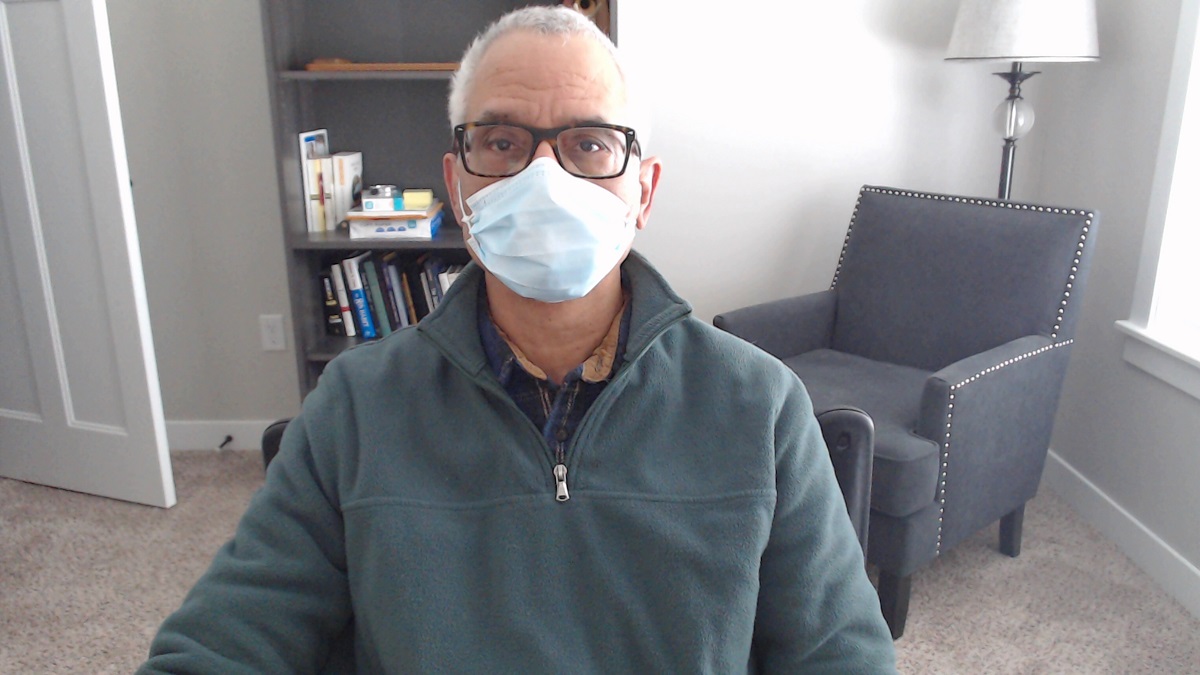
I saw the video the CDC suggested for getting a closer fit using a surgical mask. I had a tough time following how to tie the knot in the loops. Either the demonstrator went too fast or I was too slow (probably the latter.) I found a couple of videos on slip knots and crochet knots (another name for slip knot, evidently). There are probably dozens of YouTubes on how to do the Knot and Tuck.
Since the toughest part of the Knot and Tuck method is tying and adjusting the knot to hug the edge of the mask as closely as possible, I practiced a little. See what you think of the slip knot and tuck in my YouTube video below. Using a slip knot allows you to easily move the knot closer to the side of the mask, allowing a tighter fit. Tucking also helps. It also helps prevent my glasses from fogging up. It’ll never be perfect but it’s better than letting the sides flop open.
Here’s a recently published YouTube by University of Iowa Health Care on the Covid-19 virus, the Omicron variant, and vaccines (actually there are two, see update below). Points that grabbed our attention were:
Omicron is more transmissible, but overall seems to cause less severe disease.
Current vaccines, especially with the booster, protect against getting severe disease, although may not protect against infection.
It’s not a great idea to just get it over with by getting infected with Omicron. Getting the disease can lead to severe medical complications (including myocarditis) leading to hospital admission. The vaccines rarely cause myocarditis as a side effect and it generally resolves without treatment.
Vaccines make getting Covid-19 long haul syndrome less likely.
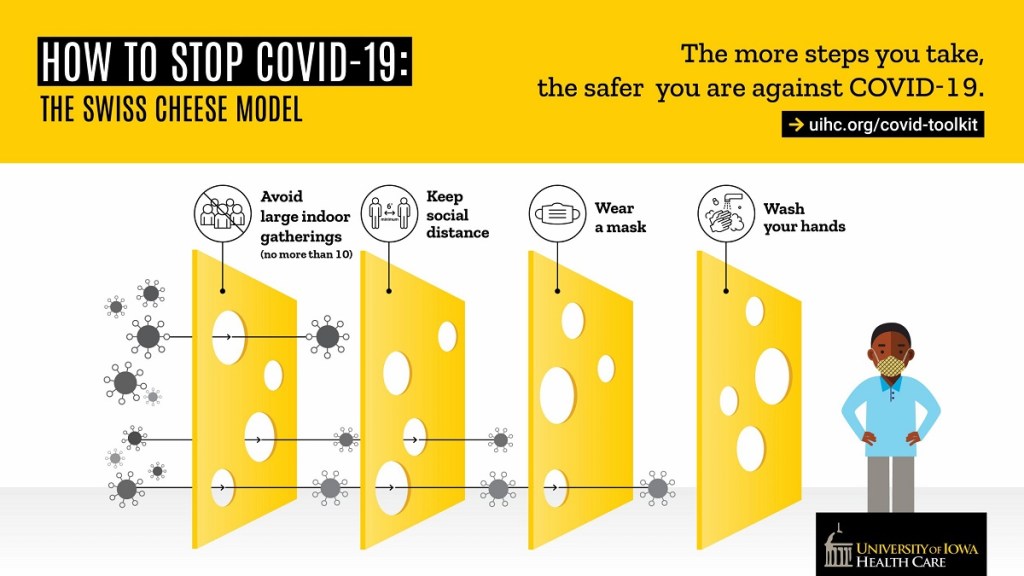
Avoiding getting together in groups of 10 or larger decreases the risk of infection with Omicron. The Swiss Cheese method of protecting yourself against Covid-19 still works best:
Include a slice getting the vaccine with booster: image credit Univ Iowa Health Care
There are medical treatments for Covid-19 disease if you get infected and have to be hospitalized. The treatments are not without side effects. One of them is dexamethasone, a corticosteroid. It can be used to reduce the immune system reaction that Covid-19 infection can eventually cause. Corticosteroids can cause neuropsychiatric side effects that can range from anxiety to frank delirium marked by psychosis. Fortunately, the duration of steroid treatment is relatively short. Vaccines don’t cause side effects of this type. Over the course of my career before I retired, as a psychiatric consultant in the general hospital, I was not infrequently called to assist in the management of extreme psychiatric side effects from high dose steroids (reference: García CAC, Sánchez EBA, Huerta DH, Gómez-Arnau J. Covid-19 treatment-induced neuropsychiatric adverse effects. Gen Hosp Psychiatry. 2020;67:163-164. doi:10.1016/j.genhosppsych.2020.06.001: quote : “Short course high-dose corticosteroid treatment, as occurs in COVID-19, may cause delirium and changes in mood (with a frequency of up to 52% of patients treated with more than 20 mg a day of prednisone during 3 months) [5], being mania and hypomania more frequently observed than depression.”)
Wearing a mask is protective. Recently the CDC recommended preferring medical grade or surgical masks over cloth masks. The guidance has a link to a YouTube on how to make the 3 layer disposable surgical mask fit closer to the face to provide a more effective barrier (and tends to reduce fogging on eyeglasses). N95 masks may be more widely available soon.
It takes a little practice
The vaccines are very safe and effective. We had minimal side effects, mainly sore arms.
Update: We watched the UIHC Covid-19 Family Forum last night which ran from 6:30-7:30 PM. I just noticed that it was recorded. It’s similar to the presentation above. It also contains helpful slides with graphs. There were great questions from the audience, which the experts answered and which are helpful to all of us. Many thanks to Dr. Dan Diekema, MD and Dr. Patricia Winokur, MD for this outstanding forum.
Today, Dr. Feranmi Okanlami, MD, MS, director of student accessibility and accommodation services at the University of Michigan, delivered the Martin Luther King Jr. Distinguished Lecture: “Disabusing Disabilities.” It was sponsored by the University of Iowa.
I attended Dr. Okanlami’s lecture by Zoom. I noticed he was wearing a handsomely carved wooden bow tie, which I don’t have an image for, but you can order them on Amazon, if you’re interested. I’m not the only attendee who noticed it. I used to wear cloth bow ties when I was a much younger man. I gave up wearing any cloth ties shortly after the Covid-19 pandemic began because, as everyone knows, fabric neckties of any kind generally almost never get laundered and carry all kinds of germs. The wooden bow tie is easily wiped down with sanitizers.
But this post is not about wooden bow ties. It’s about what Dr. Okanlami called “ableism” which naturally brings to mind other terms like “racism.” He showed a few images on his slides which showed another point he expanded on, which is the difference between equality and equity. The quick way for me to explain this is to quote the Milken Institute School of Public Health definition:
“Equality means each individual or group of people is given the same resources or opportunities. Equity recognizes that each person has different circumstances and allocates the exact resources and opportunities needed to reach an equal outcome.” — MPH@GW, the George Washington University online Master of Public Health program.
Dr. Okanlami impressed me in many ways, but one of them is his ability to give unrehearsed presentations. He hates to “give talks” as he put it, but likes to talk.
I should explain the reason for this post’s featured image, which might seem puzzling. It’s a photo of the curb ramp connected to the sidewalk outside our home. The city requires homeowners to clear the snow from curb ramps, which, ironically, the city plows plug with snow after every snowstorm. These used to be called “handicap ramps.” I suspect Dr. Okanlami would object to the use of this label and in general it’s probably insulting, but that is what they were called for years. They are an accommodation for those who use wheelchairs.
The word accommodation can have a negative connotation, which Dr. Okanlami clarified. Many believe accommodations give an “unfair” advantage to some people. Actually, they provide opportunities for those with a different set of abilities or altered abilities to participate in society in ways that allow them to contribute to society, and even change it—sometimes in major ways.
Our curb ramp is interesting. The short length of sidewalk beyond it leads to a pile of construction rubble because there is no sidewalk extending beyond our property line on that side. I call it the sidewalk to nowhere, which is now a misnomer. There is a new subdivision under development leading north of our neighborhood. There are houses being built and many have moved in. But for now, you have to walk in the street, which is often muddy and blocked. It’s difficult to walk through it because of heavy equipment and trucks parked along the street. But that doesn’t stop people from walking there. I have never seen anyone in a wheelchair attempt to use the curb ramp. But many people use it who don’t have a visible disability. But it’s there if someone needs it, and we keep it clear of snow on principle.
Dr. Okanlami mentioned those with invisible disabilities. There was not enough time to discuss this in detail, but they include those with mental health challenges. As a consulting psychiatrist working in the general hospital, I saw many of them. They deserve a seat at the table, too.
And I remember one of my medical school classmates who did need to use a wheelchair. There was a special ramp made for him that allowed him to participate in gross anatomy class. Dr. Lance Goetz, MD, graduated with our class and has been a practicing physiatrist in Richmond, Virginia for the last 21 years.
Although Dr. Okanlami’s lecture was recorded today and will, I hope, soon be available for public view, I’m including a YouTube recording of a presentation he gave in 2018 which has the same title and very similar content as the talk he delivered today.
I think his talk evolves every time he gives it. The environment in 2018 was very different than it is now because there was no pandemic and there was a live audience which interacts in a very different way than Zoom allows. That said, the slides were essentially the same today on equity and equality, as were his essential points. He shared a lot about himself in 2018, maybe a little less today mainly because of time constraints and the difficulties inherent to virtual lectures. But he has a great sense of humor.
And he does wear very handsomely carved wooden bow ties.
It’s a mystery why our Chicago Cribbage Antics video is not getting thousands of views on YouTube. It ranks right up there with the other Top 10 great mysteries:
Bigfoot sightings are everywhere, including your backyard; yet there is a shortage of Bigfoot Personal Trainers.
UFOs sightings are also on the rise, and they frequently crash; yet we don’t see UFO body shop repair businesses springing up at all.
How come there is no Save the Chupacabra Society?
What’s the delay on opening the Loch Ness Monster petting station?
Is there any explanation for the pitifully small number of Taco Bell restaurants on Mars?
Will there be an upcoming investigation into why the male Weather Channel meteorologists are required to wear pants that pool around the ankles?
Everywhere you look there is a crisis of men’s shirt pocket puckering—yet there is no federal investigation forthcoming.
Just who is in charge of installing signs to properly identify dangerous worm hole vortex entrances?
Will we ever get anything but lame excuses for the existence of isosceles triangles?
Why does shredded coconut have the texture of cellophane, making it impossible to swallow for some people, like me?
Anyway, as far as we know, there is no other video about Chicago Cribbage besides ours. It deserves around 3 million views, preferably by tomorrow. We appreciate your kind attention to this matter; thank you for your time.
Sena and I thought today’s Zoom presentation “Racial Perspectives on the Institution of Medicine” by Director and Chair of Emergency Medicine Jenice Baker, MD, from Chestnut Hill Hospital in Philadelphia was fascinating. It was an early feature of Martin Luther King Jr. Celebration of Human Rights week. This presentation stimulated a long discussion between us. The theme of this year’s MLK week is “Whatever Affects One Directly, Affects All Indirectly.”
Dr. Baker cautioned that some of the content of her talk would make us feel uncomfortable about the issue of racism in the social realm of our society extending to the medical realm as well. Sena and I were a little surprised about some of the historical facts, such as that white patients always had to be treated first before black people in emergency rooms, regardless of the severity and urgency of the trauma.
This led me to look up the term “implicit bias.” It doesn’t always denote racism per se. It does mean that we’re all prone to making broad generalizations. This accentuates the conflict between political parties, races, and other groups. People on both sides of the color line can overgeneralize, leading to stereotyping.
I told the following anecdote in a blog post from last year’s MLK Human Rights Week:
When I was a first-year resident on rotation in the inpatient psychiatric wards, one of the patients assigned to me roared at me “I don’t want no nigger doctor!” more than once. I discussed the issue with my supervisor. It was a difficult conversation. It was a long time ago and I recall mostly the sense that we both felt awkward. I asked that the patient, who clearly didn’t want anything to do with me, be transferred to the care of another resident. I don’t recall whether he offered to talk with the patient and he deferred on asking another trainee to take over the patient’s care. My recollection is dim about how I handled it. I suspect that’s because it was emotionally painful. Although I had to see him prior to rounds every day, I think I excused myself as soon as he spat the word “nigger” in my face—which was practically every day. I told him I didn’t’ have to tolerate that.
The flip side of this is a conversation I overheard in the distant past between my father (a black man) and his friend (also black, who I’ll call Mark). My father took Mark in, who had just been released from jail and was homeless. He was wearing poorly fitting clothes he probably found because he was penniless and jobless. While he paced the living room floor, he cursed and said angrily, “Man, I will never let this white man do this to me again.” My father just snorted in a way that made me think he didn’t believe that Mark was in his predicament because of any white man—it was probably Mark’s own bad decisions that led to his problems.
As in past years when Sena and I are intellectually stimulated by MLK Celebration of Human Rights week speeches, our discussions get long and spirited and tend to range widely over the spectrum and durability of human weakness, human evil, and the seemingly accidental nature of human wisdom and human kindness.
We talked at length about James Alan McPherson, long time Iowa City resident and nationally renowned writer, the first African American to win the Pulitzer Prize for short fiction, and acting director of the Iowa City Writers Workshop. He died in in the summer of 2016. An Iowa City neighborhood park was recently renamed James Alan McPherson Park in his honor.
But judging from news stories, this didn’t happen until members of the Iowa Freedom Riders suggested that a park be named “Black Lives Matter Park” in the summer of 2020. In response, more than a dozen people recommended that Creekside Park be renamed in McPherson’s honor instead.
Was the suggestion of renaming the park after McPherson simply a maneuver to avoid naming a park after BLM—and possibly to avoid extremist consequences? Why did it take Iowa City so long to honor him after he died? It is puzzling given that his peers called him the heart and soul of the Iowa Writers Workshop and given that McPherson himself called Iowa a place where he felt welcome. He was even in psychotherapy delivered by a white psychiatrist, Dr. Dorothy “Jean” Arnold, the first female psychiatrist to open a private practice in the state of Iowa in 1957. They were both from the racially polarized South. I wonder how they ever connected.
Why should this matter so much to us? Just like Dr. Baker’s presentation, it’s a very uncomfortable discussion. Sena is very good at doing what MLK suggested in his Letter from a Birmingham Jail, where the quote “Whatever Affects One Directly, Affects All Indirectly” comes from—creating “constructive nonviolent tension.” King always advised against violence or anything other than nonviolent methods of protest, saying that what we need is to create a type of constructive nonviolent tension, which he proved can be more effective than violent confrontation.
Some extremists say that King’s nonviolent approach is no longer relevant for our times, but I doubt violence is the answer. Somehow all of us need to learn how to not just tolerate an atmosphere charged with constructive nonviolent tension—but to somehow transform ourselves directly and thereby transform others indirectly into peaceful agents of change.
The 2022 Martin Luther King Jr. Celebration of Human Rights Week gets kicked off on January 12, 2022 with Chair of Emergency Medicine Jenice Baker, MD, from Chestnut Hill Hospital in Philadelphia giving a lecture via Zoom, “Racial Perspectives on the Institution of Medicine.”
And on Wednesday January 19, 2022, Dr. Feranmi Okanlami, MD, MS, director of student accessibility and accommodation services at the University of Michigan, will deliver the Martin Luther King Jr. Distinguished Lecture: “Disabusing Disabilities.” You can register on line for this lecture and see the following link for a full list of events which will be updated.
I just found out today that my blog’s theme was retired. I don’t know when WordPress retired it, but it gives me a familiar feeling about retirement. Sena gets the credit for giving me the idea of changing the theme (which is how my blog looks on the web) because of the new year. As I looked over the themes, I saw a tiny notice beside the name of my own. “Your blog theme has been retired. Consider getting a new one, you geezer!”
The notice didn’t really say that, of course, but that’s how I felt. I’ve been blogging since 2011. I’ve never had a theme that was retired. I realized that if I changed my theme now, I couldn’t go back to the old, familiar creaky, cob-webbed, old-fashioned theme I’ve had now with my second blog. This one has the theme (using the word in a different sense) of—retirement. In fact, come to think of it, the word “old-fashioned” was used in the WordPress article explaining why some themes get retired.
So, I started looking at the themes seriously today. Most of them had the word “minimalist” attached to them. Frequently, I read how great they were for my “business.”
Hey, I’m retired. I’m not in any kind of business. There seems to be a lack of emphasis on a theme for hobby bloggers, some of whom are retired geezers.
Anyway, I dropped my old-fashioned theme and put on a new one. While I was at it, I got rid of a lot of old widgets. WordPress calls them “Legacy Widgets.” I couldn’t find a clear explanation for why they call them that. I did find a definition on the web. Essentially, in this context, I think it denotes software that has been superseded but is difficult to replace because of its wide use. What’s wrong with sliders? I don’t mean little sandwiches. I mean the featured images with post titles that slide across the theme page, showing off my best posts—or at least what I think my best posts were. Really, no themes with sliders? That’s what minimalism leads to, I guess.
I’m a legacy consulting psychiatrist, meaning I’m retired—something else to feel ambivalent about. Anyway, I kind of like the new theme.
There’s this line by Agent J in Men in Black 3 that goes: “Okay, see, the prerequisite for a joke, is that it be funny.” That’s what the “you really had to be there” expression is about and which occurs to me whenever I think about an incident that cracks me up now almost as much as it did decades ago.
The thing about the “you really had to be there” expression is that it refers to an event that was funny to someone, but the comicality of it is usually tough to explain to a person who wasn’t there at the time the event occurred. It’s one of those insider jokes. The often-present feature of the story is that there are some parts of it you’d rather not reveal. That can make it hard for some people to “get it.”
This “you really had to be there” story happened when I was a teenager. A bunch of us guys were sitting around a table after finishing lunch. We were having dessert, which were crumbly snack bars. I think they were made of chocolate Rice Krispies and they were probably old. That’s a key factor, along with the paper plates on which they were served.
Some of the guys were jonesing for a cigarette. Not me because I didn’t smoke. But the place didn’t allow smoking. One guy (I can’t remember his name so I’ll call him Ralph) started complaining about it and then starting playing with his snack bar like it was a cigarette. I know Rice Krispies bars are usually gooey, but these were definitely not. They were dry and tasteless. When you picked them up, crumbs randomly dropped all over the paper plates.
Anyway, while Ralph was moaning and groaning about not being able to smoke, he started tapping on his dessert bar like he was tapping ashes off a cigarette. Now, if you’ve ever smoked or watched somebody else smoke, it eventually dawns on you why some people say they smoke—it gives them something to do with their hands. Anyway, people used to say that. They do all sorts of weird mannerisms and trick-like finger moves while they smoke.
Anyway, Ralph would roll his cigarette/snack bar on the paper plate, tap crumbs off it like they were ashes, flick it smartly and, occasionally, he’d put it up to his lips and take a bite as though he were taking a drag.
Cigarette ash doesn’t make a sound when it falls in an ashtray. It’s impossible to explain why the tapping noise of the snack bar crumbs hitting the paper plate made us all hysterical. But it definitely had a lot to do with his clowning around with a snack bar prop. Ralph’s act was a combination of complaints about the food, the smoke-free joint, and an instinct for the prerequisite of a joke. It was funny—at a particular time and in a particular place.
I’ve thought about trying to make a YouTube video of this. But I don’t think it would be as funny as Ralph’s spontaneous performance. There’s probably no way I could pull it off. And, let’s face it, as a trained doctor knowing what I know about the health hazards of smoking, it’d be pretty awkward.
And would anyone else get it? You really had to be there.
It’s been a quiet day around here. It’s New Year’s Eve. I got a great message from a former resident who has started his own Psychiatry Consultation Fellowship training program in Bangkok, Thailand. Dr. Paul Thisayakorn and his wife are welcoming 2022 with their 2 lovely children and hoping 2022 will be a better year, as we are. The Covid pandemic has been hard around the world.
Paul also looks forward to establishing a C-L Psychiatry academic society in Thailand in the coming year. Paul did his psychiatry residency at University of Iowa and his C-L Psychiatry fellowship in Cleveland. Sena and I wish him and his family all the best in the new year.
Today was quiet, but tomorrow the big snowstorm will come. We’ll be digging out all day because the forecast is for 5-8 inches, high wind gusts, and ice. It’s Iowa, after all.
But for tonight we’ll take a cup of kindness and say goodbye to 2021.
And if you like MacLean’s version of Auld Lang Syne above, you might have a listen to another with the Scottish lyrics translated.
This is just a short message wishing a safe and happy holiday to all. I’m passing readers a couple of links to update information on the Covid-19 Omicron variant and how to stay as safe as possible this winter.
First is the Rounding@Iowa link to the Omicron Variant update. It’s an interview with University of Iowa Hospitals & Clinics (UIHC) infectious disease expert, Dr. Patricia Winokur, MD. It’s about a 16 minute interview. Highlights are that it’s important to get the booster for solid protection against variants including Omicron and that the Covid-19 vaccine is, in general, likely to turn out to be a 3-shot vaccine similar to others, such as the Hepatitis and Shingles vaccines.
The other link is to UIHC infectious disease specialist Dr. Daniel Diekema, MD and his thoughts about the Omicron variant. They echo those of Dr. Winokur and the emphasis again is on the importance of getting vaccinated.
Lastly, there is some guidance by UIHC in a graphic below on how to stay safe from getting infected with Covid-19, (whatever the variant) during winter activities. Happy Holidays!