few pictures. I had not realized that I had lost about 20 pounds over the last several years. This was all intentional and I’ve shed about 7 of those in the last six months—due mainly to daily exercise including planks.
Planks are good
As a consulting psychiatrist, I thought I was getting plenty
of exercise running all over the hospital, up and down stairs and whatnot. The
trouble is that it’s stop and go, fireman-type activity that often isn’t
sustained over much time.
I’ve got a few pictures of me before I lost my paunch. It’s
funny that I’m not climbing 20 or 30 steps and getting a couple of miles or so
on my smartphone step counter—yet I’m probably a lot more fit off the job than when
I was on. That could also partly be from not eating quite as much for lunch
when I’m not working.
Retiring has overall been better for my health.
It just occurred to me while writing this post that a couple of the pictures might not make much sense. They were taken during a Psychiatry Department Residents vs Faculty matball match and picnic several years ago. If you don’t know what matball is, you can find out more about it here.
I didn’t play, but I suppose that’s obvious. Maybe it’s also why Faculty lost.
We’re just a bit on the sad side today. The robin chicks are gone. It’s another empty nest and sort of the story of our yard over the last month or so, what with the loss of the house finch and cardinal chicks before this.
It’s a hard life for every creature. On the other hand, death in our own yard is always counterbalanced by the triumph of life elsewhere on earth.
That doesn’t make it any easier. I’m reminded though of a
quote attributed to Sydney Harris:
“When I hear somebody sigh, ‘Life is hard,’ I am always tempted to ask, ‘Compared to what?’”
Sydney J. Harris
I’m pretty sure he never, ever actually asked that question.
This was a blog post I wrote back in 2011 on another blog, The Practical C-L Psychiatrist. SQiD is short for Single Question in Delirium and it’s a very short and effective screen for delirium, if you have a reliable informant. I also mention the Edinburgh Delirium Test Box (EDTB). It has been further developed into a smartphone app.
“The November Vol. 3 issue of the Annals of Delirium
published a summary of an interesting study of a Single Question in delirium
(SQiD) as a screen for delirium compared to the Confusion Assessment Method
(CAM), the Memorial Delirium Assessment Scale (MDAS) and a psychiatrist
interview[1].
The question “Do you think (name of patient) has been more
confused lately?” was put to a friend or relative of 21 patients. Compared with
psychiatric interview, the SQiD achieved a sensitivity and specificity of 80%
(95% CI 28.3-99.49%) and 71% (41.90-91.61%) respectively. The CAM
demonstrated a negative predictive value (NPV) of 80% (51.91-95.67%) and the
SQiD showed an NPV of 91% (58.72-99.77%). The CAM in the study had only a 40%
sensitivity used by minimally trained clinical users.
The negative predictive value of a test tells you how likely
it is that you actually don’t have the condition or disease. It’s defined as the
number of true negatives (people who test negative who are not affected)
divided by the total number of patients who test negative and it varies with
test sensitivity, test specificity, and disorder prevalence. The sensitivity of
a test is how accurately it detects patients who are positive for the disorder
(in this case delirium). If 100 patients are positive for the disorder, then a
test that is 80% sensitive will detect 80 of those cases and miss 20 actual cases
of the disorder. Specificity is defined as how accurately a test detects
patients who do not have the disorder. In our delirium example, if 100 patients
are free of the disorder, then a test that is 71% specific will correctly tell
71 of those people that they are not affected and will incorrectly tell 29 that
they have the disorder when they don’t.
This seems to suggest that a single question screening
question packs a fair punch compared to screening instruments and psychiatric
interview for identifying delirium. The CAM takes a few minutes to complete and
requires training to achieve optimal identification rates.
The authors suggest the SQiD deserves further study and
their results seem to support the conclusion. The study is limited by small
sample size, but intuitively the premise is appealing. This is one of the
quickest tests for delirium applicable and can be applied by almost anyone.
Single question screening exams for depression are not
unheard of so there is precedence for the SQiD. You just have to be careful
about what you say in front of patients and families. “Go ahead and run the
squid on Mr. Jones” could raise a few eyebrows.
This is possibly a low tech solution in a pinch when the CAM
forms file is empty or the battery is low on the Edinburgh Delirium Test Box
(EDTB)[2].
The EDTB is a more high-tech solution to testing for what neuropsychologists
believe what one of the main abnormalities is in delirium—lack of sustained
attention. It’s a computerized neuropsychological testing device.
And that face-off would be called SQiD versus Box.”
References:
1. Sands, M., et al., Single Question in Delirium (SQiD): testing its efficacy against
psychiatrist interview, the Confusion Assessment Method and the Memorial
Delirium Assessment Scale. Palliative Medicine, 2010. 24(6): p. 561-565.
2. Brown,
L.J.E., et al., Detecting deficits of
sustained visual attention in delirium. Journal of Neurology, Neurosurgery
& Psychiatry.
This is a short Coach’s Corner video on somatoform and
related abnormal illness behaviors which prompt physicians to request
psychiatric consultation. Medically unexplained physical symptoms are not rare
in the hospital and in medical clinics.
The general idea is to remember Stephen Covey’s caution about effectiveness and efficiency, which is that you have a lot better chance being effective rather than efficient with people.
“With people, slow is fast and fast is slow.”
Stephen Covey
The point is that it’s very important to listen for understanding and to validate pain and suffering. That means sitting with patients and taking time to hear what they tell you.
There is an excellent presentation on conversion disorder (also known as functional neurological disorder) on the National Neuroscience Curriculum Initiative (NNCI) web site. It’s very helpful for clinicians and patients.
Well, it has been about 3 months since I opened this blog. My YouTube channel needed an updated channel trailer, so I’m posting it here as well. Why not?
I was surprised at how long a minute and a half channel trailer took to make, even with the aid of video editing software (maybe because of it, partly).
In my situation, a channel trailer is sort of a mini biography. It’s hard to compress a career into a short clip that takes about 5 minutes to upload to YouTube–after a few hours of what was essentially cut and paste.
As you can gather, my path is changing. Over the next 12 months, I’ll be half off and half on the consultation-liaison psychiatry service. That’s according to the terms of my phased retirement contract.
This is really a re-introduction, of course. I’m slowly evolving–not in any big way. I’m still a geezer.
On the other hand, I have found that I’m much more comfortable being on some kind of schedule. I still get up early, only by about an hour later. I generally arise between 5:30 and 6:00 a.m. That may seem very early to some.
I eat less when I’m off service (which I’ll call “retired” for simplicity). That’s probably why my trousers fit more loosely.
I need to have something to do. I exercise daily, for about 20 minutes. I do mindfulness meditation and yoga. I blog. I photograph and film, mainly birds, which I post to YouTube.
The only reason I ‘m not a disaster in the kitchen is because you generally can’t get me within 10 yards of it unless I need a snack I can immediately eat (like an apple). I still don’t cook–not really. It’s embarrassing.
I trim the lawn and by that, I mean just around the walkway edges and some of the garden margins. I don’t mow the lawn because my wife does a much better job, by mutual agreement.
I’m not a gardener. I’m a garden appreciation expert. That means I watch gardening that is done by others.
This is just a quick post updating the saga of our robin family in the front yard crabapple tree. It looks like all 4 chicks are alive and kicking so far.
The parents are very protective. The male robin won’t fly away unless I’m just close enough to touch him. The female is about the same.
I’m anticipating a busy time next month on the psychiatry consultation service. I suspect delirium will be the main event, as it is most of the time.
So I made a very short YouTube video on delirium. It’s cast in the style of a coach’s corner because I was one of the many clinicians who won the Excellence in Clinical Coaching Award this year.
It’s getting close to the busiest time of the academic year in a teaching hospital–July. The residents have a steep learning curve during that month. Some hospitals have a sort of boot camp to get the upcoming first year internal medicine residents prepared for July.
I’m looking at my retirement countdown timer and it’s showing I have 12 months to go. I’ll be back in the saddle July 1st.
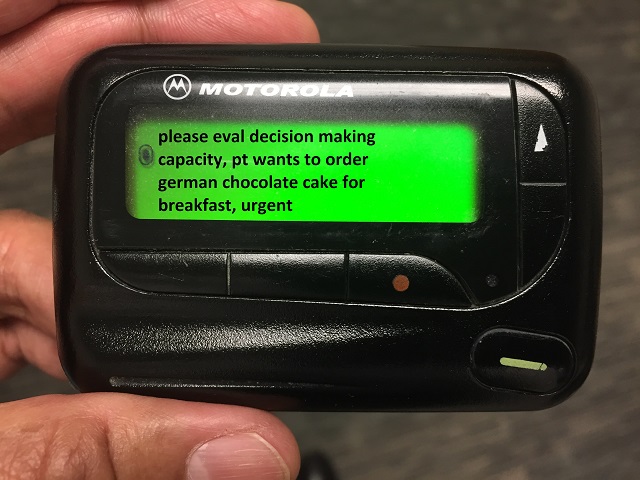
July is usually the time for the most interesting psychiatry consultation questions. Many years ago, the psychiatry residents used to keep a list of the weirdest ones. At least that’s what they claimed. Actually, I think most of them were simply made up–maybe all of them. Even though there is no way to know for sure, there is very low probability that any item on the list below could identify any patient.
We used to call it the “wailing wall” of strange and difficult to answer psychiatry consultation questions sometimes asked by our non-psychiatry colleagues from internal medicine and surgery. Questions have been and still are sometimes ambiguous (worse in July) and often need to be reframed so that the psychiatric consultant can be helpful to both customers—the patient and the consult requester. Here are some “quotes” from probably fictitious consultation requests tacked to wailing wall in the distant past, certainly embellished in some cases by frustrated psychiatry residents:
1. “EEG shows no brain activity.”
2. “The patient doesn’t like me.”
3. “We want to know
if the patient who believes they are Sponge Bob and wants to leave the MICU to
start filming a new movie—is competent.”
4. “I’m a
humanitarian but can you transfer this patient to Mexico?”
5. “The patient looked at me funny.”
6. “We are wondering
whether to discharge to their own apartment a patient who is oriented only to
self, cannot perform activities of daily living, and is actively
hallucinating?”
7. “I prefer not to speak with my patients.”
8. “I prefer not to speak with families.”
9. “Patient gets irritable during “that time of the month.”
10. “We are wondering
if the patient should be taken off sedation before getting a history from
them?”
11. “Patient swallowed their narcotic sobriety pin and is upset that morphine was discontinued.”
12. “The patient is eating their fingers off.”
13. “Cardiac arrest.”
14. “Consult for bilateral disorder or generalized panic disorder.”
15. “Anxiety and agitation 5 minutes before Code Blue.”
16. “Please evaluate for catatonia versus brain death on intubated patient.”
17. “Patient was fine
yesterday but now unresponsive. Please rule out catatonia before we work up. If
catatonia ruled out, we’ll then get a head CT and labs.”
18. “We want the consult for our own safety.”
19. “We need psychiatry’s blessing before we can feel comfortable discharging the patient.”
20. “Patient admitted for renal failure after being gored by a bull at a rodeo, please evaluate if this was a suicide attempt.”
Some are humorous and a few are mind-boggling. What they all speak to is the omnipresent opportunity for the C-L psychiatrist to excel as an educator. Reframing the question is a skill that requires patience, diplomacy, and credibility as an expert in this field.
What’s the question again?
What this may also indicate is the necessity to include a bit more about psychiatry in medical school clerkship programs.
It rained for about an hour or so before I could get out to
the crabapple to check the progress of the robin hatchlings. Yesterday there
were two unhatched eggs but there was a definite hole in one of them.
There are now 4 hatchlings, although the biggest one looks
pretty sluggish—and appears to sport a fair-size blister on its butt.
It’ll be at least a week before they look like anything but
a light snack for a crow. They’ll get to that little dinosaur stage a few days
beyond that. It’ll take a couple of weeks before they fledge—at least the ones
who survive. This would be the first time I’ve been able to get video clips.
Last year I got snapshots for a little slideshow.
Baby robins last year
I was surprised at how close the parents allowed me to get.
I could have reached out and touched them.
Sena mentioned seeing small birds flying out of the Colorado Blue Spruce on the other side of the front yard. I looked long and hard before I found anything that resembled a nest. Frankly it looks like something that could have been in use last year.
Another nest?
On the other hand, I also noticed the branches shaking in
that tree later in the afternoon. And I recall seeing a chipping sparrow streak
out of there, perch on the crabapple and chirp at me—nervously.
Yesterday, we noticed 4 eggs in the Robins’ nest. They take
about 14 days to incubate and it just so happens time’s up today.
Right on cue the eggs started cracking this morning. It
takes all day and it was well after 3:00 PM before there was the tiniest
pinhole in the third egg. Two chicks were squirming around when I finally
called it a day around 4:30 PM.
This will have to be continued…. Hope it’s not raining tomorrow.