I’m coming up on my last 3 days for the academic year and
reflecting now that my favorite season is upon us. Spring does that to me,
especially now that I’ve been in the phased retirement contract for the last 2
years. I’ll be going into the 3rd and final year as of July.
I just found out that next week I’ll be among those faculty members selected to receive the Excellence in Clinical Coaching Award from the Gradual Medical Education Office at the Leadership Symposium.
I’ve received teaching awards from the residents at
graduation time (another sign of spring!) over the years and I’m always grateful
for their recognition. The Excellence in Clinical Coaching Award is recognition
from my department as a whole, the members of which put together a nomination
package including letters from department leaders as well as trainees.
I’m also humbled by
it because I’ve learned a lot from everyone with whom I’ve had the privilege of
working, but my favorites are the trainees, including medical students. In
fact, I learned from them again in the last week or so. Three talented medical
students gave outstanding presentations about issues relevant to all
physicians, not just psychiatrists.
They will be excellent physicians. They will teach others.
They will lead and it’s a good thing—medicine needs them.
I like the coach idea. I know one of the internal medicine residents thought of me as a mentor. I’m aware of the differences between mentors and coaches as well as the similarities.
Coaches spend relatively less time with learners and the
focus of the relationship is usually a set of specific skills which needs to be
passed on. Mentors tend to develop longer term relationships and guide learners
in broader ways in terms of career goals and more.
However, both mentors and coaches serve as role models,
something all teachers do—including trainees.
That’s partly why I feel less troubled about retiring as my
time to leave draws nearer. I trust the next generation of doctors and, just
like the Supremes song says, “You better make way for the young folks.” It’s my
time to leave. It’s their time to live.
Well, we missed Earth Day this year, which fell on April 22nd. The theme was to protect threatened and endangered species. One excuse is that we’ve been too focused on the cardinals building a nest in our back yard this spring. They are neither threatened nor endangered. I would call them fussy, especially when we get too close to the nest in our evergreen tree.
My other excuse is that April 22, 2019 was the day I had my
last official work-related CPR recertification. It’s valid for two years but I’ll
be retired next year. CPR is very important and I take the class seriously. I
always seem to have a problem getting the bag mask tight enough on the
mannequin’s face to get a good breath in.
This year there was an electronic device to monitor the
quality of your chest compressions. It lights up green to let you know when they’re
adequate. Orange lights means you have to fix your technique. That was new for
me and I was probably not letting up enough to let the heart fill. Imagine
that. I’ve probably had poor technique for years.
Getting back to the cardinals, we’ve noticed that there are two eggs, off white with brown speckles. We’ve never seen eggs like that and we can distinguish them from the eggs of robins and chipping sparrows. The cardinal parents chirp pretty loudly at us whenever we get too close to the tree.
Northern Cardinal eggs…we’re pretty sure.
Also, it’s Hosta planting time in the back-yard garden, a
job my wife does because my form with a shovel is just as bad as my chest
compressions and bag breathing on the CPR mannequin.
Last year, we got out for Earth Day and I found an old polaroid camera while we were out on the Clear Creek Trail. I’m not sure how harmful it was to the environment. Judging from its condition, the environment was more harmful to the polaroid.
Polaroid in good condition.
On the other hand, we did spot a plastic bottle, which is harmful to the environment. We did the appropriate thing by dropping it in the proper trash receptacle.
Plastic goes in the trash.
Today is National DNA Day, which celebrates the discovery
and understanding of DNA and the scientific advances that understanding has
made possible. About the only thing important to me about it is that there are a
few things that are definitely not in my DNA:
Cooking—unless it’s sticking a frozen pizza in the oven.
Planting Hostas.
Bag breathing the CPR mannequins.
Reading, listening to, or watching political news.
Eating shredded coconut.
Sitting in a psychiatry outpatient clinic, waiting for no-shows.
Waiting in airports.
Shopping for anything.
Removing or spreading mulch.
It’s an incomplete list, of course. Happy DNA Day!
The cardinal nest is pretty much done—no eggs yet, though. At least we think it’s a cardinal nest. It looks typical according to experts; loosely woven of twigs, leaves, stucco, and ponderosa pine accents. They’re pretty fussy about us snooping around the backyard evergreen tree they chose to build a home in.
Any day now, we’re hoping to see a clutch of eggs, bluish
white with brown markings. Or maybe pale green with brown-lilac spots. Or
possibly whitish to pale bluish or greenish white, marked with brown, purple,
and gray. Or Hawkeye black and gold. It all depends on which guidebook you read,
I guess.
I’m gradually getting back into bird watching and spending
less time with my head at the hospital (“Earth to Jim!”). Doctors learn to
spend all their time either on the wards or in the clinic. It reminds me of a
couple of scenes from Men in Black (MIB) II.
As Agent J walks into the MIB complex at Battery Park, the
elevator dude says “Don’t you ever go home? Agent J says “Nope.”
Later he drops into Zed’s office and asks, “What you got for
me?”
Zed replies, “Look. See those guys in black suits? They work
here. We got it covered.”
That’s how physicians can get after years of acculturation
into the driven doctor model. Often enough, I take most of the work away from
the trainees, when they’re not looking. And I take my work home—that’s called
pajama time.
Hey, those dudes work here too. I have a tendency to see
myself as almost indispensable, which makes it hard to envision retirement at
times.
I have to keep reminding myself that I’m not the only doc who can do my job. The next generation of doctors are eager and ready. They deserve a chance. But I sometimes catch myself telling old war stories about how hard it was when I was a resident or a junior attending.
“I remember when I had to walk 40 miles to work in the driving
blizzard alternating with blazing heat (it’s Iowa) to get to my 6 x10 foot
office in the basement to stoke the fire in the pot-bellied stove for coffee
and grits at 4:00 in the morning, before the damn birds even get up, milk a few
dozen cows in the atrium, chase the pigs out of the operating rooms and then go
see about a hundred or so consultations before 7:00 in the morning I tell you, then
write notes until midnight, be on call until 3:30 the next morning and do it
all over again. What do you guys know about work?”
I may exaggerate a little bit. Usually there weren’t that
many cows in the atrium.
It can be difficult to unwind from the physician’s
treadmill. But as time goes on, I look forward to seeing the birds build nests,
to see the brand-new eggs, the ugly chicks who look like little dinosaurs until
the feathers grow out. I can pay more attention to the world outside the
hospital, where the new doctors are stoking the fire.
I’m a big fan of the Men in Black movies. I’m not going to
tell you how many times I’ve watched them on TV (78 million and if that number
reminds you of a scene from Men in Black, you’re just as much a fan as I am, if
not worse). One of my favorite lines is when Zed says to Edwards, “Edwards.
Let’s put it on.” Edwards asks, “Put what on?” And Zed says, “The last suit
you’ll ever wear.”
Today, I asked my secretary to order some new white coats for me. I went down to the Uniform Shop and checked on it. All they need is the requisition and they’ll get it.
Since I’m retiring after this year, these are the last white coats I’ll ever wear. There’s no Zed to tell me that. The Uniform Shop staff person won’t know it when the coats arrive—unless I tell her, of course.
I found a very long, involved discussion on the web about the meaning of Zed’s “last suit you’ll ever wear” statement. All I got out of it was that some people take that movie way too seriously.
But for me the last white coat I’ll ever wear means exactly that. I’m going to wear the coat until I retire (in about 14 months according to the countdown)—and then I’m never going to wear white coats again.
I can almost hear certain persons snickering in the background. I suspect there may be a few bets about this retirement thing being another temporary leave-taking, like the times I left for private practice and came back, sort of like bringing Agent K back after neuralyzing him at his request. He really did retire—temporarily.
But nobody is going to neuralyze me. I’ll keep a lot of
memories about my time as a Consultation-liaison (C-L) Psychiatrist, even
though some of them are sort of like Agent K’s memories of being swallowed by a
giant interstellar cockroach.
However, that reminds me of a few thoughts I have about institutional memory. I’ve mentioned my concerns about being practically the only C-L Psychiatrist in a pretty big hospital and retiring. I’m a geezer, but I know a lot about the ins and outs and moving parts and what it means to be a one-man hit-and-run fireman psychiatric consultant in a large academic medical center.
Institutional memory…
Institutional memory has been defined as “the collective
knowledge and learned experiences of a group. As turnover occurs among group
members, these concepts must be transitioned. Knowledge management tools aim to
capture and preserve these memories.”
Institutional memory can also be characterized briefly as:
Accumulated knowledge, skills, “this is the way we do things”
Some of it gets hardened into policies and procedures
Much of it “…resides in the heads, hands, and hearts of individual managers and functional experts.”- “How to Preserve Institutional Knowledge” by Ron Ashkenas, Harvard Business Review, 2013
Too much of anything for too long can be bad, including institutional memory
The bullet point that Ron Ashkenas makes above is relevant
to employers of baby boomers like me who know informal procedures, and have the
skills (and they chose us so they recognized the skills, so don’t be calling us
sport, feisty, hon, sweetie, or anything like that) and knowledge that’s in our
heads but may not be stored anywhere else.
That makes the baby boomer retirement phenomenon a real challenge. About 10,000 boomers will reach the age of 65 every day for the next 15 years. And most of us aren’t kidding around. There’s no way to just deneuralyze us to make us come back. You can’t make it happ’n Cap’n.
There are ways to package institutional memory into handy
things like mentoring partnerships, knowledge wikis, snappy videos (just shoot
the damn thing!) and other media that are easily accessible and geared for the
adult learner.
You can’t beat the Internet Archives for history. You can borrow and read the first edition of the Massachusetts General Hospital Handbook of general hospital psychiatry published in 1978, just like checking it out from a public library. Read the chapter, “Beginnings: liaison psychiatry in a general hospital.” You can learn from Dr. Thomas P. Hackett about the difference between a consultation service and a liaison service:
digital institutional memory
“A distinction must be made between a consultation service
and a consultation liaison service. A
consultation service is a rescue squad.
It responds to requests from other services for help with the diagnosis,
treatment, or disposition of perplexing patients. At worst, consultation work is nothing more
than a brief foray into the territory of another service, usually ending with a
note written in the chart outlining a plan of action. The actual intervention is left to the
consultee. Like a volunteer firefighter,
a consultant puts out the blaze and then returns home. Like a volunteer fire brigade, a consultation
service seldom has the time or manpower to set up fire prevention programs or
to educate the citizenry about fireproofing.
A consultation service is the most common type of psychiatric-medical
interface found in departments of psychiatry around the United States today.
A liaison service requires manpower, money, and
motivation. Sufficient personnel are
necessary to allow the psychiatric consultant time to perform services other
than simply interviewing troublesome patients in the area assigned. He must be able to attend rounds, discuss
patients individually with house officers, and hold teaching sessions for
nurses. Liaison work is further distinguished from consultation activity in
that patients are seen at the discretion of the psychiatric consultant as well
as the referring physician. Because the
consultant attends social service rounds with the house officers, he is able to
spot potential psychiatric problems.”—T. P. Hackett, MD.
By the way, have you seen my YouTube Channel? I’ve been beaming me up into educational videos for residents and medical students for a while now.
Next year I’ll be
doffing the white coat for good—but I’ll be on THIS planet.
Reference:
Hackett,
T. P., MD (1978). Beginnings: liaison psychiatry in a general hospital. Massachusetts
General Hospital: Handbook of general hospital psychiatry. T. P. Hackett, MD
and N. H. Cassem, MD. St. Louis, Missouri, The C.V. Mosby Company: 1-14.
I’m noticing something about my readiness for retirement.
Certain activities are starting to be at least as interesting as my work as a
consultation-liaison psychiatrist at the hospital—maybe even more so.
For example, my wife and I are hoping that the cardinals
will come back to our backyard evergreen tree. They were building a Hoorah’s
Nest in there a week ago, which I took a picture of and then they left when they
saw us spying on them. This evening, my wife noticed they were back. We rushed
to the window (me with camera in hand) and I swear, they peered at us with
intense suspicion. Pretty soon, they flew off in a huff.
They are among the most stand-offish backyard birds I’ve
ever seen.
Why is this so important? It’s because I am getting so
absorbed in birdwatching again now that I’m in phased retirement that I find it
fascinating enough to look forward to more than going to work. I think that’s a
sign I’m finally beginning to adjust to retirement.
I spent 4 years in medical school, 4 years in residency, and
have worked for more than 23 years as a psychiatrist, mostly as a general
hospital consultant. Nothing used to jazz me as much as running around the
hospital, seeing patients in nearly all specialties, evaluating and helping
treat many fascinating neuropsychiatric syndromes, teaching medical students
and residents, and I even wrote a book.
On the other hand, I don’t want to hang on too long. When
people ask me why I’m retiring so early (“You’re so young!”), I just tell them
most physicians retire at my age, around 65. I also say that I want to leave at
the top of my game—and not nudged out because I’m faltering.
I saw a blog post that identified that reason for retirement. It was entitled “When Physicians Reach Their Use-By Date,” by James Allen, MD. The site is identified as “Not secure” unfortunately, so I’m not giving a link to it. However, the web site is The Hospital Medical Director and it’s sponsored by Ohio State University–so it’s probably safe.
Now if you do read Dr. Allen’s post, you’ll think I’m
flattering myself as a “master clinician.” I don’t think of myself that way. I’m
actually more of a demigod.
I’m just kidding. The descriptions of how physicians finally reach retirement sound fascinating. I’m not sure I could just abruptly stop—that’s why I chose phased retirement. Staying on as a preceptor is not appealing to me because I liked the clinical action too much. I’m actually afraid of becoming someone who knows only medicine. It’s one of the best reasons for me to retire sooner rather than later. You’d think I’d identify with the consultant model; I’ve briefly thought of carrying my resignation letter around with me, although not in my coat pocket and not with malice in my heart.
Although I joined the fraternity of medicine, so to speak, I’m
really not a joiner. In fact, I’ve gradually given up membership in organizations
like the Academy of Consultation-Liaison Psychiatry, the American Psychiatric
Association, and the American Medical Association. I’ve let go of social media
accounts like Doximity and LinkedIn—all of them actually, including Twitter and
Facebook; I just couldn’t get the hang of those.
There’s a National Association of Retired Physicians (NAORP)
that I’ve peeked at. There’s the University of Iowa Retiree Association (UIRA)
that I learned about a couple of years ago when my wife and I attended a
seminar about retiring from the university. I probably won’t join either one.
I’ve been getting invitations from AARP for many years now (who doesn’t?). The tote bags look nice and I am glad that somebody is lobbying for people my age. I haven’t joined so far.
And I joke about my own fictional organization, Retiree On My Own Time (ROMOT). No dues, no meetings, no minutes, no Robert’s Rules of Order. I’m the President, Secretary, Treasurer (Har!), and the only member—for now.
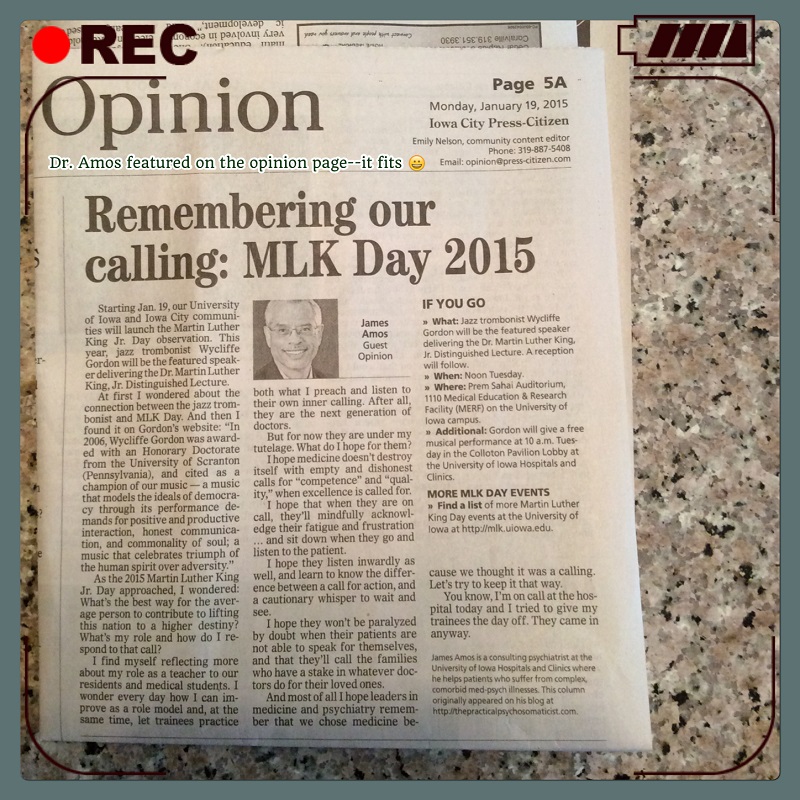
Back when I had the blog The Practical C-L Psychiatrist, I wrote a post about the Martin Luther King Jr. Day observation in 2015. It was published in the Iowa City Press-Citizen on January 19, 2015 under the title “Remembering our calling: MLK Day 2015.”
I have a small legacy as a teacher. As I approach retirement next year, I reflect on that. When I entered medical school, I had no idea what I was in for. I struggled, lost faith–almost quit. I’m glad I didn’t because I’ve been privileged to learn from the next generation of doctors.
“Faith is taking the first step, even when you don’t see the whole staircase.”
Martin Luther King, Jr.
As the 2015 Martin
Luther King Jr. Day approached, I wondered: What’s the best way for the average
person to contribute to lifting this nation to a higher destiny? What’s my role
and how do I respond to that call?
I find myself
reflecting more about my role as a teacher to our residents and medical
students. I wonder every day how I can improve as a role model and, at the same
time, let trainees practice both what I preach and listen to their own inner
calling. After all, they are the next generation of doctors.
But for now they are
under my tutelage. What do I hope for them?
I hope medicine doesn’t
destroy itself with empty and dishonest calls for “competence” and “quality,”
when excellence is called for.
I hope that when they
are on call, they’ll mindfully acknowledge their fatigue and frustration…and
sit down when they go and listen to the patient.
I hope they listen
inwardly as well, and learn to know the difference between a call for action,
and a cautionary whisper to wait and see.
I hope they won’t be
paralyzed by doubt when their patients are not able to speak for themselves,
and that they’ll call the families who have a stake in whatever doctors do for
their loved ones.
And most of all I hope
leaders in medicine and psychiatry remember that we chose medicine because we
thought it was a calling. Let’s try to keep it that way.
You know, I’m on call at the hospital today and I tried to give my trainees the day off. They came in anyway.
I suppose you’re wondering why I’ve been saying that my wife has got me this or that item, like the pink dumbbells and whatnot. She also got me an extra yoga mat.
Part of the explanation is that I’ve recently had a birthday, which reminds me of the importance of time in my life–mainly because I have a shrinking supply of it. After all, I’m heading into the sunset of my journey on Earth.
Sunset
Occasionally, I wonder what I ought to be trying to accomplish, if anything.
To achieve great things, two things are needed:
A plan and not quite enough time.
Leonard Bernstein
Bernstein’s quote is encouraging in a way. Hey, I’ve already got half of it–I don’t have enough time. Now all I have to do is achieve some great things.
I could go on the road to promote my idea for a hit song, “Put your hand in the hand of the man with a plan to get a tan, lead a band, roam the land, avoid the bladder scan, zippity do dah shazam.”
All I have to do is come up with lyrics…and a melody…and an agent…and a band…and a voice coach…and some talent.
Now, if I’m going to accomplish something great, it would make sense to keep working on building a more harmonious balance in my everyday life. I’m doing some of that, including regular exercise, mindfulness practice, and healthy eating.
That reminds me, the birthday cake was excellent, especially topped with white chocolate vanilla ice cream.
Every so often, my former mindfulness teacher sends out an email message about the upcoming mindfulness classes. She always includes an inspirational quote, like the one below:
Be a person here. Stand by the river, invoke the owls. Invoke winter, then spring. Let any season that wants to come here make its own call. After that sound goes away, wait.
A slow bubble rises through the earth and begins to include sky, stars, all space, Even the outracing, expanding thought. Come back and hear the little sound again.
Suddenly this dream you are having matches everyone’s dream, and the result is the world. If a different call came there wouldn’t be any world, or you, or the river, or the owls calling.
How you stand here is important. How you listen for the next things to happen. How you breathe.
William Stafford – “Being a Person”
There was also a couple of suggestions for yoga and meditation techniques specifically to help you sleep. I recognized one of them as the body scan. The body scan is one of the first things they teach you in Mindfulness Based Stress Reduction (MBSR).
The body scan invariably put me to sleep, which made me feel like I wasn’t doing it right. Early on in the course, that was not exactly the “goal” of the body scan. Except mindfulness is not exactly a goal-oriented activity.
That’s hard to conceptualize. And so, the other class that is offered to those who make mindfulness practice a regular part of their lives are follow-up groups. It helps reaffirm the regular commitment to practice mindfulness.
I noticed one of the follow-up groups is entitled “Embracing the Paradoxes of Mindfulness.” The description of the course makes the point that mindfulness really isn’t about reaching a goal or achieving great things. It’s about being rather than doing. It’s hard for me to get my head around that after getting into and through medical school, residency, and practicing psychiatry for umpteen years. And now I’m making a transition to retirement.
One of my biggest fears about making and sticking to a mindfulness practice was that I often didn’t think I would have enough time for it. My teacher just advised me that I would simply have to make time.
Maybe I could accept the time I do have left and just be the geezer I am.
Let’s talk about change. I’ve had a couple of brand-new tie
bars (gifts from my wife) in my dresser drawer for a couple of months now. I’d
forgotten them until last night. I used to wear a tie bar many years ago. I’m
discovering that I probably wore it wrong, according to fashion experts who
know a lot about these things.
I never knew you were supposed to wear a tie bar between the
3rd and 4th button of your shirt (counting from the neck). I guess I
always wore it too low. It was always coming loose from the shirt, and that’s
why I quit wearing it for years. It’s long gone. I think I probably just threw
it away, or maybe it got lost in one of our many moves. And I never knew that
the part of the shirt you attach the tie bar to is called a “placket.”
There are different kinds of tie bars. Most of them are made with what resembles an alligator clip. I guess you’re supposed to call that a slide clasp. Another kind of bar is difficult to manage without wrinkling your tie. It’s an awful lot like a cotter pin, but you’re supposed to call it a pinch clasp—I think. I have one of each. Pictures don’t always seem to match up with the names.
Look close to see the tie bar; it’s there. It’s just not in the right spot according to GQ.
I also used to wear bow ties. You don’t need a tie bar for
those. They were very colorful. They’re long gone.
I also used to wear the old-style suspenders and even had
buttons on the inside of my trousers to secure them. They’re long gone, maybe
because I felt insecure without a belt. That was back before I got a
paunch—which is now starting to shrink, probably because I’m exercising daily.
And speaking of daily exercise, my wife got me a pair of 5-pound dumbbells. She says pink was the only color left. Anyway, I began using them this evening. I’m not sure, but I may need some liniment.
I used to wear a heavy pair of wingtip Oxford brogues. Believe it or not I would tramp all over the hospital in those shoes. I still thought they looked sharp, but they also looked dated—kind of like me. I used to keep the old-fashioned cedar shoe trees in them, just to keep the creases out of the instep. They’re long gone. Now I wear lighter shoes. When I exercise, I wear Velcro tennis shoes.
My wife also got me an autographed copy of Dave Barry’s new book, Lessons from Lucy: The Simple Joys of an Old, Happy Dog. I’ve always been partial to his sophisticated humor—classic booger joke style.
However, I think Barry’s new book is more about how he’s changing as he ages. I haven’t had chance to read it yet except just enough from the jacket to suspect that the booger joke style will be there, but there’ll be something beyond that. He’s 70 years old and likely reflecting—about the mechanism of action of booger jokes. I used to have nearly all of his books, but they’re long gone. Just like the tie bar, I lost most of them in the many moves we’ve made.
The point is I’m changing in a lot of little ways. The big change coming up is, of course, retirement. I’m changing from a physician to a retiring physician—a retiring psychiatrist. Not all of the changes are to my liking, either about myself or my path.
“A flower falls even though we love it; and a weed grows even though we do not love it.”
Dogen
Change is not always comfortable. I have not stayed the same across the decades. Some changes have been painful. Others have been so much fun that I wouldn’t mind reliving them. They’re all long gone. We’ll just have to make new ones.
In my off-service time, I discovered that you need to exercise
150 minutes a week or a little over 20 minutes a day. Exercise guidelines come from
the Department of Health and Human Services and the World Health Organization
who are behind this conspiracy, I mean this recommendation.
I’ve adopted this to some extent, at least what I consider reasonable for a geezer in his mid-60s. I even added something for speed and dexterity. The video shows an abbreviated version of my routine as a demo.
I divide up my mindfulness and sitting meditation with the exercise when I’m on service. I do floor yoga and sitting meditation on alternate mornings and exercise in the evening after I get home from work.
You’ll notice I don’t have a fancy exercise machine. My
exercise equipment is simple. I’m an older guy and I’ve got other stuff I need
to spend my money on—health insurance, muscle cream, beef jerky.
I realize my plank is not absolutely the best form, but I’m
working on it.
I would not make this regimen a requirement for membership in a new retirement club I’m considering. I think a good name might be Retiree On My Own Time (ROMOT). There would be no membership dues. You could make your own card, similar to the one I made. Meetings would be optional because many retirees are actually pretty busy, believe it or not.
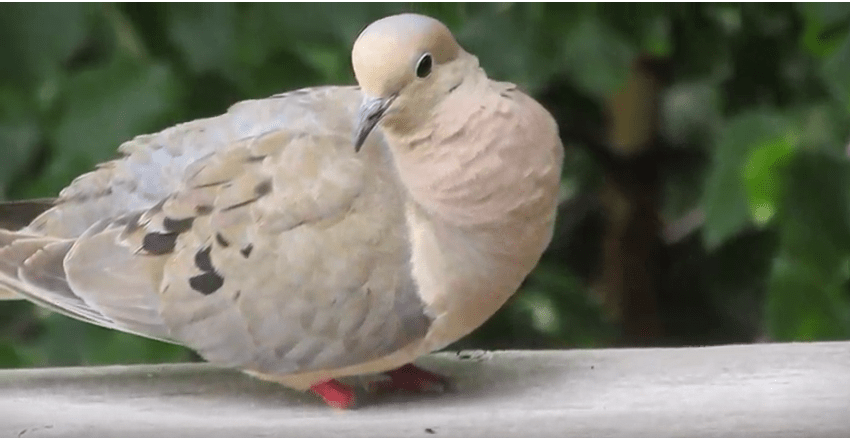
I’m an amateur bird watcher. Last August, I saw a toeless Mourning Dove with what some people would call String Foot, a foot deforming condition that might be caused by a variety of injuries. I had never seen anything like it.
Toeless Mourning Dove
In the slide show you can see a bird seemingly sitting in its own poop, which is said by some to cause the problem—which I suspect is doubtful. The last shot is that of a pair of doves trying to nest in our window box, which was full of sharp, plastic artificial plants. It was painful to watch and I wonder if their hazardous habits could lead to injuring their feet.
Mourning Doves nesting on a speaker
I’ve seen Mourning Doves do strange things, mainly nesting in areas that don’t make much sense. Years ago, we could not dissuade a pair of them from building a home on top of one of the audio speakers mounted outside on our deck. Cranking up the volume didn’t work.
I clicked around the web trying to find out about the problem. Speculation about the causes of these injuries range from something called String Foot (string or human hair used to build nests getting wrapped around toes leading to amputation), sitting in poop leading to infections, and frostbite.
In the book, Birds of
Massachusetts and Other New England States by Edward Howe Forbush, you can
read one of the many anecdotes from amateur ornithologists about bird behavior
that Forbush collected for his book, which was published circa 1929 (I actually
plucked it from one of E.B. White’s essays):
“Mrs. Olive Thorne Miller. Reported case of female
tufted titmouse stealing hair from gentleman in Ohio for use in nest building.
Bird lit on gentleman’s head, seized a beakful, braced itself, jerked lock out,
flew away, came back for more. Gentleman a bird lover, consented to give hair
again. No date.”– Forbush, Edward Howe, 1858-1929. Birds of Massachusetts And Other New England States. [Norwood,
Mass.: Printed by Berwick and Smith Company], 192529.
I wonder why a bird would risk String Foot by using hair in
nests?