Today is the first day of Martin Luther King, Jr. Human Rights Week and I’m giving a shout-out for acts of kindness as well as the Loving-Kindness meditation. A neighbor with a snowblower helped clear our driveway a couple of weeks ago. A couple of days ago he did the same for his next-door neighbor. I’m going to go out on a limb and speculate the city snowplow driver was kind enough to avoid plugging the driveways on our street. No kidding, we watched the snowplow use what was obviously a different plowing technique which left our driveways relatively clear of snow.
The Loving-Kindness meditation is a mindfulness practice that Dr. King would probably have supported. It’s a way to send love to yourself and others, including those with whom you might be in conflict—even your enemies. King might say, “Now is the time” for something like that.
I’m reestablishing my mindfulness and exercise practice after a several month lapse. I first took the Mindfulness-Based Stress Reduction (MBSR) course several years ago through The University of Iowa Hospitals and Clinics. It made a difference in how I approached problem-solving and conflict. I was on autopilot most of the time and wrote a blog post about my experience before and after my mindfulness training experience, “How I left the walking dead for the walking dead meditation.”
Part of that program included instruction on the Loving-Kindness meditation. I’m still a beginner at mindfulness, although my approach to life is still ironically more like the expert’s in Shunryu Suzuki’s quote:
“In the beginner’s mind, there are many possibilities, in the expert’s mind there are few.”–Shunryu Suzuki
I need to keep working on being more open to different ideas, interpretations, and ways of getting things done—approaching challenges with a beginner’s mind.
One recent challenge is hanging pictures. Sena and I hung a picture yesterday. I wanted to measure everything and she wanted to estimate. She had misgivings about my measurements but went along with it. After the picture was hung, even I had to admit it was not in the right spot. Funny thing, after a short while, she admitted that the misplacement was not that far off and that she was getting used to it. If you’ve ever hung pictures, you know I’m leaving out a lot of the back-and-forth negotiation about how we finally arrived at that middle ground. It involved loving kindness on both sides.
I know I promised to observe National Nothing Day, but I learned something new today about Dr. Martin Luther King, Jr, and I figured I’d write a little something. Actually, I was not idle. So much for Nothing Day.
Dr. King liked jazz music, especially bebop. Dr. King said this about jazz: “When life offers no order and meaning, the musician creates an order and meaning from the sounds of the earth which flow through his instrument.”
Sena and I like smooth jazz, which doesn’t highlight improvisation as much as bebop—and that’s about all I know about jazz. I’m really more of a blues, rock and roll, and classical fan. I’m not really much of an improviser, I guess. I rely on recipes and frozen pizzas when I fix meals, which thank goodness is infrequent. Sena doesn’t use recipes and changes things up a lot, not just in the kitchen.
I found out that King even alluded to a jazz musician’s composition in his “I Have a Dream” speech at the Lincoln Memorial in Washington, D.C. in 1965. A friend of King shared that the civil rights leader had used the refrain “Now is the time” from Charlie Parker’s 1945 classic tune.
“Now is the time to make real the promises of democracy. Now is the time to rise from the dark and desolate valley of segregation to the sunlit path of racial justice. Now is the time to life our nation from the quick sands of racial injustice to the solid rock of brotherhood. Now is the time to make justice a reality for all of God’s children.”
I’m just guessing, but I think Parker probably improvised his music a lot. On the other hand, as I’ve grown older, I’ve pretty much scripted what I do in my life. When I was much younger, I improvised more. It’s a common path. There’s nothing especially wrong with regularity and predictability—bowel movements come to mind as one example. I’m a geezer after all.
But sometimes my relationships with others might have been helped if I had been a little more spontaneous, a little nimbler and more flexible with my attitude and responses. I guess that goes for all of us.
Now is the time to do something about that. It’s not too late.
I’m writing this post because I just found out that tomorrow is National Nothing Day, so I won’t have a chance to write it then. Ever heard of it? The legend is that a San Francisco Examiner humor columnist, Harold Pullman Coffin, created it in 1973, probably in reaction to the proliferation of holidays in general. National Nothing Day falls on January 16 and “observing” it means you do nothing all day.
How you do nothing is up to you. The holiday from doing leads into the idea of nothingness, one example of which might be outer space. The notion that nothing is out there and that we’re alone in the universe is always up for debate. In fact, in a recently posted science news item, the author announced a study finding that there are “only” a few hundred billion stars out there, not 2 trillion as previously estimated. Therefore, that makes it more likely earthlings are alone in the universe.
No kidding, that’s what the author concluded. I couldn’t find that conclusion in the study’s findings, but I didn’t read much between that and the introduction. It’s pretty technical.
I’d like to hear your thoughts about whether we’re alone in the universe. I don’t know whether life is out there on other planets, but I hope so. The feeling of being alone in the universe sometimes makes me a little gloomy.
I’m reminded of quotes from Men in Black 2 (what doesn’t remind me of Men in Black movies?). Agent J asks his partner, Agent T, “T, when was the last time we just looked at the stars? Then he asks, “Ever get the feeling we’re alone in the universe?” Agent T says “Yes” and then a second later says “No” because he thinks the questions are some kind of test he needs to pass. When Agent J offers to buy him a piece of pie, Agent T puts his arm around him and says reassuringly, “Hey, you’re not alone in the universe.”
You could ask why Agent J, one of the Men in Black agents who police and monitor all alien life on planet earth, would ask such a question at all? He’s busting the chops of beings from other planets every day. I think what he means is that he feels alone for a different reason. He had to give up his identity as a regular person in order to be one of the Men in Black. No one can ever know him—or love him. You’ll have to watch the movie to see how that works out.
On the other hand, feeling alone in the universe is a pretty big deal to many people. In fact, for astronomers and non-scientists, it’s intriguing to speculate about it. What are humans doing here anyway? What is earth, besides being a planet in one of the many galaxies? What other life forms could be out there and what’s our relationship to them?
What if earth is some sort of exile or prison planet? Remember the 1981 movie, Escape from New York, with Kurt Russell as Snake Plissken and Lee Van Cleef as Hauk? Manhattan is the maximum-security prison for the entire country. I’m not knocking New York City; we loved our visit there several years ago. I got a senior discount on my ticket for the visit to the top of the Empire State Building.
“I’m not jumping off of this building!”–Agent J in Men in Black 3 on the Chrysler Building in New York City
Another example is Men in Black 3, in which the heavy, Boris the Animal (“It’s just Boris!”), an intergalactic psychopathic alien, was imprisoned in Lunar Max, a supermax prison on the dark side of our moon.
The Ancient Alien theorists have ideas that are just as speculative. We’re the Martians; we have alien DNA zipped into our own. Some people believe they are abducted by aliens, who conduct weird experiments on them. The kind of questions that arise echo that of the character Newton in Men in Black 2: “What’s up with anal probing? Aliens travel billions of light years just to check out our…” Newton gets abruptly interrupted by the impatient Agents K and J, but I think his question is good.
I’ve noticed there a lot more TV shows with UFO content now. Some of them talk about recently declassified documents from the military and the government. People are interviewed who have been told never to reveal what they’ve seen and heard—by supposedly real Men in Black and military officers. The witnesses come forward and discuss their experiences with fear on their faces and a few of them probably wish they’d been neuralyzed.
I don’t know what to think of it, except that sometimes I wonder if maybe we’d be better off if we were truly alone in the universe. By the way, remember to do nothing tomorrow. This will confuse the aliens.
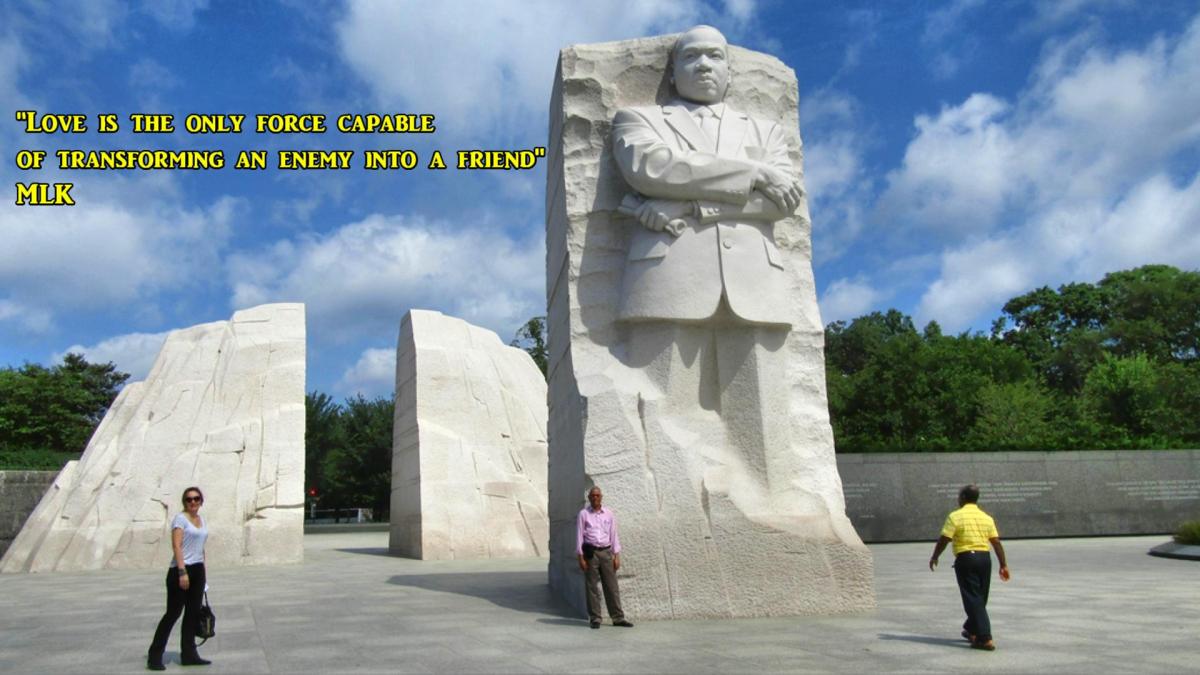
As I struggle to remember to write and say the year “2021” I noticed the University of Iowa Health Care quotation selection by Dr. Martin Luther King, Jr this month pertinent to the upcoming MLK Human Rights Week, starting January 18, 2021:
“Love is the only force capable of transforming an enemy into a friend.”
It’s funny because, as usual, the way my sense of humor works, I also recall quotes from the movie Men in Black 3. Agent K asks Agent J, “Do you know the most destructive force in the universe?” Agent J answers with a wisecrack, “Sugar?” Agent K replies, “Regret.”
Then what is the most constructive force in the universe? Dr. King thought it was love.
Since my retirement in July of last year, I’ve had a lot of time on my hands. It leaves me with too much time to reflect on my current life as a retired psychiatrist—and my past life as a consulting psychiatrist. As my thin veneer of authority, responsibility, and other lies I tell myself drop away, I become more aware of my flaws in both roles. I find deep holes in my identity as a person as my identity as a doctor fades. Just being a person who has a lot to learn about life despite being a psychiatrist—is hard. I have regrets and remorse. My sense of humor sometimes helps me get by.
Dr. Martin Luther King, Jr and me in Vegas.
Regret can indeed be a destructive force. Though it’s similar to regret and painful, remorse could help me be a better person. It becomes more and more important that I find something constructive, both to do and to be.
Maybe love is the most constructive force in the universe. Because quotes are sometimes misquoted and inaccurately attributed, I googled the quote “Love is the only force capable of transforming an enemy into a friend.” I found the sermon from which I think the quote is derived on a Stanford University web site. It’s called the “Loving Your Enemies” sermon and it’s published in the book, A knock at midnight: inspiration from the great sermons of Reverend Martin Luther King, Jr.
There are YouTube and Vimeo videos of an audio recording of the sermon as well. The internet being what it is, you apply hyperlinks to these and other works at the risk of the links being broken at some point, which I have found and which might be due to uncertainty about whether the text of the sermon is in the public domain.
As an aside, I’m reminded of a quote variously attributed to Charles Schulz, creator of the Peanuts comic strip, Fyodor Dostoyevsky, and others: “I love mankind; it’s people I can’t stand.” This probably betrays my skepticism about the ability to love your enemies.
You know, it’s funny. I didn’t find the Dr. King quote, word for word, the first couple of times I scanned it in the Stanford University transcript. What I did was the thing most junior medical students do when they discover the vast load of information they have to memorize and digest. I scanned the sermon for the key words and didn’t see them.
Nor did I find it on the third read, in which I finally abandoned the scanning method and actually read the sermon. But I got the point.
If the Stanford version and my reading are accurate, what I found were probably the main ideas I needed to make sense of the sermon. King said that I have to look deep within myself first before attempting to understand anyone else, much less to love my enemies. I also would do well to look for the good in people who I judge are bad. Moreover, I gain nothing by trying to defeat my enemies. He even mentions the theories of psychologists and psychiatrists to support his profound conclusions. As I read them, I was acutely reminded of my shortcomings as a psychiatrist. You would think a psychiatrist would know how to analyze himself (and psychoanalysts do undergo analysis in training). I am not a psychoanalyst. But I am capable of reflection.
The exact quote might not be discoverable (at least to me) in King’s sermon. Nevertheless, the transformative and redemptive power of love is clearly expressed. The quote is distilled from the text of the sermon. That doesn’t mean that there might not be a different version of the sermon which could have contained each and every word. According to one writer, that may be the case. Perhaps it’s in the book, A Knock at Midnight: Inspiration from the Great Sermons of Martin Luther King, Jr.
What is more important for me at this time of my life is to accept that my search for the most constructive force in the universe will proceed in baby steps.
What I need to do is reflect on my own shortcomings and find ways to improve while avoiding making excuses. Stephen Covey said that we often blame our parents or our grandparents for our flaws. This was part of his three theories of determinism to explain man’s nature. Genetic determinism says I inherited my flaws from my grandparents (whom I never met), which implied my mistakes were encoded in my DNA. Psychic determinism supposedly explains what I got from my parents because of their mistakes in rearing me. Hmmm, I was exposed to fruitcake at Christmas. Environmental determinism implicates says that other people in my workplace, my school, my neighborhood or my country (politicians perhaps?) caused my flaws.
Covey disputed these ideas by the example of Viktor Frankl’s personal triumph over his experience as a prisoner in a Nazi death camp. His captors controlled his liberty to move about his environment. They could not control his freedom to choose what he thought and felt. He controlled his self-awareness, imagination, conscience, and independent will to draw meaning from his experience [The Seven Habits of Highly Effective People: By Stephen R. Covey. New York: Simon and Schuster, 1989].
How can I see the good in my enemies, despite their obvious flaws in comparison to my own angelic perfection? And how to avoid acting on the urge to defeat them, despite the reality that there have to be winners and losers at all levels in society, including elections, sports, cribbage (at which my wife regularly beats me)? Something tells me I’m getting off to a shaky start here.
I have to crawl before I can walk; I have to walk before I can run—before I fall flat on my face for the umpteenth time. Now more than any other time in my life, I must keep trying. I must get up and try again.
ADDENDUM January 11, 2021: I tried to access the King Library and Archives (KLA) today at The King Center website. There is a message indicating the KLA page is down indefinitely and redirects the reader to the Stanford University site noted above.
Day before yesterday was the eve of Christmas Eve. We ventured out on the blustery day despite the forecast for winds in excess of 40 mile per hour. We got started late in the morning and the temperatures dropped like a rocket in reverse about an hour later because of wind chill. A thin film of ice formed on the lake and it looked like the geese were leaning into the wind, which was blowing hard out of the southeast.
It almost looked like the water fowl were listening for something. In fact, we thought we heard a low-pitched hum when the wind was gusting the hardest. Sena heard it first. It came and went. I think we heard it best when we looked up at a patch of cloud-filled sky on the east side of the trail. One cloud looked sort of like a turtle’s head to me, although Sena thought it looked more like a pig’s head. The hum seemed more noticeable there.
There was a fair amount of excitement several years ago about seemingly pervasive low-pitched hums and many people were very sensitive to the noise. Some of them said it make them miserable. There is even a Wikipedia entry about the phenomenon. One guy even recorded it. I’m not sure if it’s the same sound, but it was similar. I didn’t think it was unpleasant; just odd. It’s unlikely you’ll hear it in our YouTube video, but then again, your hearing may be much keener than mine.
A heavy sign with the word “Skating” on it got knocked down by a powerful gust. We watched a very strong guy set it upright—it blew over again moments later.
Along with the wind, a blizzard was predicted for the Midwest, but it missed us. We barely got enough snow to sweep off our porch.
Merry Christmas! I hope Santa watched out for those crosswinds.
The first supply of the COVID-19 Vaccination vials arrived at the University of Iowa Hospitals and Clinics (UIHC) this week. We couldn’t have wished for a better Christmas gift. As a recent UIHC physician retiree, I know first hand how hard everyone works there. They live the motto: We Stand Together. UIHC is making history—and they’ve been doing that for a long time.
This is just a brief announcement—a Kindness Alert. This past Saturday, we got our first load of snow of the season dumped on us, which meant we had to go out and shovel. Our driveway is pretty big. We don’t have a snowblower. This means we were out there about an hour and a half powering our way through a few inches of wet, heavy snow.
And naturally, that meant the city snowplows plugged in our driveway shortly after we went inside, foolishly congratulating ourselves on a job well done. I think there must be some kind of local ordinance requiring all driveways to be plugged with snow right after the homeowners finish clearing them. I’ve posted about this before.
But then as we watched from our front window, our neighbor interrupted his own snow removal work to clear off our driveway plug and then some. In fact, he used a snowblower and a shovel! He spent considerable time on the job. It was an impressive act of kindness. I remember wanting to rush out in the cold to thank him.
Little did I know that I would have the opportunity to return the favor. Shortly after our neighbor finished, another snow plow rumbled through and dumped more show in our driveway and even spread it around more generously in other places near the curb—and even shoved snow over the curb on the lawn. By that time, the stuff had frozen into small boulders of ice and mud.
I plodded outside again and cleaned it up. Then I noticed that the snowplow driver had also piled more snow on my neighbor’s side. In fact, I did return the favor—sooner than I thought I would.
A big shout-out for my neighbor’s act of kindness!
A couple of days ago, Country Arborists cleaned up the debris left behind in our back yard from the derecho that smacked Iowa in August 2020. They are wild, flying tree warriors. That was a scary storm and if the straight-line winds had blown in a slightly different direction, our house would have been all but demolished.
Like a lot of other people in the state, we’ve been clearing tree limbs. But the massive oak was beyond any tool we owned.
The view from our window was a constant reminder of the derecho. The fallen oak was broken but not separated high up and we had to leave that kind of work for the professionals. Many of the tree removal pros have been extremely busy. Some are scheduling out to a couple of years from now. Country Arborists are just as busy, but made time for us anyway.
We had no idea what was involved in tree removal jobs of this magnitude. When they arrived last Friday, one of the first things they noticed about our back-yard trees was one which they identified as possibly a Native American Trail Marker Tree. This summer, Sena noticed this odd, old tree which was bent at right angles.
Native American Trail Marker Tree
Anyway, I filmed the work they did, which was spectacular. They rigged a rope system which allowed one of them to cut the trees at the top, above the difficult terrain. He was like a trapeze artist, swinging from the branches. He carried all the tools he needed on his belt, leg holster, and harness as he flipped his little chain saw (which didn’t look big enough to cut the biggest tree but did) behind his back from hand to hand as needed to get the best angle of attack.
It was cold outside and I had trouble keeping the video camera still because I was shivering. I missed the shots of the biggest trees as they were in the act of falling because of that and a flashing red light on the viewfinder, which I was afraid was signaling either low battery or nearly full memory card. This is something Sena will be reminding me of for years to come.
I will never forget my dismay at missing the moment when the airborne arborist finished off the huge broken oak by kicking it, sending it to the ground with a biblical crash. I had to contain my urge to shout, “Hey, can we get another take on that?”
The big job is done—sort of. A wooded lot is a mixed blessing. Parts of the back yard are almost mesmerizing when the foliage is thick and the birds are flying all over the place. The forest is alive, but it doesn’t live forever. We have to learn how to live together somehow.
Here’s another post on music. This one got started while watching Eric Clapton Crossroads Guitar Festival 2019 last night on the Iowa Public Broadcasting Service channel. It’s great pizza and beer music. It was the fifth event of its kind since it got started in 2004. Part of the profits go to support the substance abuse treatment center in Antigua, founded by Clapton. Although inpatient treatment programs are currently suspended because of the COVID-19 pandemic, a virtual intensive outpatient treatment program is available.
I don’t mean to belittle Crossroads with the pizza and beer remark. I’m leading up to something and there is nothing wrong with enjoying music of any kind along with pizza and beer. Clapton and Peter Frampton did a superb job doing an old Beatles’ tune, “While My Guitar Gently Weeps.” Clapton did the original guitar solo on that one, which I didn’t know. Sheryl Crow and Bonnie Raitt rocked out Bob Dylan’s “Everything is Broken.” Many of the artists were older than me (I’m no spring chicken although they are definitely not retired). However, a newcomer, Lianne La Havas, delivered an outstanding cover of “I Say a Little Prayer for You,” originally sung by Dionne Warwick, later by Aretha Franklin.
It was great fun listening to these old songs. Most of them, except for “I Say a Little Prayer for You,” did tend to remind me of all the trouble going on in the world now, including the pandemic, political vitriol, and violence. Come to think of it, we could all use a little prayer right now.
I thought about posting the YouTube videos of a few of the Crossroads Festival songs. But I noticed that one of the YouTubers carried a large number of deleted videos, possibly due to copyright infringement issues, and they’re relatively recent. I figured the posted videos might not last long.
This brings me to an old (meaning much older than the 1960s) classical work I heard recently, “Vaughn Williams: Fantasia on a Theme by Thomas Tallis.” I saw it on the Light Classical cable music channel I wrote about a couple of days ago, the one about Samuel Coleridge-Taylor.
This one actually woke me up while I was sleeping on the couch. I frequently fall asleep to most classical music, partly because it helps me relax. However, the Vaughn Williams Fantasia didn’t just calm me—it also energized me. I’ve heard about the quality of music that can do that for people, but I was a bit skeptical. I have since looked for YouTube versions of the work, trying to find the same one I heard on the cable music channel.
I’m pretty sure I found it. It’s the one recorded by the Philharmonia Orchestra (London, UK) just last month, October 2020. I’ve listened to a couple of other highly praised recordings you can hear from a YouTuber called 2ndviolinist. One was by the Boyd Neel String Orchestra conducted by Boyd Neel in 1936. The other was done by the Halle Symphony Orchestra, conducted by Sir John Barbirolli in 1946. Both are widely thought of as masterpieces.
The Philharmonia Orchestra players are all spaced at least 6 feet apart, adhering to the social distancing required to reduce transmission of COVID-19. If I close my eyes (or even if I don’t), this doesn’t make me nervous as I listen to the oceanic sonority of the music itself. Many comments about the recording attest to the beauty of the piece, making it a soothing treasure in our troubled times.
I’m less worried about the possibility of the video ever being deleted. I felt the same way about the one by Samuel Coleridge-Taylor. It isn’t just because they’re old and copyright issues may be less of an issue. It’s more because they’re probably universally viewed as vital for healing our souls. At least I hope so.
Grab a pizza and a beer—and enjoy music that heals.
Last night I was half-dozing while listening to our cable light classical music channel. It was the usual lineup of 200-year-old white males of the 3-B variety—Bach, Beethoven, and Brahms. You see a photo or artist’s rendition of a guy in a powered wig, often looking depressed or constipated, alongside of short biographical blurbs. Many of the blurbs I mentally correct for grammatical or spelling errors.
Suddenly, I was struck by what I thought was a mistake in the name of the artist—next to a photo of a Black man. The name was Samuel Coleridge-Taylor. Even now I initially started to type Samuel Taylor Coleridge, which also didn’t make sense, because he was not a composer. He was a famous 19th century poet who wrote The Rime of the Ancient Mariner, Kubla Khan, and other works I learned from my English Literature professor, Dr. Jenny Lind Porter (that was her real name; no mix up with the Swedish opera singer, Jenny Lind).
I learned a lot from Dr. Porter, although I didn’t learn anything about Samuel Coleridge-Taylor, who was a famous 19th century composer in England. He happened to have been of mixed racial parentage, like I was. His mother (Alice Hare Martin) was white and his father was black—exactly my situation. His father (Dr. Daniel Peter Hughes Taylor) didn’t know about Samuel and they never met. I knew my father—and probably picked up some of his bad habits. Alice gave Samuel the name Coleridge because she was a fan of the poet. My name is Jim, but people often call me John, which was my father’s name.
How I got confused was a simple mental transposition of the last names. Samuel Taylor Coleridge was a white man who was hooked on laudanum and wrote great poetry. Samuel Coleridge-Taylor was a mulatto who was not hooked on laudanum and wrote great music.
I had never seen any composers of African American descent on the cable music Light Classical channel—and we’ve been cable subscribers for many years. I have to wonder whether I just have not been paying attention or whether this is a recent phenomenon and a sign of the times.
Samuel Coleridge-Taylor and his wife, Jessie Walmisley (a white woman), had two children. They named his son Hiawatha, after the native American in Henry Wadsworth Longfellow’s poem, The Song of Hiawatha. It turns out Hiawatha (also known as Ayenwathaaa or Aiionwatha) was a real guy, an important Native American leader. Longfellow’s poem is actually about the legend of Hiawatha, which is probably not connected in any plausible way to the real life of Ayenwathaaa or Aiionwatha. Some speculate that naming their son Hiawatha might have been related to Hiawatha never knowing who his father was, which Samuel might have identified with.
The Coleridge-Taylors also had a daughter, who they initially named Gwendolyn Avril. Gwendolyn then later changed her name (why not?) to Avril Coleridge-Taylor.
Both Avril and Hiawatha went on to have distinguished careers in music. Avril was a conductor-composer in her own right—which makes me wonder why I’ve not seen any women highlighted on the Light Classical cable music channel.
Samuel was an influential and respected musical, cultural, and political leader. Sadly, he died young, of pneumonia. He was 37 years old.
I hope this helps you feel a bit less confused about all the names in this story. If you’ve got it straight, please drop me a note explaining it—so I can finally get it sorted out.