I’m writing this post today because this firefighter retires tomorrow—and I’ll probably be very busy and too weary at the end of my last day on the psychiatry consult service to write. In fact, I’ve been too busy and tired to post for the last several weeks because we’ve been in the process of moving. Does that ever really end?
I can tell that what will really end at around 5:00 PM tomorrow is my career as a general hospital psychiatric consultant. It has been a long time coming. I’ve been on a 3-year phased retirement contract and going back and forth between wishing for it to end sooner and being scared to death as the final day approaches.
There are those last things: handing in the keys, the white coats, the parking hang tag and the like. I’ve cleaned out my office and somebody already wants it. I’m surprised that I’m just the tiniest bit territorial about the place, which is strange. I never spent much time in it because I was always chasing consults around the hospital.
I’ve never retired before. I wonder what the rules are. I still don’t know how to answer everybody’s question: “What are you going to do?”
There is the “new” house. It’s actually an older home, which fits my status as an older person, I guess.
The floors squeak and creak, a lot like my joints. There are little jobs and slightly bigger jobs to do for which I’m painfully aware of the need to develop a whole new skill set—or at least relearn them.
It’s about new noises and new animals. A fox trots across our yard occasionally. I’m used to deer, but we’ve never spotted a fox on our lawn. It has a rusty coat streaked with a lot of gray. It looks old. But it’s a good hunter and more than once we’ve seen it carrying a big mouthful of something that might have put up a pretty good fight.
I’m touched by the well-wishers, and those who say thanks for the memories. Just about every day of the last week, I’ve seen and done something at the hospital which makes me say, “That is what I’ll miss.”
I brought my camp stool home from my office at the hospital yesterday. For the past several years and up until the time of the COVID-19 pandemic, I used it while interviewing hospitalized patients as part of my job as a consultation-liaison psychiatrist in the general hospital. I stopped only when I wondered whether carrying around an object which could be contaminated with the virus was a safe thing to do.
A colleague lent me the little chair when he and his colleagues on the Palliative Care Medicine consultation service started using them. I asked him whether he wanted it back and he graciously said I could take it with me now that I’m retiring—and use it as a camp stool (in a way, saying “Please take your seat”). For many years prior to getting the stool, I had been finding a chair or sending my trainees to find one for me. I felt more comfortable sitting eye to eye with patients and I got the impression that my patients appreciated that as well.
I got a lot of positive feedback from patients, family members, and other hospital staff about the little chair. I think it helped break the ice with patients and was a great opener, especially if they felt well enough to express a sense of humor— “Hey, doc; you don’t need nunchucks; I promise I’ll be good!”
There are a few papers in the medical literature supporting the usefulness of sitting with patients. Most authors assert that it helps build rapport and increases the patients’ perception of how interested their physicians or other health care clinicians are in their welfare (see the reference list below).
Once, when my original little chair broke beneath me during an evaluation for catatonia in one patient, the stool abruptly became a novel catatonia assessment tool.
The patient was mute but there was little evidence otherwise for catatonia, one of the chief features of which is the inability to react to any stimulus in the environment. I was seated on the chair explaining in detail the intravenous lorazepam challenge test for catatonia (which often interrupts the episode of muteness and immobility).
I was sitting in front of the patient but facing the family and the consult service trainees while expatiating on the topic. As I was droning on, I heard a sudden pop—and I fell flat on my fundament as the chair collapsed beneath me.
My audience exploded in loud laughter, and pointed at the patient. When I turned to look at him, he was convulsed with silent mirth.
I considered this a negative test for catatonia in this case, though impractical for regular use.
My colleague gave me a replacement camp stool, more securely built. However, he mentioned he might give up using his as a result of my accident which, incidentally, befell (rimshot) another doctor on his team. I’m not sure whether I’ll use the little chair. If I sit on it too long, my legs go numb. I think that’s about 10-15 minutes, about the length of time mentioned in one of the studies below. It didn’t seem to influence the positive perception of the visit—but it did make me walk funny.
I probably spend about the same time with patients now that I don’t use the little chair. But I don’t feel right about it. I’m always reminded of what Hackett said:
“As a matter of courtesy, I sit down when interviewing or visiting patients. Long accustomed to the ritual of making rounds, many physicians remain standing as a matter of course. Standing, physicians remind me of missiles about to be launched, poised to depart. Even if that is not necessarily true, they look the part. Patients sense this and it limits conversation. In addition, when standing, the physician necessarily looks down on the patient. This disparity in height is apt to encourage the attribution of arrogance. Looking down at a patient who is prone emphasizes the dependency of the position. Sitting at the bedside equalizes station. Sitting with a patient need not take longer than standing with him.”—Thomas Hackett, in MGH handbook of general hospital psychiatry, 1978.
References:
Johnson RL, Sadosty AT, Weaver AL, Goyal DG. To sit or not to sit?. Ann Emerg Med. 2008;51(2):188‐193.e1932. doi:10.1016/j.annemergmed.2007.04.024
Swayden KJ, Anderson KK, Connelly LM, Moran JS, McMahon JK, Arnold PM. Effect of sitting vs. standing on perception of provider time at bedside: a pilot study. Patient Educ Couns. 2012;86(2):166‐171. doi:10.1016/j.pec.2011.05.024
Strasser F, Palmer JL, Willey J, et al. Impact of physician sitting versus standing during inpatient oncology consultations: patients’ preference and perception of compassion and duration. A randomized controlled trial. J Pain Symptom Manage. 2005;29(5):489‐497. doi:10.1016/j.jpainsymman.2004.08.011
Orloski CJ, Tabakin ER, Shofer FS, Myers JS, Mills AM. Grab a Seat! Nudging Providers to Sit Improves the Patient Experience in the Emergency Department. J Patient Exp. 2019;6(2):110‐116. doi:10.1177/2374373518778862
Merel SE, McKinney CM, Ufkes P, Kwan AC, White AA. Sitting at patients’ bedsides may improve patients’ perceptions of physician communication skills. J Hosp Med. 2016;11(12):865‐868. doi:10.1002/jhm.2634
The robins are building their Hurrah’s nests in our back yard again. That’s about the only thing that has not changed. The COVID-19 (C-19) pandemic has changed just about everything else in our lives.
I wear a face shield now at the hospital. We’re told to wear it as much as possible, like putting on our clothes in the morning. Don’t we leave them on all day? The shield keeps you from touching your face, which is why it’s better than a face mask. However, I’ve noticed something about wearing the face shield for much of the day. Before I describe it, let me give you analogy: If you’ve ever worked detasseling corn when you were young a long time ago, you might remember what happened when you closed your eyes at night and tried to go to sleep. I saw corn fields—miles and miles of corn fields. When I opened my eyes, the vision would disappear. But as soon as I closed my eyes again, I saw the vast corn fields.
It’s crazy, but I have a similar sensory after-effect when I doff my face shield–sometimes I still feel the headband. The pressure of it is just the same as if I were still wearing it. I suppose it’s because I cinch it too tightly. But if I don’t, it slips down my brow, pushing my eyeglasses down my nose.
Another change—I’m a Consultation-Liaison (C-L) Psychiatrist, so I’m used to washing my hands in between patients in the hospital. Now, I’ve got something I’ve never had before–alligator hide patterns on the backs of my hands. They’re dry and cracked. I don’t count the number of times I wash my hands, but it’s a lot more frequent than I used to do. It’s not uncommon for health care professionals to wash hands 75-100 times a day in the C-19 era. I have to use hand cream conscientiously—something I almost never did.
I’m less comfortable being closer than several feet away from people. I tend to hug the walls and corners in stairwells, where I now encounter more people than I ever have before. I guess the message everyone hears is “Stand by me—six feet away if you please.”
I don’t shake hands anymore. The lines into the hospital sometimes lead to crowding while we wait to have our temperatures taken and answer the screening questions about whether we’ve had fever, cough, shortness of breath, etc. It’s perfunctory most of the time, because virtually always the answer is “no” and everybody is in a hurry.
I don’t carry my little camp stool with me anymore, which allowed me to sit down with patients and have face to face, eye level interaction. I’m distinctly uncomfortable standing over them because I haven’t done that in years. If there is a chair in the room, I’m hesitant to use it because, like the camp stool, I worry that it might carry C-19 virus on its surface.
I used to evaluate psychiatric patients in our emergency room by simply going there and seeing them face to face, either in their rooms or, when it was really busy (which is most of the time), in the hallways.
I just used a remote telehealth interface platform using an iPad the other day, which allows me to interview patients from my office, in order to avoid the risk of contagion. It was a little slow and awkward, and I was uncomfortable that a health care professional had to be in the emergency room to hold it up for the patient—who was covered in blood. I felt a little guilty.
I used to round with medical students and residents on our patients. We were the movable feast, a sort of MASH (Mobile Army Surgical Hospital) unit, more like Mobile Unifying Shrink Hospital (MUSH). Unifying means unifying medicine and psychiatry. The medical students are not permitted on the wards now, in order to protect them. It’s awkward rounding with only one resident at a time, although another resident can do other things like chart review and telephone relatives for collateral history. I get in the hospital earlier nowadays, and see many non-C-19 patients alone without trainees, preparing for the C-19 surge when I expect we’ll get many more consultation requests to help care for C-19 patients with delirium and depression. It’s a one-man hit-and-run psychiatry consult service and efficiency is mandatory to meet the demand.
I see patients by myself for another reason. Try as we might, C-19 positive patients will slip through the screens. Many are asymptomatic but contagious, and any test will have false negative results. The idea is to expose the least number of health care front line staff members as possible. Faculty capacity is stretched pretty thin, which is pretty much the situation everywhere. I have to choose. I’m older. I’m weeks from retirement. I’m afraid.
But robins don’t have the burden of choice. They obey their instinct every spring, just the same.
Today was my first day back on the hospital consultation-liaison service and I’m a little tired. I put about 2 miles and 22 floors on my step counter, which was a nice pace for starters. It’ll get busier as the COVID-19 surge develops over the next couple of weeks.
Being in phased retirement means I’m away for weeks, sometimes more than that. The pandemic changed many processes and policies while I was gone.
I think the biggest challenge I had this morning was just getting used to donning and doffing the face shield. I passed many people in the halls who are wearing them. My clumsiness was a little embarrassing. It took me a while just to figure out how to adjust the head band. But those who recommend them are right–they keep you from touching your face, which the masks don’t do.
You may have seen my YouTube video and the post on how to trim beards so they don’t interfere with the seal of the N95 masks. I even shaved mine off. Come to find out, I’ll probably never have to wear one given the shortages of masks generally.
I’m learning a lot of things on the fly and that includes how to use electronic gadgets to facilitate remote interviewing in order to cut down on spread of the virus.
I saw a lot more people in the stairwells and elevators were much less crowded.
It’s snowing today, starting this afternoon. It’s not a blizzard. It comes down slowly and peacefully. Occasionally I see people and their kids and dogs out walking in it, likely grateful for the fresh air. It’s hard to be stuck indoors, self-isolating because of the COVID-19 epidemic. We play cribbage.
Sena tried the grocery pickup thing in order to avoid crowds. She ordered yesterday and picked up this afternoon. For the most part, the shoppers did OK. We noticed that as she was ordering, items would be sold out even before and sometimes after (we found out later) the ordering was done.
But we were able to get toilet paper.
This epidemic changes your life in many ways. I’m in the latter stage of phased retirement and I’ll go back on the consultation-liaison psychiatry service in April. I expect it to be busy, but I’ll likely not do as many face-to-face interviews, depending on the situations in the emergency room and the general hospital.
I probably won’t carry around my camp stool, which I use to sit with patients when I interview them. It’s just another item that the coronavirus can stick to.
We’re told not to wear neckties because they’re germy, but I gave that up a long time ago for banded collar shirts. But now I’ll have to remember to keep my arms bare up to the elbows.
We’re also reminded to avoid elevators so as to maintain social distance (6 feet or 2 meters, roughly). I’ve been taking the stairs for years. Many people avoid the stairs.
I’ve gotten used to handwashing because I’m a hospitalist. I’ll wear masks a lot more frequently as well as don and doff personal protective equipment as needed more often.
I’m older and I worry a little bit about belonging to a higher risk age group for COVID-19 and being exposed more. On the other hand, I’m pretty healthy compared to a lot of patients younger than me.
I’m glad the next generation of doctors will be taking over, though.
I began rereading the book Invisible Man by Ralph Ellison today, which is Leap Day. Given what little I know about Leap Day and Leap Year in general, there isn’t a connection.
I first read Invisible Man well over 40 years ago. It was a paperback and I took it with me to Huston-Tillotson College in Austin, Texas (now Huston-Tillotson University), one of the historically black colleges and universities (HBCUs) in the United States.
It was very hot in Austin in my freshman year and the students didn’t have air-conditioned dormitories in those days. It must have been over 90 degrees. The glue melted on most of my paperback books, including Invisible Man. I suppose that’s why I eventually threw the book away, because it was falling apart.
After all these years, I bought a hardcover edition. We have air-conditioning now. I was motivated to read it again after I read Invisible Hawkeyes: African Americans at the University of Iowa during the Long Civil Rights Era, edited by Lena M. Hill and Michael D. Hill. See my blog posts, Milestones, and The Iowa River Landing Sculpture Walk, for background.
When I was a young man, I identified with the protagonist in Invisible Man. The Prologue still strikes a chord.
On the other hand, I googled my name today and found a few links that made me feel less invisible. Probably the most surprising link was to an interview with me entitled “James Amos, MD,” which you can read here. The piece evoked memories of a past version of me—which has not changed much since then. It mentions my former blog The Practical Psychosomaticist which I later renamed The Practical C-L Psychiatrist (C-L stands for Consultation-Liaison) after the flagship organization, the Academy of Psychosomatic Medicine changed its name to the Academy of C-L Psychiatry in response to a poll of its membership asking whether the name should be changed.
This biography makes me more visible, at least on the web. On the other hand, the blog no longer exists, due in part from my concerns about the General Data Protection Regulation (GDPR), which was enforced in 2018. I posted a lot of educational material about C-L Psychiatry on the blog along with pictures and presentations of my trainees. In a way, I did not protect their privacy and I was uncomfortable about that.
Other web pages surfaced during my self-googling. They included my article on delirium, “Psychiatrists Can Help Prevent Delirium,” posted on Psychiatric Times in 2011.
I also found my blog post on physician burnout, “How I left the walking dead for the walking dead meditation,” published on the Gold Foundation web site in 2014.
And there was my other Gold Foundation post about rude doctors, “Are doctors rude? An insider’s view,” posted in 2013.
There are a couple of petitions left over from years ago as well, about the controversial Maintenance of Certification (MOC) and the closure of state mental hospitals in Iowa several years ago.
I also found my review of Dr. Jenny Lind Porter’s book, The Lantern of Diogenes and Other Poems (published 1954).
The book seller’s note to me when Porter’s book was delivered in 2011 read as follows:
“Thanks for your purchase! It’s rare to find a book of this age that when you open the pages, it creaks like it is unread. I guess someone liked the way it looked on their bookshelf! Haha! Enjoy the book and Happy New Year, Rob J.”
An unread author is an invisible author. The first poem in the book is below:
The Lantern of Diogenes
by Jenny Lind Porter
All maturation has a root in quest.
How long thy wick has burned, Diogenes!
I see thy lantern bobbing in unrest
When others sit with babes upon their knees
Unconscious of the twilight or the storm,
Along the streets of Athens, glimmering strange,
Thine eyes upon the one thing keeps thee warm
In all this world of tempest and of change.
Along the pavestones of Florentian town
I see the shadows cower at thy flare,
In Rome and Paris; in an Oxford gown,
Men’s laughter could not shake the anxious care
Which had preserved thy lantern. May it be
That something of thy spirit burns in me!
Dr. Porter’s house in Austin, Texas was demolished a few years ago. There were plans to build a house there reminiscent of the architectural style of her original home and also a remembrance of her published work. I just noticed a satellite image of the property. There is no visible evidence that anything of that nature was ever built. Dr. Porter is, in a sense, invisible although her lantern still burns.
Visibility is a relative term. My advancing age and approaching retirement sometimes lead me to feel like I’m becoming invisible, gradually vanishing from the landscape of consultation-liaison psychiatry and general medicine.
Ralph Ellison’s book Invisible Man is a visible legacy. My legacy is small—yet the flame flickers, visible after all.
I got a nice, if puzzling surprise today. At a faculty meeting I was recognized for my 10-year anniversary of service at our hospital. It’s an important milestone, even if it is wrong. They scheduled this small event a couple of months ago, but I was too busy on the psychiatry consult service to break away. I also usually carry the pager for the trainees during the noon hour when the faculty meetings are held.
The 10-year anniversary recognition was very kind—except that I’ve been here for twenty odd years, not counting residency and medical school.
In all fairness, my department knows that and we shared a few jokes about it. I guess I should clarify that I have left the university for private practice a couple of times, which interrupts the years of service recognition timelines.
I was gone both times for a total of less than 12 months—just sayin’. I returned for a few reasons, although mainly because I missed teaching.
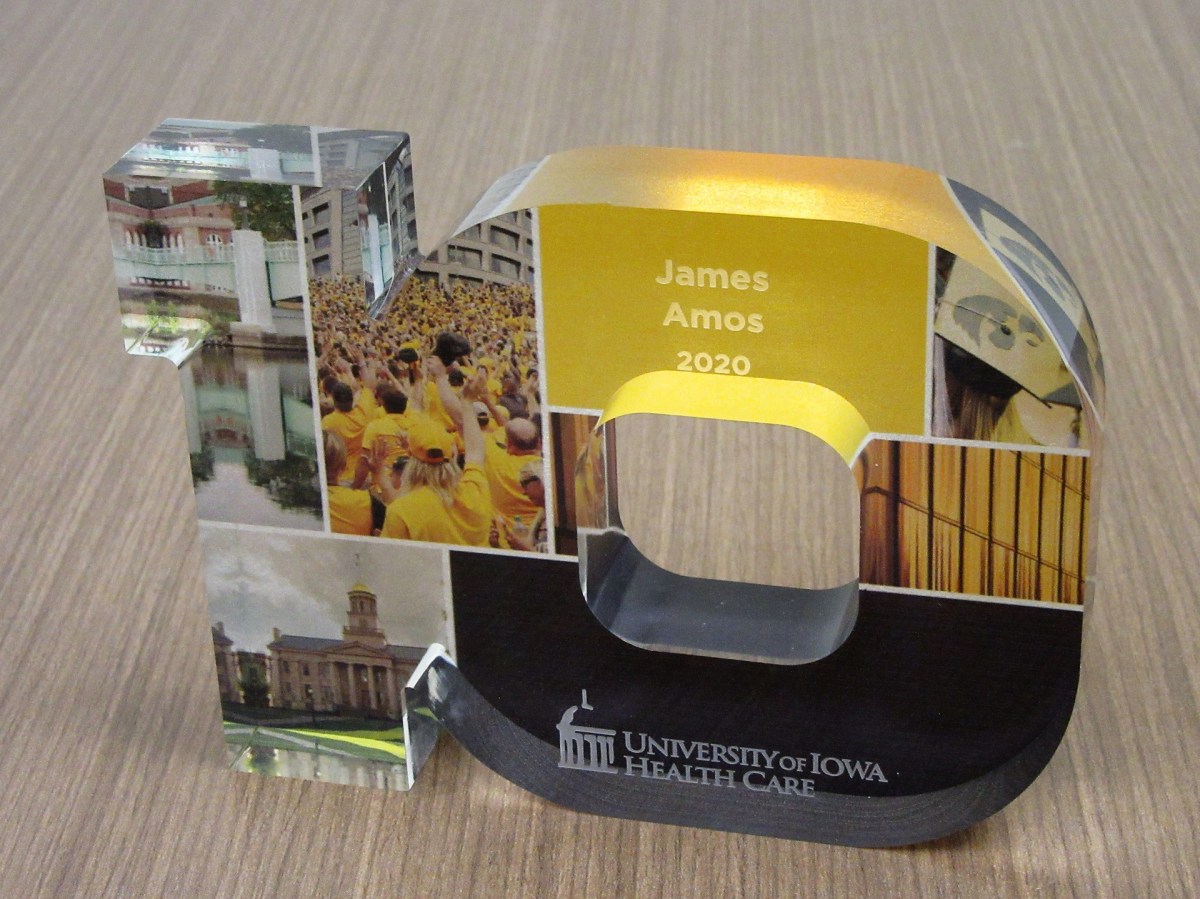
Anyway, I showed up at the faculty meeting, albeit a little guilty looking because I’m usually too busy to attend. My department chair arrived and said that she had to run back to get my “statue.”
That jarred me. Several years ago, when I had my first blog, The Practical Consultation-Liaison (C-L) Psychiatrist, I used to kid my readers that someday a statue of me would be erected in the university Quad. It would be made of Play-Doh.
And that’s why I asked her as she turned to leave, “Is it made of Play-Doh?” She looked puzzled and I didn’t really think I could explain in a way that wouldn’t make me look like I’d been smoking something illegal.
The “statue” is a handsome little sculpture of the number 10, standing for 10 years of service. It has color photos embedded in it of various aspects of academic life at the University of Iowa, many of which I’ve had the privilege of enjoying in the 30 odd years my wife, Sena, and I have been in Iowa City.
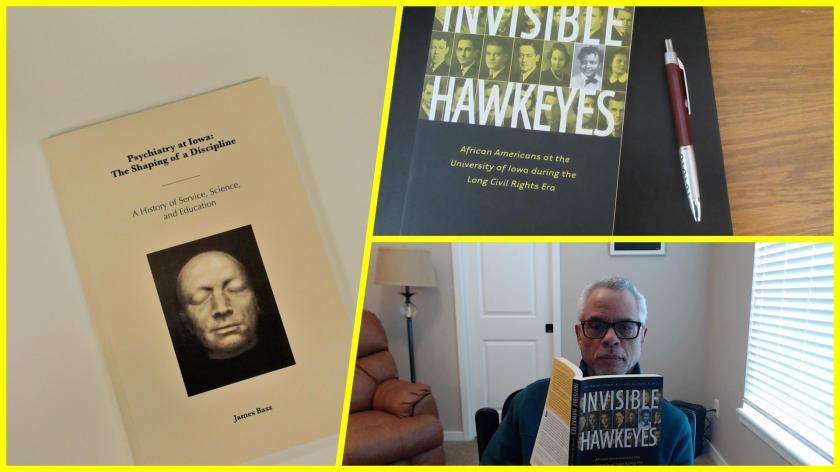
Just before the meeting, I had walked up to the 8th floor (I always take the stairs) to the psychiatry department offices to see if I could get a copy of the recently published history of the department, Psychiatry at Iowa: The Shaping of a Discipline: A History of Service, Science, and Education, written by James Bass.
Mr. Bass interviewed many people in the department, including me. I didn’t expect that my perspective on the consultation service, the clinical track, or my race would even get mentioned. However, 2 out of 3 made it into print.
It didn’t really surprise me that my being African American was not mentioned. I think I’m probably the only African American faculty member of the department in its 100-year history, at least until very recently.
It reminded me of another book that I just acquired, Invisible Hawkeyes: African Americans at the University of Iowa during the Long Civil Rights Era, edited by Lena M. Hill and Michael D. Hill.
In a small way, I’m making the invisible visible.
Making the invisible visible
And also, because it’s great for my ego, I’m going to quote what Bass wrote about me in Chapter 5, The New Path of George Winokur, 1971-1990:
“If in Iowa’s Department of Psychiatry there is an essential example of the consultation-liaison psychiatrist, it would be Dr. James Amos. A true in-the-trenches clinician and teacher, Amos’s potential was first spotted by George Winokur and then cultivated by Winokur’s successor, Bob Robinson. Robinson initially sought a research gene in Amos, but, as Amos would be the first to state, clinical work—not research—would be Amos’s true calling. With Russell Noyes, before Noyes’ retirement in 2002, Amos ran the UIHC psychiatry consultation service and then continued on, heroically serving an 811-bed hospital. In 2010 he would edit a book with Robinson entitled Psychosomatic Medicine: An Introduction to Consultation-Liaison Psychiatry.” (Bass, J. (2019). Psychiatry at Iowa: A History of Service, Science, and Education. Iowa City, Iowa, The University of Iowa Department of Psychiatry).
In chapter 6 (Robert G. Robinson and the Widening of Basic Science, 1990-2011), he mentions my name in the context of being one of the first clinical track faculty in the department. In some ways, breaking ground as a clinical track faculty was probably harder than being the only African American faculty member in the department.
As retirement approaches this coming June, I look back at what others and I worked together to accomplish within consultation-liaison psychiatry. The challenges were best described by a former President of the Academy of Consultation-Liaison Psychiatry, Thomas Hackett (this quote I helped find for James Bass and anyone can view it on the Internet Archive):
“A distinction must be made between a consultation service and a consultation liaison service. A consultation service is a rescue squad. It responds to requests from other services for help with the diagnosis, treatment, or disposition of perplexing patients. At worst, consultation work is nothing more than a brief foray into the territory of another service, usually ending with a note written in the chart outlining a plan of action. The actual intervention is left to the consultee. Like a volunteer firefighter, a consultant puts out the blaze and then returns home. Like a volunteer fire brigade, a consultation service seldom has the time or manpower to set up fire prevention programs or to educate the citizenry about fireproofing. A consultation service is the most common type of psychiatric-medical interface found in departments of psychiatry around the United States today.
A liaison service requires manpower, money, and motivation. Sufficient personnel are necessary to allow the psychiatric consultant time to perform services other than simply interviewing troublesome patients in the area assigned. He must be able to attend rounds, discuss patients individually with house officers, and hold teaching sessions for nurses. Liaison work is further distinguished from consultation activity in that patients are seen at the discretion of the psychiatric consultant as well as the referring physician. Because the consultant attends social service rounds with the house officers, he is able to spot potential psychiatric problems.”— Hackett, T. P., MD (1978). Beginnings: liaison psychiatry in a general hospital. Massachusetts General Hospital: Handbook of general hospital psychiatry. T. P. Hackett, MD and N. H. Cassem, MD. St. Louis, Missouri, The C.V. Mosby Company: 1-14.
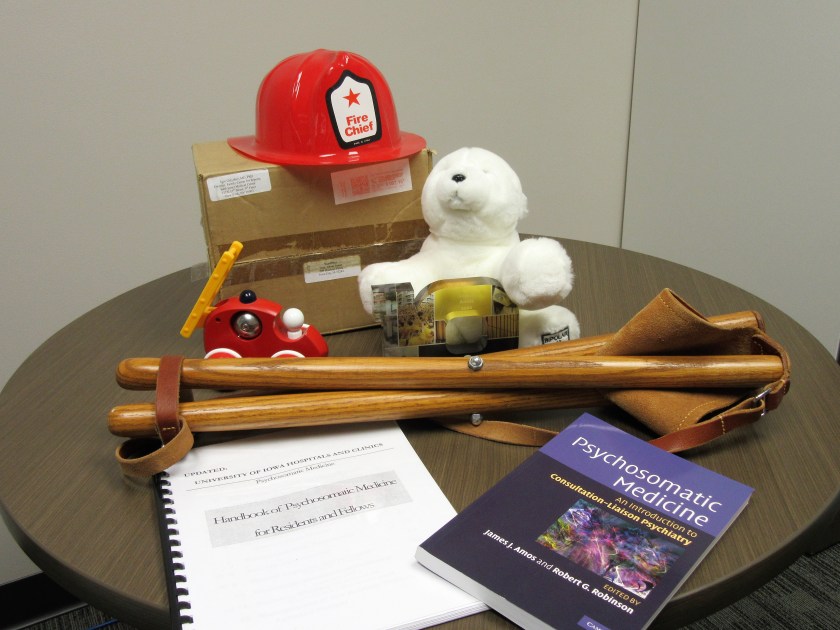
I have what seems like precious few mementos of my sojourn here in the department and, indeed, on this earth. I have a toy fireman’s helmet I found hanging in a plastic sack on my office doorknob one day. It was a gift from a Family Medicine resident who rotated on the consult service and who learned why I called it a fire brigade.
For the same reason, I have a toy fire truck, sent to me by a New York psychoanalyst who was also a blogger.
I have Bumpy the Bipolar Bear, believe or not, sent to me by psychiatrist, Dr. Igor Galynker, about whose emergency room suicide risk assessment method I had blogged about several years ago. C-L psychiatrists do a lot of suicide risk assessments in the hospital and the clinics. I still have the box with the address to me:
WordPress
Attn: James Amos
200 Hawkins Drive
Iowa City, IA 52242
I have my first homemade handbook for C-L Psychiatry and the published handbook that eventually replaced it. Thank goodness the leaders of the Academy of Consultation-Liaison Psychiatry listened to the membership and changed the name from Psychosomatic Medicine to C-L Psychiatry.
I have an award for being an excellent clinical coach.
And I have my little camp stool, which a colleague who is a surgeon and emergency medicine physician gave me and which allows me to sit with my patients anywhere in the hospital, so that I don’t have to stand over them.
It will all fit in a cardboard box on my last day—the next milestone.
I had so much fun with the giant chicken post on January 25, 2020 that I thought it would be nice to revisit the subject, only this time take a butt-freezing tour of the entire Iowa River Landing (IRL) Sculpture Walk.
We took the walk Tuesday, January 28, 2020. The weather was typical for Iowa in January. The temperature was in the teens and there were brief flurries. My wife, Sena, and I dressed warm and took a meandering journey through the Sculpture Walk, guided by a small map.
It was a little more challenging because snow and ice covered up many of the plaques identifying the works (and parts of the sculptures as well) although this lent even more visual interest to them. They’re three dimensional objects anyway and you really have to walk around them to fully appreciate their complexity. You have to watch out for yellow snow.
What made this adventure even more special was the Iowa Writers’ Library in the lobby of the Coralville Marriott Hotel and Conference Center. It’s maintained by the Coralville Public Library. One of the issues I had was being unfamiliar with the text of the poems and other literary works (all were connected with the Iowa Writers’ Workshop) referenced by the artists. The library was cozy, had a fireplace warming the softly lit room lined by bookshelves and a couple of ladders on wheels to help you reach the books higher up.
I have always felt comforted in libraries, ever since I was a little boy. Every day I got the chance, I would walk to my hometown library (which was about a mile trip), browse the stacks for hours, then tote home piles of books in both arms.
The hotel library had most of the books pertinent to the literary references cited by the artists for their sculptures. I even found David B. Axelrod’s book, The Man Who Fell in Love with a Chicken. It turns out that the title of Axelrod’s poem is “The Man Who Fell in Love with His Chicken.” There, I’ve said enough already about that chicken.
Of course, I couldn’t take the time to find and read every book; we would not have had time to freeze our butts off touring the sculptures.
I didn’t wear my heavy winter boots and had to crunch through the crusty snow nearly up to my ankles to reach certain sculptures. Sena was dressed better for the weather but we both slipped around on the ice and I began to think more and more about things like broken hips.
But we soldiered on because it was necessary to walk completely around the Made of Money sculpture by Aaron Wilson in order to see the message printed, “HOW CAN WE HELP YOU?” It’s funny because that’s what I typically ask patients in the general hospital when I sit down on my little camp stool after I introduce myself to them as a consultation-liaison psychiatrist.
The sculpture To Dorothy, by artist James Anthony Bearden, was in a difficult spot and initially we thought we’d have to either rappel down from the roof of the building it was in front of or climb up the big retaining walls to get a good look at it. We found a way out to it and ignored passersby who gawked at us. They needed to admire us for how unique we are (not how eccentric and possibly a danger to ourselves and others), which is what I think Iowa Poet Laureate Marvin Bell was getting at in his poem of the same title as Bearden’s sculpture.
The sculpture, A Thousand Acres, by artist V. Skip Willits was another piece you really have to walk around to fully appreciate, although you generally have to do that with any sculpture. The book of the same title by Jane Smiley is based on Shakespeare’s King Lear—which I have also never read—but which I got an earful about in my undergraduate days from a fellow student who thought he knew everything there was to know about King Lear. He was garrulous in the extreme and bested me in debating class mainly because he never let me open my mouth.
The sculpture by artist Victoria Ann Reed, called Convergence, was very intriguing and looked more like a human figure who had been through a wormhole than a memory.
The Tipping Point, by artist Sarah Deppe, was a convincing image of persons with holes in their heads (several holes in fact). Bureaucrats come to mind.
We nearly dismissed the sculpture called After Trillium by artist Anthony Castronovo as a broken lamppost with dysfunctional solar panels, only partly because snow and ice covered the panel describing it. On the other hand, the top part does resemble a flower called a Trillium, not to be confused with Trillian, a character in the book by Douglas Adams, The Ultimate Hitchhiker’s Guide to the Galaxy. I’m glad I could clear that up for you.
The Prairie Breeze Bench by artist Bounnak Thammavong is a sculpture you could actually sit on and watch the Bald Eagles. However, it’s made of steel and the seat was covered by snow. After you wipe away the Bald Eagle droppings, you can read the poem by James Hearst, “Landscape Iowa.” You can also hear it set to music and performed by Scott Cawelti, a former University of Northern Iowa educator who taught film, writing, and literature courses. He also edited The Complete Poetry of James Hearst (University of Iowa Press, 2001).
The Alidade sculpture by Dan Perry was the one Sena and I both really liked. I know Perry says the alidade was used by astronomers but I remember it as being a part of an instrument used by land surveyors, also for measuring distance and angles in topographical surveys. I used to work for consulting engineers as a surveyor’s assistance and draftsman many years ago. Perry links it to the poem entitled “1,2,3” from James Galvin’s book of poems, X: Poems. I confess I don’t see the connection yet. The poem for the most part reminds me of spelunking although Galvin describes a hole that he and a friend rappel into as being a planet. Much of the rest seems to be about something very painful. I’m sorry I can’t do better, but that’s why he’s a poet and I’m not.
Next, we encountered Bounnak Thammavong’s second sculpture, a very recognizable fish, a “lowly river carp,” entitled From the River. It’s linked to the poem “Where Water Comes Together with Other Water” by Raymond Carver. When I was a boy, I used to fish for bullhead in my hometown river. I sometimes caught carp and thought that was the poorer catch. It didn’t matter. I always threw both back into the river. My mom would not clean fish and neither would I.
Finally, by a pretty circuitous route, we saw the last sculpture, Gilead, by artist Kristin Garnant. The snow plow had piled up a lot of snow around it. I probably won’t read Gilead, the epistolary novel by Marilynne Robinson.
In fact, I probably won’t read a lot of the literature connected with the sculptures we saw. I did read Margaret Walker’s poem “For My people.” Sorry, Jubilee is way too much for me. She was the first African-American woman to be accepted into the Iowa Writers’ Workshop, of course depending on which story you believe about when the program formally began (Invisible Hawkeyes: African Americans at the University of Iowa during the Long Civil Rights Era, in Chapter Four: Obscured Traditions: Blacks at the Iowa Writers’ Workshop, 1940-1965, by Michael D. Hill, University of Iowa Press, 2016).
In some ways, I identify way with her, one of the reasons being obvious and skin-deep. The other is that she taught school at Jackson State, a historically black college in Jackson, Mississippi.
I wonder if the IRL Sculpture Walk could include another one for her, just to make it an even dozen?
I spent my Freshman and Sophomore college years at a historically black college. It was then called Huston-Tillotson College (now Huston-Tillotson University) in Austin, Texas. That was back in the mid-1970s. I had grown up in largely white neighborhoods and gone to predominantly white schools prior to going to H-TC. It was a culture shock and that’s probably about all I’ll say about it for now, since this post is way too long.
I can say one other thing about H-TC. I submitted a poem for the college’s annual poetry contest. Winners would have their work published in the school’s small anthology called Habari Gani (Swahili for What’s Going On?). Mine didn’t make it but years later I scoured the web looking for a way to get a copy of Habari Gani, finally succeeding only a few years ago after tracking a copy of the Spring 1975 volume down at the H-TU library. I like the short introductory poem:
The Martin Luther King Jr. Day of Service is today and the University of Iowa has taken a quote from King to set the tone each year for this event. This year it is:
“Let us build bridges rather than barriers, openness rather than walls. Rather than borders, let us look at distant horizons together in a spirit of acceptance, helpfulness, cooperation, peace, kindness and especially love.”—Dr. Martin Luther King, Jr.
Dr. Martin Luther King, Jr.
As I look back on my career in medicine, it’s only natural for me to think of my role as a consultation-liaison psychiatrist as a sort of bridge between medicine and psychiatry. I’m pretty sure most would agree that as I chased around the hospital up and down the stairs doing the 3 and 30 (3 miles and 30 floors; I never take the elevator), I was doing my level best to bring psychiatric care to the patients in the general hospital who were suffering from medical illness as well.
The featured image shows the cover of a little book of kind remembrances I received from colleagues and trainees when, during one of my two such lapses in good judgment, I left the University of Iowa to have a try at private practice. The book has an image of a bridge on it. At the time, I thought of it as a depiction of my path between academia and community psychiatry. We need bridges there too, although one person let me know that someone has to teach new doctors.
I also got a fancy birdhouse as a going-away gift. I still do some bird-watching.
Starlings on ice
As I head into retirement, I hope that I’ve been a bridge of sorts between the old ways and the new to the next generation of doctors. After all, I’m the institutional memory of psychiatry on the medical and surgical units, in a manner of speaking.
The Medical-Psychiatry Unit (MPU) at University of Iowa Hospitals & Clinics was where I learned how this ward of patients with both medical and psychiatric illness served as a bridge between the departments of psychiatry and medicine. My teachers were doctors who were and still are great leaders. I still recall Dr. Roger Kathol, MD, an internist who also trained in psychiatry, and who designed and started the MPU decades ago, gave readings during sit-down rounds in the unit conference room. He read passages from the works of Galen, the Greek physician, surgeon, and philosopher in the Roman Empire.
Dr. Kathol assigned to me a task one day, which was to give a short presentation the following day on hyponatremia and how to distinguish psychogenic polydipsia from the Syndrome of Inappropriate Antidiuretic Hormone (SIADH). That night I was on call and got 4 admissions on the unit, which was chaotic. One patient actually broke a bed. I didn’t get any sleep. I was up running around until we all sat down to discuss patients.
I struggled through presentations of the 4 patients I had admitted the night before. I could barely talk. I had actually looked up a little information for my assigned presentation on hyponatremia but I was sweating it because I could barely stay awake. I was not the first resident to have episodes of microsleep on rounds and I knew Dr. Kathol saw it happening to me. That was in the days of 32 hours of call. They don’t make trainees do that now.
Dr. Kathol gave me sort of a sidelong glance as we finished discussing patients, which was usually when trainees were expected to give short educational talks. That day, he skipped me.
I should mention that he thought the proper name for the MPU was the Complexity Intervention Unit (CIU), owing to not just the medical and psychiatric complexity of our patients, but also to their social environments and the U.S. payer system which often led to many having inadequate, dis-integrated health care, meaning that there was no bridge between psychiatric and medical illness treatment and split health insurance coverage even though research showed that mental illness definitely lessened quality of life and increased health care costs. He has his own company, aptly named Cartesian Solutions, and it’s a major organization dedicated to helping hospitals and clinics set up collaborative ways to bridge the needs of patients with comorbid psychiatric and medical illness.
The University of Iowa model for the MPU has been disseminated to a number of other hospitals in the country, one of them in Pennsylvania, which I mentioned in a previous post, “Brief News Item,” on May 23, 2019. I’ve just received word a couple of days ago from Dr. Kolin Good that the unit, called the Medical Complexity Unit (MCU), a name which bridges the underlying intent of MPU and CIU, has saved the hospital a great deal of money, has drastically cut the use of sitters doing one to one observation (an extremely expensive intervention), is treasured by patients, and popular with trainees. They are very proud of it and have every right to be so. They are bridge builders too.
Dr. Louis Kirchhoff has been one the most notable internal medicine co-attendings on the MPU. He’s an infectious disease specialist, but has a knack for communicating effectively with patients who are mentally and medically ill, even speaking fluent Spanish with some of them. He and I shared triage call to the MPU every other night before the triage system was changed to a more humane schedule. He was a bridge between internal medicine and psychiatry trainees rotating on the ward. He could explain psychiatry to the medicine residents as well as I could.
I have had a penchant for finding a chair to sit down when I interview patients in their hospital rooms. There are usually not enough chairs in the rooms. A few years ago, Dr. Tim Thomsen, a surgeon and Palliative Care Medicine specialist as well, lent me a camp stool which I carry around with me so that I’m never at a loss for a chair. Everyone likes it. I think the camp stool helps build an emotional bridge with patients.
The little chair
There are special combined specialty residencies at the University of Iowa Hospitals and Clinics which bridge Internal Medicine and Psychiatry and Family medicine and Psychiatry. Slowly but surely the siloed departments of academic medical centers are broadening their curricula and training regimens to rebuild the bridge between mind and body.
It’s been evolving for years. I’m proud to have played a small role in it. This is a place where teachers, researchers, and clinicians build bridges in many ways, foster openness, and search the “distant horizons in a spirit of acceptance, helpfulness, cooperation, peace, kindness and especially love.”
I took the picture of the little chair one of the residents brought to the psychiatry consult office yesterday. I got a big charge out of it, especially because I’ve been using a version made of wood and leather for a few years now. I think it’s possible that it could be an auspicious chair.
The resident actually used his, too. It was a busy day; I put in about 4 miles and 40 floors on my step counter—which meant the residents did too. The chair is obviously useful to rest our feet, but I think Thomas P. Hackett summed up the best ever rationale for sitting with patients:
“As a matter of courtesy, I sit down when interviewing or visiting patients. Long accustomed to the ritual of making rounds, many physicians remain standing as a matter of course. Standing, physicians remind me of missiles about to be launched, poised to depart. Even if that is not necessarily true, they look the part. Patients sense this and it limits conversation. In addition, when standing, the physician necessarily looks down on the patient. This disparity in height is apt to encourage the attribution of arrogance. Looking down at a patient who is prone emphasizes the dependency of the position. Sitting at the bedside equalizes station. Sitting with a patient need not take longer than standing with him.”— Hackett, T. P., MD (1978). Beginnings: liaison psychiatry in a general hospital. Massachusetts General Hospital: Handbook of general hospital psychiatry. T. P. Hackett, MD and N. H. Cassem, MD. St. Louis, Missouri, The C.V. Mosby Company: 1-14.
I had a little fun with the chair in a YouTube video as well.
The chair I use now is a replacement for the first one I got as a sort of loaner from a colleague in Palliative Care Medicine. That one broke during a consultation visit with a patient and his family (circumstances disguised to protect confidentiality) in the emergency room in which we were asked to evaluate for catatonia. The patient was mute but there was little evidence otherwise for catatonia, one of the chief features of which is the inability to react to any stimulus in the environment. I was sitting on the chair explaining in detail the intravenous lorazepam challenge test for catatonia (which often interrupts the episode of muteness and immobility).
I was sitting in front of the patient but facing the family and the consult service trainees while expatiating on the topic. As I was droning on, I heard a sudden pop—and I fell unceremoniously on my rear end as the chair collapsed beneath me.
My audience exploded in loud laughter, of course, as you’d expect when a pompous ass falls on his ass. But they also pointed to the patient. When I turned to look at him, he was convulsed with apparent mirth although still unable to make a sound.
I considered this a novel test for catatonia, negative in this case. Of course, it would be impractical for regular use.
Where was I? Oh, the little chair the resident brought for consult rounds. I was honored by it. It seemed to show that I was leaving a legacy as I head for retirement in June.
Another sign of leaving a legacy was a New Year’s email message I got from a former resident, Dr. Paul Thisayakorn, MD, who has been making an auspicious beginning in the field of consultation-liaison psychiatry in Thailand. He’s working very hard and is an outstanding clinician, researcher, and teacher. He has a lovely family. He and I respect each other a great deal.
Speaking of auspicious, when Paul graduated from our psychiatry residency and before leaving for his Consultation-Liaison fellowship program, he gave me a necktie with white elephants printed on it. I still have it. I may not have the symbolic meaning of the white elephant exactly right, but I think the white elephant in Thai culture is called “chang samkhan,” or maybe “chang phueak” which means “auspicious elephant.” In general, I think the idea is they symbolize success or at least the promise of success. Paul’s gift showed his gratitude and respect for me because I was one of his teachers. I am still honored to have been a part of his education and his life. I will always treasure his gift of gratitude.
An auspicious tie
Paul is very hard-working and very successful. And if the residents now start to use the little camp stools to sit with their patients, I would treasure that legacy as well.