A couple of days ago, Country Arborists cleaned up the debris left behind in our back yard from the derecho that smacked Iowa in August 2020. They are wild, flying tree warriors. That was a scary storm and if the straight-line winds had blown in a slightly different direction, our house would have been all but demolished.
Like a lot of other people in the state, we’ve been clearing tree limbs. But the massive oak was beyond any tool we owned.
The view from our window was a constant reminder of the derecho. The fallen oak was broken but not separated high up and we had to leave that kind of work for the professionals. Many of the tree removal pros have been extremely busy. Some are scheduling out to a couple of years from now. Country Arborists are just as busy, but made time for us anyway.
We had no idea what was involved in tree removal jobs of this magnitude. When they arrived last Friday, one of the first things they noticed about our back-yard trees was one which they identified as possibly a Native American Trail Marker Tree. This summer, Sena noticed this odd, old tree which was bent at right angles.
Native American Trail Marker Tree
Anyway, I filmed the work they did, which was spectacular. They rigged a rope system which allowed one of them to cut the trees at the top, above the difficult terrain. He was like a trapeze artist, swinging from the branches. He carried all the tools he needed on his belt, leg holster, and harness as he flipped his little chain saw (which didn’t look big enough to cut the biggest tree but did) behind his back from hand to hand as needed to get the best angle of attack.
It was cold outside and I had trouble keeping the video camera still because I was shivering. I missed the shots of the biggest trees as they were in the act of falling because of that and a flashing red light on the viewfinder, which I was afraid was signaling either low battery or nearly full memory card. This is something Sena will be reminding me of for years to come.
I will never forget my dismay at missing the moment when the airborne arborist finished off the huge broken oak by kicking it, sending it to the ground with a biblical crash. I had to contain my urge to shout, “Hey, can we get another take on that?”
The big job is done—sort of. A wooded lot is a mixed blessing. Parts of the back yard are almost mesmerizing when the foliage is thick and the birds are flying all over the place. The forest is alive, but it doesn’t live forever. We have to learn how to live together somehow.
I recently read an article about Maintenance of Psychiatry (MOC) written by Dr. Henry A. Nasrallah, MD and published this month in Current Psychiatry. The title is “Revamp the maintenance of certification program.” It brought back memories of my crusade to do the same thing in past years.
I lost my connection to that crusade when I was in my last year of my phased retirement contract. In a way, though I don’t miss MOC itself, I miss the sense of meaning and purpose I had while I opposed MOC through working with the Iowa Medical Society, through a petition to oppose Maintenance of Licensure (MOL, a state based version of MOC), and through writing articles and blogging about why I think psychiatrists and physicians in general don’t need these expensive, time-consuming activities which have led to anti-trust lawsuits being filed against certification boards.
In his article, Dr. Nasrallah criticizes the MOC as a monopoly perpetrated by the American Board of Psychiatry and Neurology (ABPN) and cites his own informal survey of 319 Current Psychiatry readers. He found that 86.5% of them recommended abolishing MOC. He tends to agree there should be an alternative to it. He recommends bringing back the oral exam.
I think it’s an interesting suggestion and I respect Dr. Nasrallah’s effort to not just oppose MOC, but to come up with another way for Psychiatry diplomates to keep their knowledge and skills up to date.
I remember my own oral board certification exam. It was very anxiety provoking, but I passed on the first try. There are reasons in addition to the anxiety they caused for why the oral boards were phased out after 2008. You can find them on the first page of a very entertaining post by Dr. Maria Yang. It’s a very long article, but the gist of the reasons for abolishing the oral boards is outlined on the first page. It was almost impossible to eliminate the wide variability of the live patient interview experience for diplomates while not being a guaranteed method for assessing a candidate’s knowledge and skills.
Dr. Yang lists several horror stories that make up the unverifiable yet terrifying lore about the process.
Even Dr. Nasrallah admits that the usual way the oral exams were conducted back in the day was almost unbelievably complicated logistically and also extremely expensive. He suggests that conducting them by videoconferencing could cut down on the costs, which is plausible. The justification for reinstating oral board exams is that it provided examiners a method for assessing a candidate’s interview skills and ability to collect and synthesize history and observation into a thorough diagnostic assessment and comprehensive treatment plan.
In fact, the academic medical center where I taught held what are sometimes called mock oral board exams regularly, which produced a tolerable mimic of the oral board experience in a less anxiety-provoking environment.
Making the oral exam, even in virtual format, the alternative to MOC would probably still make candidates nervous. It could also by logistically challenging as well. Would they be vulnerable to some sort of hack, such as Zoom bombing?
I spent a lot of time opposing MOC while I was working. It was frustrating. On the other hand, I thought it was important for me to let trainees know that life after residency would include challenges in addition to patient care and teaching, and that lifelong learning activities they engaged in might cost them a lot of money and personal time that they might find burdensome. I thought of myself as an example of a responsible protester in basic agreement with the principle of lifelong learning and improvement, although objecting to the certification boards’ methods.
The anti-MOC movement was a crusade that gave me a sense of purpose. I’m retired now. I salute Dr. Nasrallah.
I’m writing this post today because this firefighter retires tomorrow—and I’ll probably be very busy and too weary at the end of my last day on the psychiatry consult service to write. In fact, I’ve been too busy and tired to post for the last several weeks because we’ve been in the process of moving. Does that ever really end?
I can tell that what will really end at around 5:00 PM tomorrow is my career as a general hospital psychiatric consultant. It has been a long time coming. I’ve been on a 3-year phased retirement contract and going back and forth between wishing for it to end sooner and being scared to death as the final day approaches.
There are those last things: handing in the keys, the white coats, the parking hang tag and the like. I’ve cleaned out my office and somebody already wants it. I’m surprised that I’m just the tiniest bit territorial about the place, which is strange. I never spent much time in it because I was always chasing consults around the hospital.
I’ve never retired before. I wonder what the rules are. I still don’t know how to answer everybody’s question: “What are you going to do?”
There is the “new” house. It’s actually an older home, which fits my status as an older person, I guess.
The floors squeak and creak, a lot like my joints. There are little jobs and slightly bigger jobs to do for which I’m painfully aware of the need to develop a whole new skill set—or at least relearn them.
It’s about new noises and new animals. A fox trots across our yard occasionally. I’m used to deer, but we’ve never spotted a fox on our lawn. It has a rusty coat streaked with a lot of gray. It looks old. But it’s a good hunter and more than once we’ve seen it carrying a big mouthful of something that might have put up a pretty good fight.
I’m touched by the well-wishers, and those who say thanks for the memories. Just about every day of the last week, I’ve seen and done something at the hospital which makes me say, “That is what I’ll miss.”
I almost never write more than one post a day, but I’m pretty impressed with the blog post “The Perfect Balance” by The Goodenough Psychiatrist. It was very thought-provoking and the Stuart Ablon Ted Talk on Collaborative Problem Solving was refreshing.
A little over 3 ½ minutes into the video, Ablon says something interesting about conventional wisdom which helps cast doubt on blindly trusting it. When he remarks that conventional wisdom commonly fosters misconceptions including teaching that the earth was flat, it reminded me of a scene from Men in Black (I confess, one of my favorite movies). Agent K says, “A person is smart. People are dumb, panicky dangerous animals and you know it. Fifteen hundred years ago everybody knew the Earth was the center of the universe. Five hundred years ago, everybody knew the Earth was flat, and fifteen minutes ago, you knew that people were alone on this planet. Imagine what you’ll know tomorrow.”
His remarks highlight the challenge to those who break with conventional wisdom, which can sometimes be isolation.
Today was my first day back on the hospital consultation-liaison service and I’m a little tired. I put about 2 miles and 22 floors on my step counter, which was a nice pace for starters. It’ll get busier as the COVID-19 surge develops over the next couple of weeks.
Being in phased retirement means I’m away for weeks, sometimes more than that. The pandemic changed many processes and policies while I was gone.
I think the biggest challenge I had this morning was just getting used to donning and doffing the face shield. I passed many people in the halls who are wearing them. My clumsiness was a little embarrassing. It took me a while just to figure out how to adjust the head band. But those who recommend them are right–they keep you from touching your face, which the masks don’t do.
You may have seen my YouTube video and the post on how to trim beards so they don’t interfere with the seal of the N95 masks. I even shaved mine off. Come to find out, I’ll probably never have to wear one given the shortages of masks generally.
I’m learning a lot of things on the fly and that includes how to use electronic gadgets to facilitate remote interviewing in order to cut down on spread of the virus.
I saw a lot more people in the stairwells and elevators were much less crowded.
I began rereading the book Invisible Man by Ralph Ellison today, which is Leap Day. Given what little I know about Leap Day and Leap Year in general, there isn’t a connection.
I first read Invisible Man well over 40 years ago. It was a paperback and I took it with me to Huston-Tillotson College in Austin, Texas (now Huston-Tillotson University), one of the historically black colleges and universities (HBCUs) in the United States.
It was very hot in Austin in my freshman year and the students didn’t have air-conditioned dormitories in those days. It must have been over 90 degrees. The glue melted on most of my paperback books, including Invisible Man. I suppose that’s why I eventually threw the book away, because it was falling apart.
After all these years, I bought a hardcover edition. We have air-conditioning now. I was motivated to read it again after I read Invisible Hawkeyes: African Americans at the University of Iowa during the Long Civil Rights Era, edited by Lena M. Hill and Michael D. Hill. See my blog posts, Milestones, and The Iowa River Landing Sculpture Walk, for background.
When I was a young man, I identified with the protagonist in Invisible Man. The Prologue still strikes a chord.
On the other hand, I googled my name today and found a few links that made me feel less invisible. Probably the most surprising link was to an interview with me entitled “James Amos, MD,” which you can read here. The piece evoked memories of a past version of me—which has not changed much since then. It mentions my former blog The Practical Psychosomaticist which I later renamed The Practical C-L Psychiatrist (C-L stands for Consultation-Liaison) after the flagship organization, the Academy of Psychosomatic Medicine changed its name to the Academy of C-L Psychiatry in response to a poll of its membership asking whether the name should be changed.
This biography makes me more visible, at least on the web. On the other hand, the blog no longer exists, due in part from my concerns about the General Data Protection Regulation (GDPR), which was enforced in 2018. I posted a lot of educational material about C-L Psychiatry on the blog along with pictures and presentations of my trainees. In a way, I did not protect their privacy and I was uncomfortable about that.
Other web pages surfaced during my self-googling. They included my article on delirium, “Psychiatrists Can Help Prevent Delirium,” posted on Psychiatric Times in 2011.
I also found my blog post on physician burnout, “How I left the walking dead for the walking dead meditation,” published on the Gold Foundation web site in 2014.
And there was my other Gold Foundation post about rude doctors, “Are doctors rude? An insider’s view,” posted in 2013.
There are a couple of petitions left over from years ago as well, about the controversial Maintenance of Certification (MOC) and the closure of state mental hospitals in Iowa several years ago.
I also found my review of Dr. Jenny Lind Porter’s book, The Lantern of Diogenes and Other Poems (published 1954).
The book seller’s note to me when Porter’s book was delivered in 2011 read as follows:
“Thanks for your purchase! It’s rare to find a book of this age that when you open the pages, it creaks like it is unread. I guess someone liked the way it looked on their bookshelf! Haha! Enjoy the book and Happy New Year, Rob J.”
An unread author is an invisible author. The first poem in the book is below:
The Lantern of Diogenes
by Jenny Lind Porter
All maturation has a root in quest.
How long thy wick has burned, Diogenes!
I see thy lantern bobbing in unrest
When others sit with babes upon their knees
Unconscious of the twilight or the storm,
Along the streets of Athens, glimmering strange,
Thine eyes upon the one thing keeps thee warm
In all this world of tempest and of change.
Along the pavestones of Florentian town
I see the shadows cower at thy flare,
In Rome and Paris; in an Oxford gown,
Men’s laughter could not shake the anxious care
Which had preserved thy lantern. May it be
That something of thy spirit burns in me!
Dr. Porter’s house in Austin, Texas was demolished a few years ago. There were plans to build a house there reminiscent of the architectural style of her original home and also a remembrance of her published work. I just noticed a satellite image of the property. There is no visible evidence that anything of that nature was ever built. Dr. Porter is, in a sense, invisible although her lantern still burns.
Visibility is a relative term. My advancing age and approaching retirement sometimes lead me to feel like I’m becoming invisible, gradually vanishing from the landscape of consultation-liaison psychiatry and general medicine.
Ralph Ellison’s book Invisible Man is a visible legacy. My legacy is small—yet the flame flickers, visible after all.
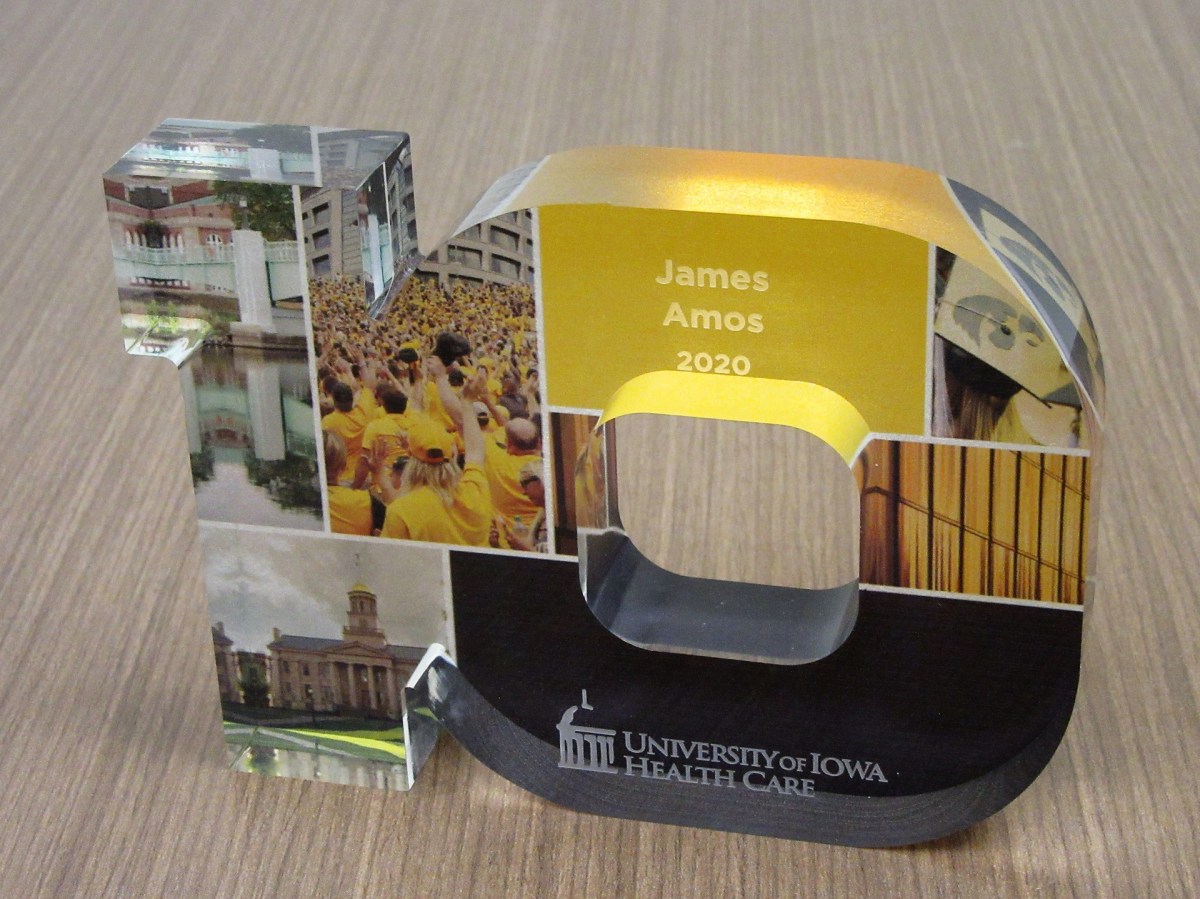
I got a nice, if puzzling surprise today. At a faculty meeting I was recognized for my 10-year anniversary of service at our hospital. It’s an important milestone, even if it is wrong. They scheduled this small event a couple of months ago, but I was too busy on the psychiatry consult service to break away. I also usually carry the pager for the trainees during the noon hour when the faculty meetings are held.
The 10-year anniversary recognition was very kind—except that I’ve been here for twenty odd years, not counting residency and medical school.
In all fairness, my department knows that and we shared a few jokes about it. I guess I should clarify that I have left the university for private practice a couple of times, which interrupts the years of service recognition timelines.
I was gone both times for a total of less than 12 months—just sayin’. I returned for a few reasons, although mainly because I missed teaching.
Anyway, I showed up at the faculty meeting, albeit a little guilty looking because I’m usually too busy to attend. My department chair arrived and said that she had to run back to get my “statue.”
That jarred me. Several years ago, when I had my first blog, The Practical Consultation-Liaison (C-L) Psychiatrist, I used to kid my readers that someday a statue of me would be erected in the university Quad. It would be made of Play-Doh.
And that’s why I asked her as she turned to leave, “Is it made of Play-Doh?” She looked puzzled and I didn’t really think I could explain in a way that wouldn’t make me look like I’d been smoking something illegal.
The “statue” is a handsome little sculpture of the number 10, standing for 10 years of service. It has color photos embedded in it of various aspects of academic life at the University of Iowa, many of which I’ve had the privilege of enjoying in the 30 odd years my wife, Sena, and I have been in Iowa City.
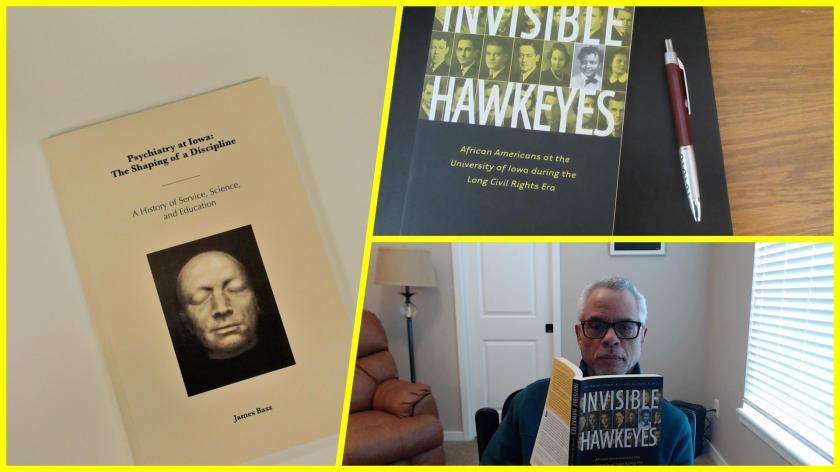
Just before the meeting, I had walked up to the 8th floor (I always take the stairs) to the psychiatry department offices to see if I could get a copy of the recently published history of the department, Psychiatry at Iowa: The Shaping of a Discipline: A History of Service, Science, and Education, written by James Bass.
Mr. Bass interviewed many people in the department, including me. I didn’t expect that my perspective on the consultation service, the clinical track, or my race would even get mentioned. However, 2 out of 3 made it into print.
It didn’t really surprise me that my being African American was not mentioned. I think I’m probably the only African American faculty member of the department in its 100-year history, at least until very recently.
It reminded me of another book that I just acquired, Invisible Hawkeyes: African Americans at the University of Iowa during the Long Civil Rights Era, edited by Lena M. Hill and Michael D. Hill.
In a small way, I’m making the invisible visible.
Making the invisible visible
And also, because it’s great for my ego, I’m going to quote what Bass wrote about me in Chapter 5, The New Path of George Winokur, 1971-1990:
“If in Iowa’s Department of Psychiatry there is an essential example of the consultation-liaison psychiatrist, it would be Dr. James Amos. A true in-the-trenches clinician and teacher, Amos’s potential was first spotted by George Winokur and then cultivated by Winokur’s successor, Bob Robinson. Robinson initially sought a research gene in Amos, but, as Amos would be the first to state, clinical work—not research—would be Amos’s true calling. With Russell Noyes, before Noyes’ retirement in 2002, Amos ran the UIHC psychiatry consultation service and then continued on, heroically serving an 811-bed hospital. In 2010 he would edit a book with Robinson entitled Psychosomatic Medicine: An Introduction to Consultation-Liaison Psychiatry.” (Bass, J. (2019). Psychiatry at Iowa: A History of Service, Science, and Education. Iowa City, Iowa, The University of Iowa Department of Psychiatry).
In chapter 6 (Robert G. Robinson and the Widening of Basic Science, 1990-2011), he mentions my name in the context of being one of the first clinical track faculty in the department. In some ways, breaking ground as a clinical track faculty was probably harder than being the only African American faculty member in the department.
As retirement approaches this coming June, I look back at what others and I worked together to accomplish within consultation-liaison psychiatry. The challenges were best described by a former President of the Academy of Consultation-Liaison Psychiatry, Thomas Hackett (this quote I helped find for James Bass and anyone can view it on the Internet Archive):
“A distinction must be made between a consultation service and a consultation liaison service. A consultation service is a rescue squad. It responds to requests from other services for help with the diagnosis, treatment, or disposition of perplexing patients. At worst, consultation work is nothing more than a brief foray into the territory of another service, usually ending with a note written in the chart outlining a plan of action. The actual intervention is left to the consultee. Like a volunteer firefighter, a consultant puts out the blaze and then returns home. Like a volunteer fire brigade, a consultation service seldom has the time or manpower to set up fire prevention programs or to educate the citizenry about fireproofing. A consultation service is the most common type of psychiatric-medical interface found in departments of psychiatry around the United States today.
A liaison service requires manpower, money, and motivation. Sufficient personnel are necessary to allow the psychiatric consultant time to perform services other than simply interviewing troublesome patients in the area assigned. He must be able to attend rounds, discuss patients individually with house officers, and hold teaching sessions for nurses. Liaison work is further distinguished from consultation activity in that patients are seen at the discretion of the psychiatric consultant as well as the referring physician. Because the consultant attends social service rounds with the house officers, he is able to spot potential psychiatric problems.”— Hackett, T. P., MD (1978). Beginnings: liaison psychiatry in a general hospital. Massachusetts General Hospital: Handbook of general hospital psychiatry. T. P. Hackett, MD and N. H. Cassem, MD. St. Louis, Missouri, The C.V. Mosby Company: 1-14.
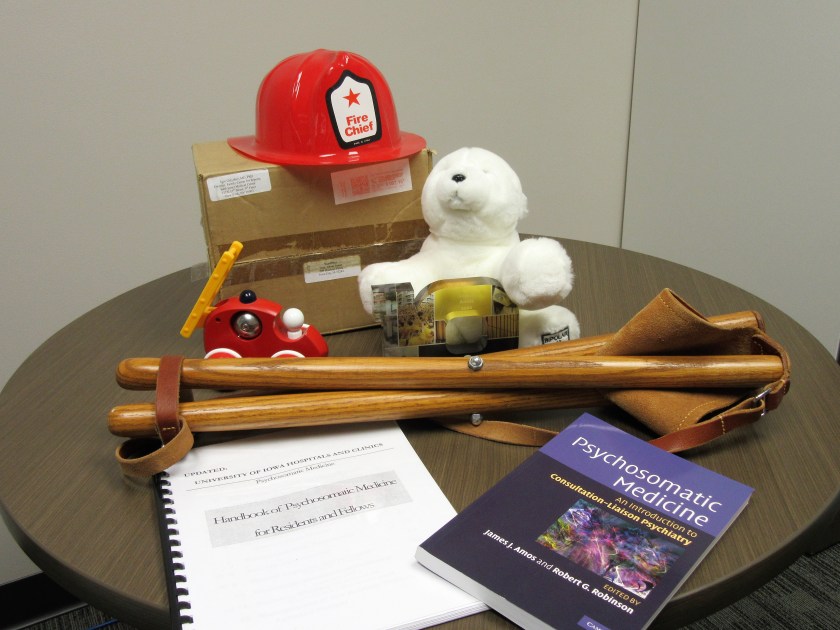
I have what seems like precious few mementos of my sojourn here in the department and, indeed, on this earth. I have a toy fireman’s helmet I found hanging in a plastic sack on my office doorknob one day. It was a gift from a Family Medicine resident who rotated on the consult service and who learned why I called it a fire brigade.
For the same reason, I have a toy fire truck, sent to me by a New York psychoanalyst who was also a blogger.
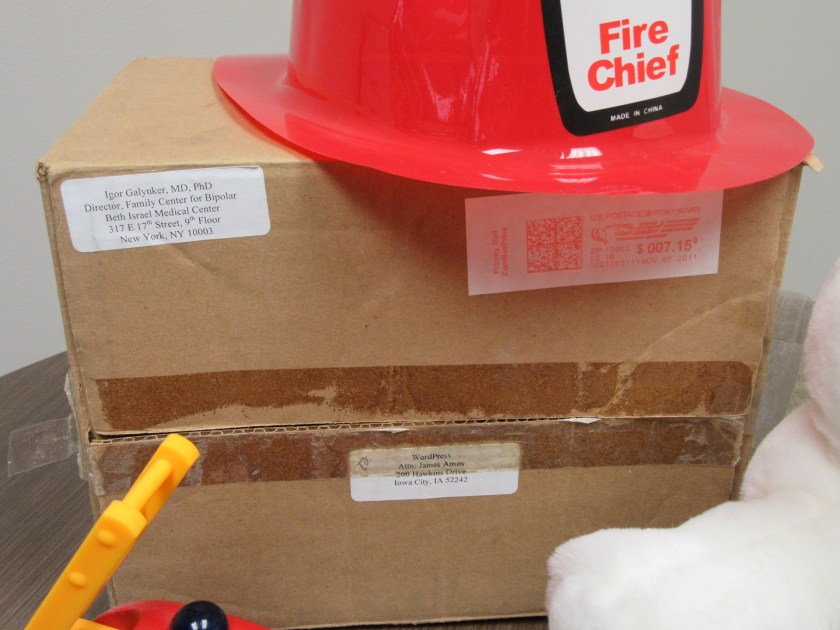
I have Bumpy the Bipolar Bear, believe or not, sent to me by psychiatrist, Dr. Igor Galynker, about whose emergency room suicide risk assessment method I had blogged about several years ago. C-L psychiatrists do a lot of suicide risk assessments in the hospital and the clinics. I still have the box with the address to me:
WordPress
Attn: James Amos
200 Hawkins Drive
Iowa City, IA 52242
I have my first homemade handbook for C-L Psychiatry and the published handbook that eventually replaced it. Thank goodness the leaders of the Academy of Consultation-Liaison Psychiatry listened to the membership and changed the name from Psychosomatic Medicine to C-L Psychiatry.
I have an award for being an excellent clinical coach.
And I have my little camp stool, which a colleague who is a surgeon and emergency medicine physician gave me and which allows me to sit with my patients anywhere in the hospital, so that I don’t have to stand over them.
It will all fit in a cardboard box on my last day—the next milestone.
I had so much fun with the giant chicken post on January 25, 2020 that I thought it would be nice to revisit the subject, only this time take a butt-freezing tour of the entire Iowa River Landing (IRL) Sculpture Walk.
We took the walk Tuesday, January 28, 2020. The weather was typical for Iowa in January. The temperature was in the teens and there were brief flurries. My wife, Sena, and I dressed warm and took a meandering journey through the Sculpture Walk, guided by a small map.
It was a little more challenging because snow and ice covered up many of the plaques identifying the works (and parts of the sculptures as well) although this lent even more visual interest to them. They’re three dimensional objects anyway and you really have to walk around them to fully appreciate their complexity. You have to watch out for yellow snow.
What made this adventure even more special was the Iowa Writers’ Library in the lobby of the Coralville Marriott Hotel and Conference Center. It’s maintained by the Coralville Public Library. One of the issues I had was being unfamiliar with the text of the poems and other literary works (all were connected with the Iowa Writers’ Workshop) referenced by the artists. The library was cozy, had a fireplace warming the softly lit room lined by bookshelves and a couple of ladders on wheels to help you reach the books higher up.
I have always felt comforted in libraries, ever since I was a little boy. Every day I got the chance, I would walk to my hometown library (which was about a mile trip), browse the stacks for hours, then tote home piles of books in both arms.
The hotel library had most of the books pertinent to the literary references cited by the artists for their sculptures. I even found David B. Axelrod’s book, The Man Who Fell in Love with a Chicken. It turns out that the title of Axelrod’s poem is “The Man Who Fell in Love with His Chicken.” There, I’ve said enough already about that chicken.
Of course, I couldn’t take the time to find and read every book; we would not have had time to freeze our butts off touring the sculptures.
I didn’t wear my heavy winter boots and had to crunch through the crusty snow nearly up to my ankles to reach certain sculptures. Sena was dressed better for the weather but we both slipped around on the ice and I began to think more and more about things like broken hips.
But we soldiered on because it was necessary to walk completely around the Made of Money sculpture by Aaron Wilson in order to see the message printed, “HOW CAN WE HELP YOU?” It’s funny because that’s what I typically ask patients in the general hospital when I sit down on my little camp stool after I introduce myself to them as a consultation-liaison psychiatrist.
The sculpture To Dorothy, by artist James Anthony Bearden, was in a difficult spot and initially we thought we’d have to either rappel down from the roof of the building it was in front of or climb up the big retaining walls to get a good look at it. We found a way out to it and ignored passersby who gawked at us. They needed to admire us for how unique we are (not how eccentric and possibly a danger to ourselves and others), which is what I think Iowa Poet Laureate Marvin Bell was getting at in his poem of the same title as Bearden’s sculpture.
The sculpture, A Thousand Acres, by artist V. Skip Willits was another piece you really have to walk around to fully appreciate, although you generally have to do that with any sculpture. The book of the same title by Jane Smiley is based on Shakespeare’s King Lear—which I have also never read—but which I got an earful about in my undergraduate days from a fellow student who thought he knew everything there was to know about King Lear. He was garrulous in the extreme and bested me in debating class mainly because he never let me open my mouth.
The sculpture by artist Victoria Ann Reed, called Convergence, was very intriguing and looked more like a human figure who had been through a wormhole than a memory.
The Tipping Point, by artist Sarah Deppe, was a convincing image of persons with holes in their heads (several holes in fact). Bureaucrats come to mind.
We nearly dismissed the sculpture called After Trillium by artist Anthony Castronovo as a broken lamppost with dysfunctional solar panels, only partly because snow and ice covered the panel describing it. On the other hand, the top part does resemble a flower called a Trillium, not to be confused with Trillian, a character in the book by Douglas Adams, The Ultimate Hitchhiker’s Guide to the Galaxy. I’m glad I could clear that up for you.
The Prairie Breeze Bench by artist Bounnak Thammavong is a sculpture you could actually sit on and watch the Bald Eagles. However, it’s made of steel and the seat was covered by snow. After you wipe away the Bald Eagle droppings, you can read the poem by James Hearst, “Landscape Iowa.” You can also hear it set to music and performed by Scott Cawelti, a former University of Northern Iowa educator who taught film, writing, and literature courses. He also edited The Complete Poetry of James Hearst (University of Iowa Press, 2001).
The Alidade sculpture by Dan Perry was the one Sena and I both really liked. I know Perry says the alidade was used by astronomers but I remember it as being a part of an instrument used by land surveyors, also for measuring distance and angles in topographical surveys. I used to work for consulting engineers as a surveyor’s assistance and draftsman many years ago. Perry links it to the poem entitled “1,2,3” from James Galvin’s book of poems, X: Poems. I confess I don’t see the connection yet. The poem for the most part reminds me of spelunking although Galvin describes a hole that he and a friend rappel into as being a planet. Much of the rest seems to be about something very painful. I’m sorry I can’t do better, but that’s why he’s a poet and I’m not.
Next, we encountered Bounnak Thammavong’s second sculpture, a very recognizable fish, a “lowly river carp,” entitled From the River. It’s linked to the poem “Where Water Comes Together with Other Water” by Raymond Carver. When I was a boy, I used to fish for bullhead in my hometown river. I sometimes caught carp and thought that was the poorer catch. It didn’t matter. I always threw both back into the river. My mom would not clean fish and neither would I.
Finally, by a pretty circuitous route, we saw the last sculpture, Gilead, by artist Kristin Garnant. The snow plow had piled up a lot of snow around it. I probably won’t read Gilead, the epistolary novel by Marilynne Robinson.
In fact, I probably won’t read a lot of the literature connected with the sculptures we saw. I did read Margaret Walker’s poem “For My people.” Sorry, Jubilee is way too much for me. She was the first African-American woman to be accepted into the Iowa Writers’ Workshop, of course depending on which story you believe about when the program formally began (Invisible Hawkeyes: African Americans at the University of Iowa during the Long Civil Rights Era, in Chapter Four: Obscured Traditions: Blacks at the Iowa Writers’ Workshop, 1940-1965, by Michael D. Hill, University of Iowa Press, 2016).
In some ways, I identify way with her, one of the reasons being obvious and skin-deep. The other is that she taught school at Jackson State, a historically black college in Jackson, Mississippi.
I wonder if the IRL Sculpture Walk could include another one for her, just to make it an even dozen?
I spent my Freshman and Sophomore college years at a historically black college. It was then called Huston-Tillotson College (now Huston-Tillotson University) in Austin, Texas. That was back in the mid-1970s. I had grown up in largely white neighborhoods and gone to predominantly white schools prior to going to H-TC. It was a culture shock and that’s probably about all I’ll say about it for now, since this post is way too long.
I can say one other thing about H-TC. I submitted a poem for the college’s annual poetry contest. Winners would have their work published in the school’s small anthology called Habari Gani (Swahili for What’s Going On?). Mine didn’t make it but years later I scoured the web looking for a way to get a copy of Habari Gani, finally succeeding only a few years ago after tracking a copy of the Spring 1975 volume down at the H-TU library. I like the short introductory poem:
I took the picture of the little chair one of the residents brought to the psychiatry consult office yesterday. I got a big charge out of it, especially because I’ve been using a version made of wood and leather for a few years now. I think it’s possible that it could be an auspicious chair.
The resident actually used his, too. It was a busy day; I put in about 4 miles and 40 floors on my step counter—which meant the residents did too. The chair is obviously useful to rest our feet, but I think Thomas P. Hackett summed up the best ever rationale for sitting with patients:
“As a matter of courtesy, I sit down when interviewing or visiting patients. Long accustomed to the ritual of making rounds, many physicians remain standing as a matter of course. Standing, physicians remind me of missiles about to be launched, poised to depart. Even if that is not necessarily true, they look the part. Patients sense this and it limits conversation. In addition, when standing, the physician necessarily looks down on the patient. This disparity in height is apt to encourage the attribution of arrogance. Looking down at a patient who is prone emphasizes the dependency of the position. Sitting at the bedside equalizes station. Sitting with a patient need not take longer than standing with him.”— Hackett, T. P., MD (1978). Beginnings: liaison psychiatry in a general hospital. Massachusetts General Hospital: Handbook of general hospital psychiatry. T. P. Hackett, MD and N. H. Cassem, MD. St. Louis, Missouri, The C.V. Mosby Company: 1-14.
I had a little fun with the chair in a YouTube video as well.
The chair I use now is a replacement for the first one I got as a sort of loaner from a colleague in Palliative Care Medicine. That one broke during a consultation visit with a patient and his family (circumstances disguised to protect confidentiality) in the emergency room in which we were asked to evaluate for catatonia. The patient was mute but there was little evidence otherwise for catatonia, one of the chief features of which is the inability to react to any stimulus in the environment. I was sitting on the chair explaining in detail the intravenous lorazepam challenge test for catatonia (which often interrupts the episode of muteness and immobility).
I was sitting in front of the patient but facing the family and the consult service trainees while expatiating on the topic. As I was droning on, I heard a sudden pop—and I fell unceremoniously on my rear end as the chair collapsed beneath me.
My audience exploded in loud laughter, of course, as you’d expect when a pompous ass falls on his ass. But they also pointed to the patient. When I turned to look at him, he was convulsed with apparent mirth although still unable to make a sound.
I considered this a novel test for catatonia, negative in this case. Of course, it would be impractical for regular use.
Where was I? Oh, the little chair the resident brought for consult rounds. I was honored by it. It seemed to show that I was leaving a legacy as I head for retirement in June.
Another sign of leaving a legacy was a New Year’s email message I got from a former resident, Dr. Paul Thisayakorn, MD, who has been making an auspicious beginning in the field of consultation-liaison psychiatry in Thailand. He’s working very hard and is an outstanding clinician, researcher, and teacher. He has a lovely family. He and I respect each other a great deal.
Speaking of auspicious, when Paul graduated from our psychiatry residency and before leaving for his Consultation-Liaison fellowship program, he gave me a necktie with white elephants printed on it. I still have it. I may not have the symbolic meaning of the white elephant exactly right, but I think the white elephant in Thai culture is called “chang samkhan,” or maybe “chang phueak” which means “auspicious elephant.” In general, I think the idea is they symbolize success or at least the promise of success. Paul’s gift showed his gratitude and respect for me because I was one of his teachers. I am still honored to have been a part of his education and his life. I will always treasure his gift of gratitude.
An auspicious tie
Paul is very hard-working and very successful. And if the residents now start to use the little camp stools to sit with their patients, I would treasure that legacy as well.
I got an email from Don R. Lipsitt, MD yesterday which reminded me of the Janus Head logo for the Academy of Consultation-Liaison Psychiatry (ACLP). It was changed to another sort of nondescript logo several years ago for reasons I didn’t understand.
Dr. Lipsitt is a luminary in C-L Psychiatry and recently published a definitive history of the field, Foundations of C-L Psychiatry: The Bumpy Road to Specialization (2016).
Go ahead; buy this book!
I posted a blog or two about Don and his book in a previous blog, The Practical C-L Psychiatrist. We’ve never formally met. A few years ago, he noticed that I had written about him and his book. I had sent him an email message about it at around the same time the APM was considering the name change for the organization, telling him that I had plugged his book and asking him what he thought of the name change. Incidentally, he thought both of our books made a great package, so I guess I’m allowed to plug mine, strangely titled Psychosomatic Medicine: An Introduction to C-L Psychiatry, editors James Amos and Robert Robinson (2010).
Go ahead; buy my book, too…
Don expressed his
opinion about the name change:
“I feel I have dealt with that at some length in my book. I
still feel C-L is most fitting and that the Board made a big mistake naming it
PM. Who were they? Any C-L psychiatrists among them? Any Psychosomaticists? Why
are not the “complex medically ill” a special population? And why is
APA now offering courses on “integrated” care (which is what C-L
psychiatry has always been about? The notion that C-L was not
declared a specialty because it was considered a skill of ALL psychiatrists
(with minimal training), then how do geriatric or child psychiatry become specialties
(that all psychiatrists also have training in)? Don’t get me started.”
He considered his book, in large part, a “polemic” against
the name “Psychosomatic Medicine.”
Anyway, the ACLP was formerly the Academy of Psychosomatic
Medicine (APM) until a couple of years ago when the organization responded
robustly to the membership (of which I was one at the time) to abandon the term
“Psychosomatic Medicine” and adopt what rank and file practitioners
preferred—Consultation-Liaison Psychiatry.
It was a kind of rebranding and it was not the first time
the academy had considered a name change. I and a lot of other C-L
Psychiatrists cringed at the term “psychosomatic,” not so much because of the
word itself in terms of its true denotation, but because of the unfortunate
negative connotations it had acquired.
Another luminary of C-L Psychiatry, Dr. Thomas Hackett, MD,
wrote about the term “psychosomatic” in the Massachusetts General Hospital:
Handbook of general hospital psychiatry: edited by Hackett and Ned Cassem
(1978):
“The term ‘psychosomatic service’ has had a variable
history. The term generally leaves a bad taste in the mouths of physicians. It
reminds them of the 1930s, 1940s, and 1950s, when various psychosomatic schools
espoused doctrines linking specific psychological conflicts or unique
personality profiles with diseases designated as psychosomatic. Compounding
this misunderstanding has been the term’s abuse by the general public, who
regard anything psychosomatic as either imaginary or nervous in origin. As a
consequence, most people believe that a psychosomatic disease is not to be
taken seriously.”
Well, anyway, because of my anecdotage, I’ve strayed a
little from my original story about the Janus head logo.
I already mentioned that the logo was abandoned in favor of something that looks like waves and could lead to seasickness. I inquired about the history of the use of the Janus head logo.
In addition to my curiosity about why the logo was changed, I also wondered why it was chosen in the first place and when. According to Don, it was part of the organization’s journal, Psychosomatics, in the late ‘60s and ‘70s. What was interesting is that it was already in use by the Journal of Geriatric Psychiatry when the Psychosomatics editors started using it. However, a conflicting view was that it was not introduced to the cover until 2010. Hmmmm.
I saw the 2012 issue of the APM Newsletter had a pretty funny picture of Drs. Shuster and Rosenstein posing as Janus and the statement “Thank you, Janus. You served us well for over 50 years.” That might put the origin of the logo, at least, around 1962 although my understanding is that APM was started in 1953 (TN Wise, A Tale of Two Societies, Psychosomatics 1995).
Time to say “Hello, again, Janus?”
It’s
just my opinion, but because Janus is the ancient god of beginnings and
transitions, gates, doorways, endings and time, and typically depicted as
two-faced because he looks to the future and the past, I think the symbol is a
better image for what C-L Psychiatry has been through over the years.
Anyone for re-rebranding and go retro back to the Janus head logo?