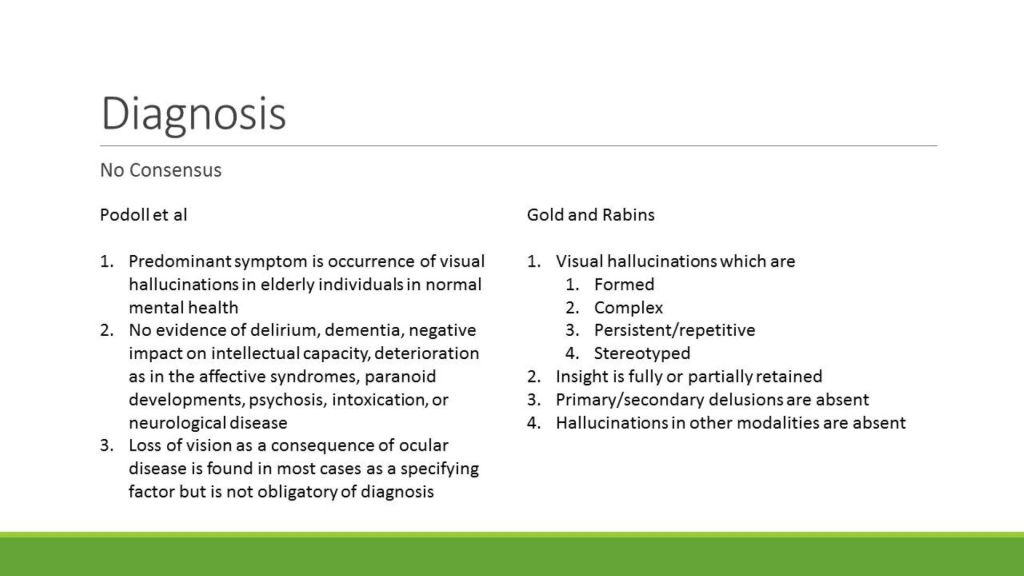
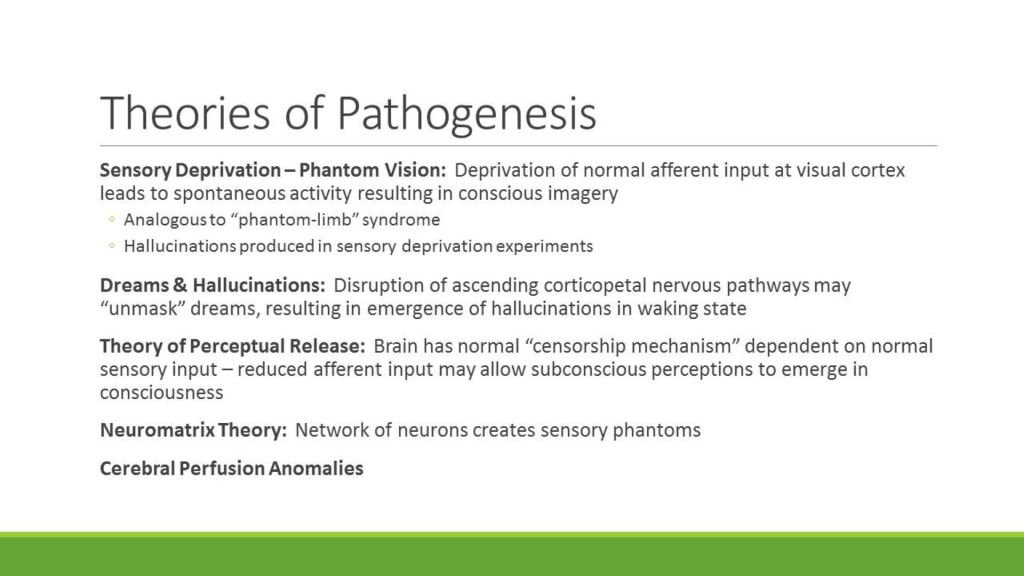
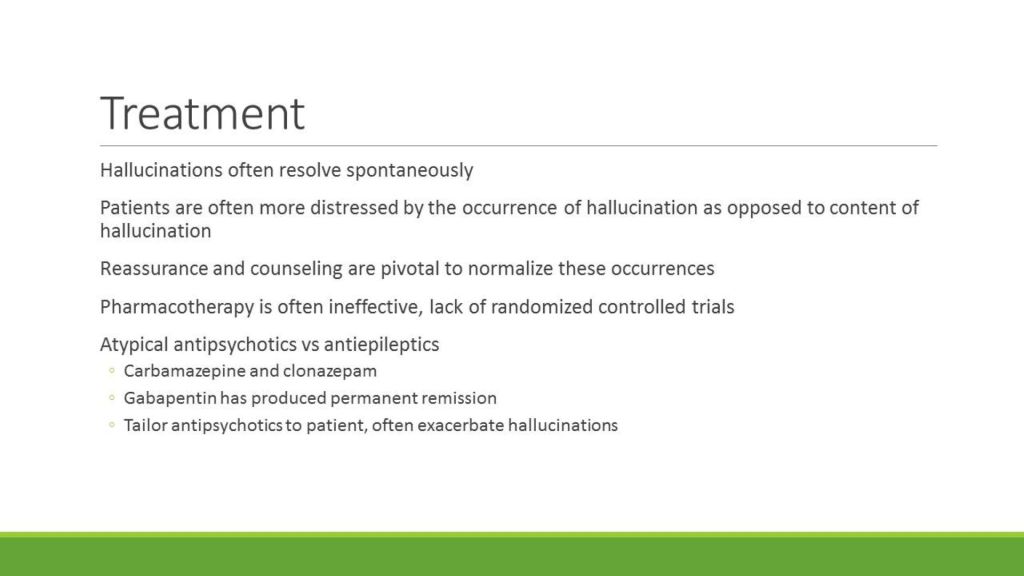
I ran across an old Clinical Problems in Consultation Psychiatry (CPCP) presentation by a couple of sharp medical students in 2014. They presented it at one of my morning consult rounds and it’s about Charles Bonnet Syndrome.
They did a very nice job and it compares fairly well with the University of Iowa Ophthalmology Dept summary. One of the authors of that summary is my retinal specialist, Dr. Ian Han, who did the surgery on my detached retina about 4 years ago. It also has a link to a great YouTube video of a woman who has Charles Bonnet Syndrome. It’s not a psychiatric disorder although ironically one of the treatments for it may sometimes be antipsychotic medications.
The other thing about this presentation is that the students’ fictional case description mentions that the patient had visions of “a break-dancing koala bear” among other things. I can’t remember whether I was the one who told them about a video on the internet that showed a break-dancing stuffed koala bear—or if it was the other way around! At any rate, I remember seeing it around that time, but of course I can’t find it now.
I was thinking about the Clinical Problems in Consultation Psychiatry (CPCP) learning sessions which was introduced to me by one of my first teachers in the University of Iowa Dept of Psychiatry, Dr. William R. (Bill) Yates.
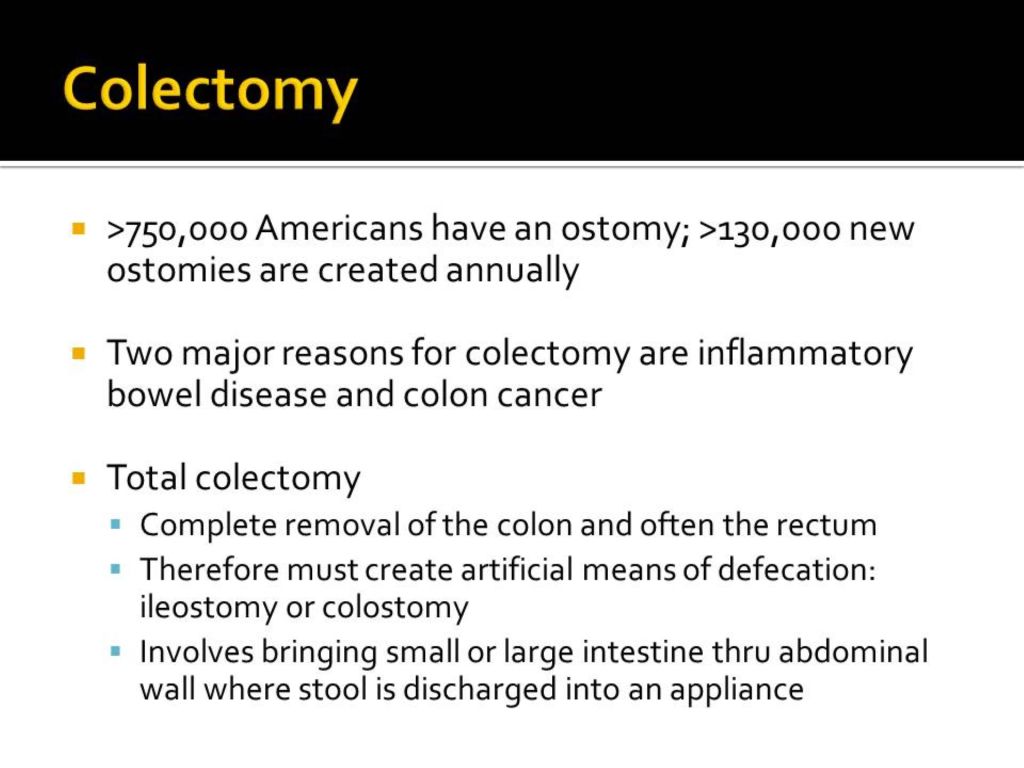
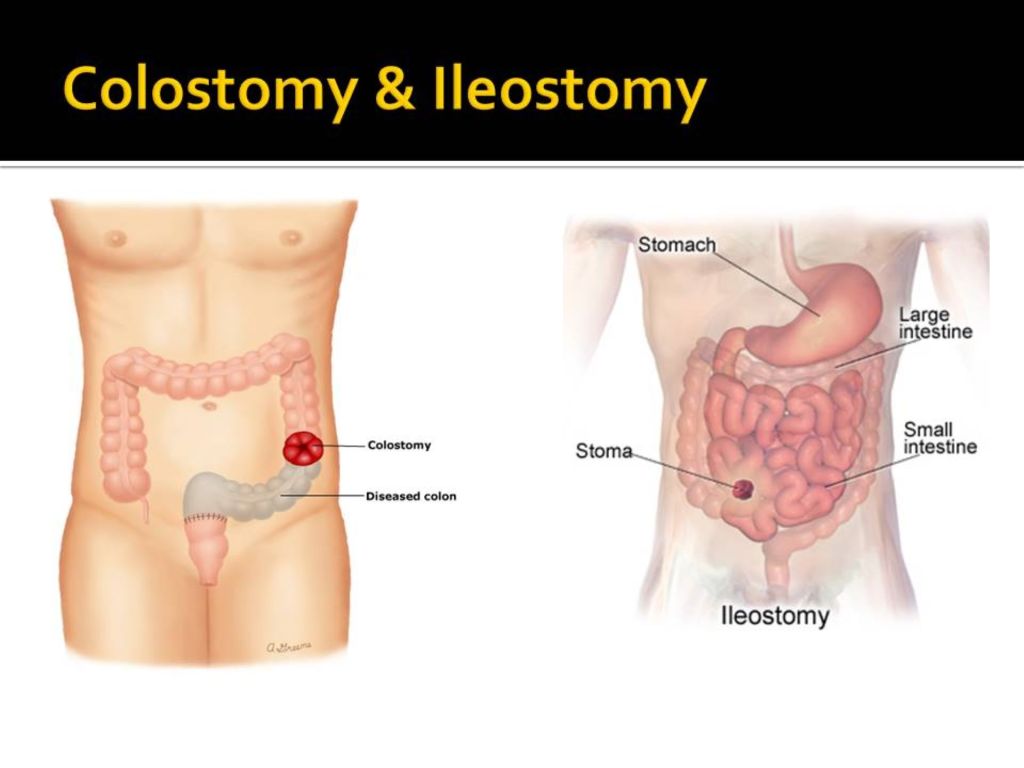
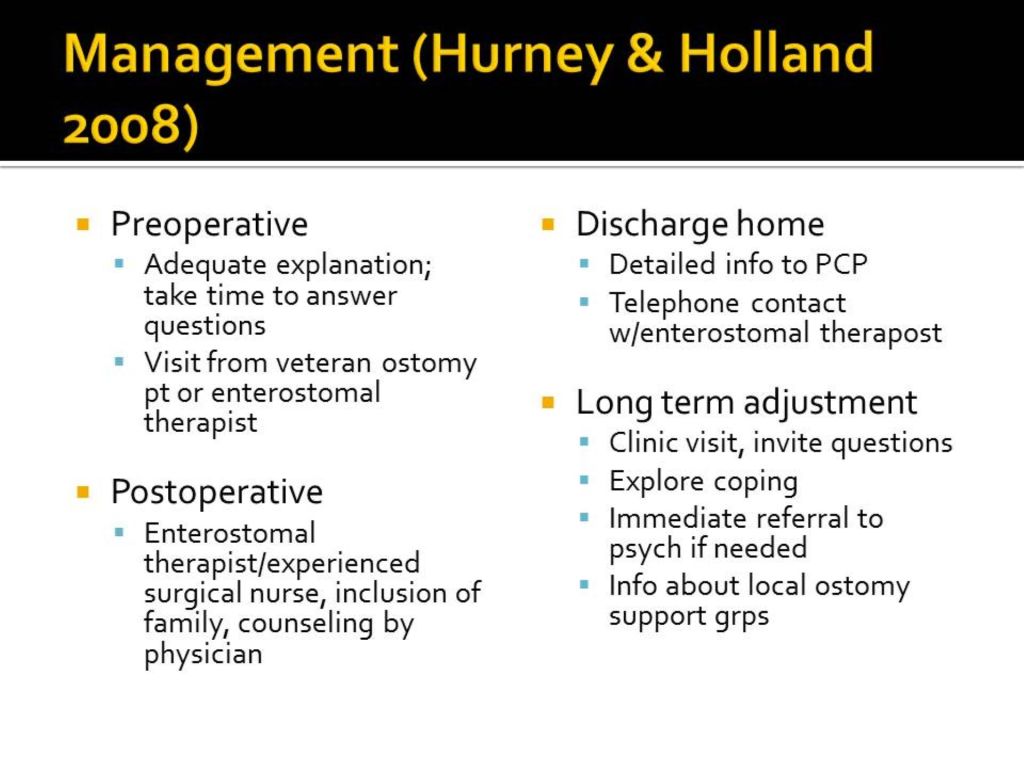
I had originally been thinking of posting one of my own CPCPs that I presented in 2015. It was about the psychosocial adjustment of patients to ostomy.
I searched widely and in vain on the web for any recent information about what Dr. Yates was doing now. I was surprised and saddened to discover his obituary. He died on January 19, 2023 in Tulsa, Oklahoma.
As the obituary says:
He served on the faculty at the University of Iowa for Psychiatry and Family Medicine before becoming Professor and Chair of Psychiatry at the University of Oklahoma College of Medicine in Tulsa. After retiring, he continued to dedicate his time as a volunteer research psychiatrist at OU and the Laureate Institute for Brain Research where he also served on the board of directors. He authored over 100 scientific manuscripts that were published in peer-reviewed journals.
He was an energetic, a great teacher, had a great sense of humor, and was easy to get along with. He published in many scientific journals and taught many trainees. He was an avid bird watcher and his blog Brain Posts highlighting neuroscience research findings is still visible on the web.
He published the paper along with a chief resident on problem-based learning used on the psychiatry consult-liaison service in 1996, the year I graduated psychiatry residency and joined the faculty at The University of Iowa Hospitals & Clinics (Yates, W. R. and T. T. Gerdes (1996). “Problem-based learning in consultation psychiatry.” Gen Hosp Psychiatry 18(3): 139-144.) You can read the abstract for it along with a description of the CPCP at the link above which takes you to my April 19, 2019 blog post “Clinical Problems in Consultation Psychiatry.”
When he was the leader of the psychiatry consult service, we were still using paper charts and his staffing comments were always very brief and encapsulated the assessment and plan succinctly without wasted verbiage—contrasting with my long-winded note.
His remarks about his role at Laureate Institute for Brain Research is still accessible:
“I work part-time as a research psychiatrist for the assessment team at the Laureate Institute for Brain Research. We do research diagnostic assessments for a variety of imaging, genetic and biomarkers studies in mood, anxiety and other brain disorders. I also provide review and analysis of neuroscience research on my blog Brain Posts that can be found at www.brainposts.blogspot.com. You can follow me on Twitter @WRY999. I also use my blog and Twitter feed to share my bird photography images.”
I respected and admired Dr. Yates, as I’m sure many learners did. I will always remember Bill as a gifted scientist and teacher.
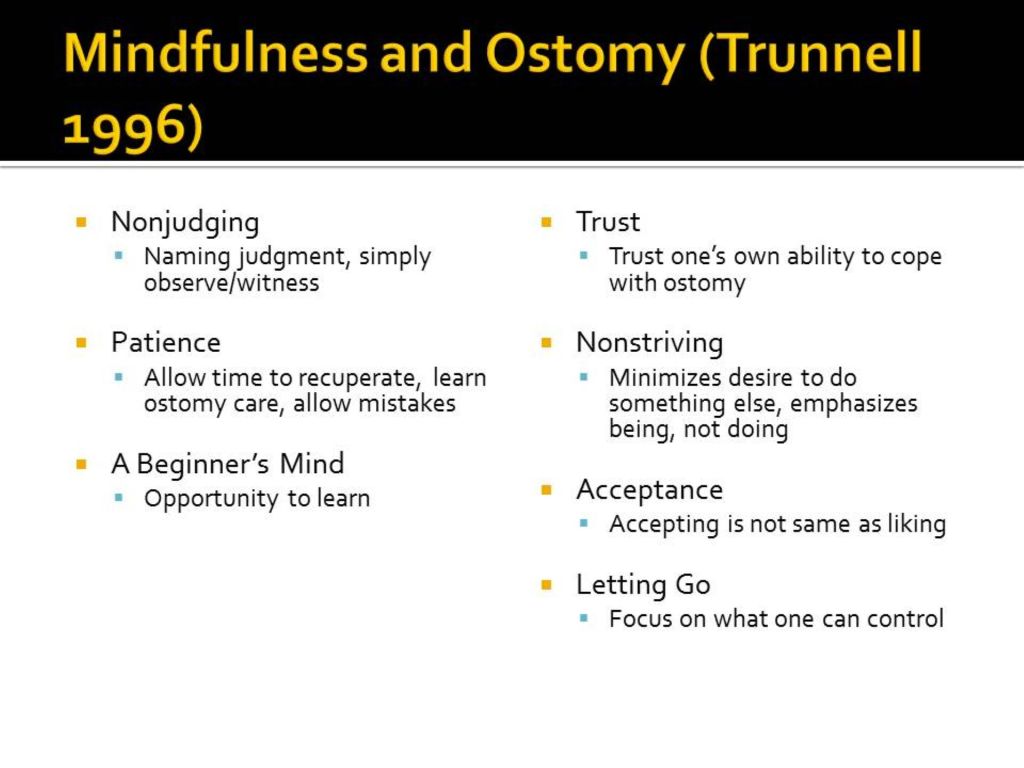
I think a fitting tribute would be to go ahead and post my CPCP on the psychosocial adjustment of patients with ostomy. One of the most interesting articles in the bibliography is how the mindfulness meditation approach to that adjustment can be very helpful. The website United Ostomy Association of America website is also informative.
The presentation is also limited to a dozen slides. I often encouraged learners to keep the number of slides to a managed number so the presentations wouldn’t run too long. I called my slide sets the Dirty Dozens.
Many thanks to Dr. William R. Yates and my condolences to his family.
Dr. H. Steven Moffic discussed the issue with psychiatric polypharmacy in his August 29, 2022 entry on Psychiatric Views on the Daily News. The patient who had been getting 10 psychotropic drugs was found to have a medical problem ultimately, which led to simplification of the complex regimen.
This is a great opportunity to again mention the value of what was a regular part of the teaching component of the University of Iowa Hospital Consultation-Liaison Psychiatry service, at least until my retirement. This was the Clinical Problems in Consultation Psychiatry (CPCP) seminar. Once a week or so, when I was staffing the service, I and the trainees, which included medical students, and psychiatry residents as well as Pharmacy, Neurology, and/or Family Medicine residents.
Whenever we encountered a difficult and interesting case, which was almost every rotation, the trainees did a literature search to bone up on the clinical issue and gave a short presentation about it before consultation rounds. Often the case had both medical and psychiatric features.
I looked through my collection of student presentations and found one that might fit Dr. Moffic’s example in a general way. Medical problems can often look like psychiatric problems, which can include thyroid and other diseases. A very important one is autoimmune encephalitis, one example of which is anti-N-methyl-d-aspartate (NMDA) receptor encephalitis. There is an excellent summary of it in the August issue of Current Psychiatry entitled Is it psychosis, or an autoimmune encephalitis? (Current Psychiatry. 2022 August;21(8):31-38,44 | doi: 10.12788/cp.0273).
Several years ago, three medical students tag-teamed this topic and delivered a top-notch CPCP seminar summarizing the pertinent points. I hope the CPCP is still part of the educational curriculum.
Long day on the C-L Psychiatry service. I logged 2.8 miles and 33 floors on my step counter. I barely had time to eat lunch. This post is going to be short.
We were treated to outstanding presentations on fascinating topics over the last couple of days and they were given by top-notch medical students. One of them summarized the literature on mental illness in the population of incarcerated women. The other was a great overview of catatonia.
The students put a lot of work into them. The data search was obviously thorough and their presentations were polished. They had very well organized PowerPoint slides.
They were among the best examples of Clinical Problems in Consultation Psychiatry (CPCP) learning sessions in recent memory. The CPCPs were a frequent feature in my previous blog, The Practical C-L Psychiatrist.
The CPCP was developed by a former teacher of mine, William R. Yates, MD. He was the head of the C-L Psychiatry service years ago before moving on to the University of Oklahoma in Tulsa.
He’s a part time research psychiatrist for the assessment team at the Laureate Institute for Brain Research. They do research diagnostic assessments for a variety of imaging, genetic and biomarkers studies in mood, anxiety and other brain disorders.
The CPCP format is:
A weekly case conference held Wednesdays from 8:00 a.m. to
approximately 8:45 a.m. Each week, a case is selected from the Daily Review
Rounds Records to illustrate a clinical problem for the next week’s
meeting. The residents are assigned dates when they rotate. The medical
students are welcome and even encouraged to participate as well.
This is a practical way to approach teaching the
Practice-Based Learning & Improvement Core Competency. This helps develop
the habit of reflecting on and analyzing one’s practice performance; locating
and applying scientific evidence to the care of patients; critically
appraising the medical literature; using the computer to support learning and
patient care; facilitating the education of other health care professionals.
This is applying principles of evidence-based medicine (EBM) to clinical
practice.
Evidence-based
medicine is a systematic approach to use up to date information in the
practice of medicine
Skills
are needed to integrate the available evidence with clinical experience
and patient concerns
Application
and evaluation of EBM skills will provide a frame-work for life-long
learning.
Self-evaluation is vital to the successful practice of EBM:
Am
I asking answerable clinical questions?
Am
I searching the literature?
Am
I becoming more efficient in my searches?
Am
I integrating my critical appraisals into my practice?
The assigned resident is responsible for searching the
literature and selecting one or two teaching papers for the conference.
Presentations will begin with a review of the case, followed by a summary of
the references with subsequent round table discussion.
Circulate copies of 2-4 pertinent articles to team members
including psychiatric nurses and faculty. A copy machine is available in the
departmental administration office. Consult staff can also assist with
obtaining copies.
Presentations begin with a 5-minute summary of the case with discussion of both psychiatric and medical aspects of evaluation and management. The remaining time is spent summarizing the pertinent data in the articles. Residents and medical students are encouraged to use the case conference material as preparation for submitting a case report or letter to the editor.
Bill and a former chief resident of psychiatry, Dr. Terri Gerdes, published a paper about the CPCP (then called problem-based learning in consultation psychiatry) in 1996:
Yates, W. R. and T. T. Gerdes (1996).
“Problem-based learning in consultation psychiatry.” Gen Hosp
Psychiatry 18(3): 139-144.
Abstract: Problem-based learning (PBL) is a method of instruction gaining increased attention and implementation in medical education. In PBL there is increased emphasis on the development of problem-solving skills, small group dynamics, and self-directed methods of education. A weekly PBL conference was started by a university consultation psychiatry team. One active consultation service problem was identified each week for study. Multiple computerized and library resources provided access to additional information for problem solving. After 1 year of the PBL conference, an evaluation was performed to determine the effectiveness of this approach. We reviewed the content of problems identified, and conducted a survey of conference participants. The most common types of problem categories identified for the conference were pharmacology of psychiatric and medical drugs (28%), mental status effects of medical illnesses (28%), consultation psychiatry process issues (20%), and diagnostic issues (13%). Computerized literature searches provided significant assistance for some problems and less for other problems. The PBL conference was ranked the highest of all the psychiatry resident educational formats. PBL appears to be a successful method for assisting in patient management and in resident and medical student psychiatry education.
The year that was published was the first year of my appointment to the Clinical Track faculty in the department of Psychiatry at The University of Iowa Hospitals and Clinics. I learned a lot from Bill.
And I’m confident that the students who presented their own CPCPs this week will teach many other trainees in their careers.