I just saw a great post on Fear of Missing Out (FOMO) on Bob Lowry’s blog, Satisfying Retirement. The link is on my home page and it’s a great read, along with many of his other posts.
FOMO for me is different because I’m not actually retired
yet. Bob has been retired for a long time and knows what he’s talking about. I’m
still just trying to get used to the idea of being retired for now.
Even though I’ve been in phased retirement for over two
years now and this coming year is my last before full retirement (see my
countdown!), I’m still coping with FOMO.
I check my email several times a day, even when I’m not on
service. My position will likely be filled with my replacement well before the
year is out. Occasionally I’ll find a trainee evaluation that is time sensitive
that I have to complete. I updated the guide to the psychiatry consultation
service and notified others about that just yesterday.
What am I going to do when I’m retired? That’s what so many ask me and which I sometimes ask myself. I’m actually having a pretty good time now that I’m finally adjusting to phased retirement. According to the 2018 Report on U.S. Physicians’ Financial Preparedness: Retired Physicians Segment, one suggestion is that physicians try to retire gradually rather than abruptly.
I agree with that and the phased retirement program I’m in has
felt right for me. It hasn’t stopped me from FOMO so far, but I’m gradually
getting more and more enjoyment from doing things that are not work-related—even
though FOMO makes me check my email and the electronic medical record every
day.
My wife and I started saving very early on in my medical training and we were fortunate enough to eliminate educational debt early. We’ve always lived simply and don’t need a lot of expensive toys.
Feed me!
I find ways to build a schedule into my day. I exercise and meditate.
Exercise daily and you can look like me!
Meditating makes my head radiate like this.
I’m not much for yard work, but I try. I get a big kick out of hobbies I’ve rediscovered such as bird-watching.
I’m not a yard kind of guy…
Tree Swallow peeking
I like to make silly videos as some of my medical students have noticed. One of them learned how to fold a fitted sheet from one of my YouTube videos. I really enjoy blogging and combining that with my mostly short YouTube movies. You’ll notice I do have some work-related videos, though, some of them fairly recent.
Hey, here’s how to fold a fitted sheet!
The featured image for this post was actually partly a
creation of one the residents a few years ago, who by some miracle found a way
to combine my photo with a picture of a smartphone. I added a little more to it
to make the point about FOMO.
My FOMO nightmare, once upon a time.
I actually didn’t have a smartphone until about 4 years ago. And I still mainly use it just as a phone. I check the step counter when I’m staffing the psychiatry consultation service, but I’ll quit doing that.
In fact, the residents persuaded me to get a smartphone. I had a flip phone for a few years prior to that mainly because a snowstorm caught my wife out on the road while she was driving to the hospital to pick me up from work. I had no way of knowing where she was and was worried out of my mind. That convinced me we needed more than land lines.
I may go back to the flip phone after I fully retire.
I still use a desk phone at work. For the first time in my career, last weekend it just quit working. You can’t imagine how happy I was.
What?
You gotta be kidding!
You’re not kidding…
Whenever I drop my pager, I always say out loud to the trainees, “Oh my gosh, I hope it’s broken!” I’m only half-joking.
I won’t miss pagers when I retire.
I dropped most of my social media accounts over a year ago, including Facebook, LinkedIn, Twitter, and even Doximity believe it or not. I don’t miss them.
I’ll keep you posted on how my struggle with FOMO goes.
The featured image for this post is that of a Painted Lady
butterfly, one beautiful member of a hugely diverse group of such creatures. It
reminded me of the state of our physician supply, which is not so very diverse
when it comes to inclusion of minorities.
Even though I’m moving into the final year of my phased
retirement contract in July and I’m off service—I still check my office email several
times every single day. It’s a hard habit to break after 23 years, not counting
4 years each of residency and medical school. So, I get a pang every time I see
a news item in my inbox about the shortage of physicians, especially the
shortage of minority physicians. The challenge to increase diversity of race
and ethnicity in the supply of American doctors is a big one.
The Greenville News in South Carolina posted a long article about this issue on May 13, 2019 (“Despite efforts to boost their numbers, blacks account for just 6% of doctors in SC” by Liv Osby). Even though blacks make up 13% of the U.S. population, only about 6% of the doctors in Greenville, S.C. are black. Many members of minority groups do not recall seeing a doctor who looked like them while they were growing up. Minority role models for the goal of becoming physicians have always been few and far-between.
I recall being one of a handful of minority students entering
the summer enrichment program in 1988 at the University of Iowa. The summer
enrichment opportunity was intended to be one way to assist minority students
excel in the basic sciences courses that we would be facing in the upcoming regular
academic year.
I have always appreciated that boost but not all of my peers
saw it that way. One young man said simply, “I’ll see you in the fall,” evidently
meaning he would not be attending the summer enrichment program. It was clear
from talking with him that he thought the program sent the wrong message to the
majority students—that we were getting an unfair advantage. I’m pretty sure
that the summer enrichment program ended many years ago, at least in part
because of that negative perception.
This reminded me of my undergraduate experience at
Huston-Tillotson (H-T) College (now H-T University) when the controversy about affirmative
action was prominent. I recall only one black student who was planning to go to
medical school and hoped to get into the University of Texas. In fact, even
though the term is no longer used, the Greenville News story mentioned that
Texas Tech last year eliminated race as a consideration for admission to its
Health Sciences Center. This indicates ongoing discomfort about the perception
of favoritism or special treatment being given to minorities.
I still see one of my summer enrichment program professors
in the hospital hallways every so often. He even remembers my name. We exchange
friendly greetings.
And I’m painfully aware that there may be only one other
black psychiatrist in Iowa—and I think he’s also a baby boomer.
As I head for retirement, I remember a line from one of the final scenes in the movie Men in Black, “I haven’t been training a partner; I’ve been training a replacement.” I’m not sure if there will be someone to replace me.
Today I want to thank everyone in my department for nominating me for the Excellence in Clinical Coaching Award . I accepted it during the Graduate Medical Education Leadership Symposium this afternoon.
For some reason, I almost wrote “Excellence in Clinical Clowning Award ” above. I guess maybe one of the reasons is that I was given an award (tongue in cheek) by the residents a few years ago when I made a pretty funny mistake giving a Grand Rounds presentation.
Much to my embarrassment, I somehow mixed up my slides so badly that many of them were out of order. I had to ad lib around that–a lot. Little wonder the residents whipped up the Improviser of the Year Award for outstanding improvisation during a Grand Rounds.
Improviser of the Year Award
Another honor I received about 8 years ago was a Feather in My Cap award after making the rank of Clinical Professor. The awardees had to come up with a favorite quote which guided them, and which was printed on the certificate. At the time, my favorite quote was:
“Vitality shows in not only the ability to persist but the ability to start over.”
F. Scott Gitzgerald
Another feather in my cap
I think I chose that because I have sort of reinvented myself over the years, including going to medical school later in adulthood, trying private practice in psychiatry, and most recently transitioning to retirement.
I’m also very fond of the Leonard Tow Humanism in Medicine Award about twelve years ago.
These days, other quotes are more important to me, like the one by Stephen Covey,
“Leadership is a choice, not a position.”
Stephen Covey
The comments praising today’s honorees, written in the the program by trainees and department colleagues, were heart warming for everyone. They brought back memories for all of us, I’m sure.
I struck up a conversation with an attendee about comparing coaches and mentors. I mentioned that in a previous post, “Spring,” on May 4, 2019. Many people tend to conflate the two roles, although I still favor the view that coaches tend to have shorter relationships that are more focused on skill building while mentors have longer term relationship more focused on career building.
However, both mentors and coaches serve as role models, something all teachers do. I have a short coaching video below for a skill I have often role-modeled for trainees–sitting with patients and listening to them for understanding.
In honor of Excellence in Clinical Coaching–and Clowning.
I’m also a big fan of a sense of humor on the Consultation-Liaison Psychiatry service, as anyone knows who has worked with me. My work-related anecdotes get more colorful, less accurate, and longer the older I get. I know when to cut them short, though–the trainees snore loudly. My hearing is still pretty good. I briefly considered getting a coach’s whistle—but thought better of it.
Dr. Amos, clowning again–and thanks for all the produce!
I get a big kick of this video every time I see it. It’s a
YouTube about people who are 100 years old who are funny, wise, and talented. It’s
included on the SSM Health St. Mary’s Hospital YouTube channel. St. Mary’s
Hospital is in Madison, Wisconsin. I worked as a psychiatrist there very
briefly a long time ago.
However, the other thing this video brings to mind is
something sad. I see patients half my age (nowhere near 100) almost every day
in the hospital who are delirious, sometimes for prolonged periods of time.
According to the medical literature, they will be at risk for developing
dementia and not infrequently do. In fact, research tends to show that for
every day someone spends delirious, the risk for developing dementia goes up
35%. That makes delirium a life-limiting condition which can happen to anyone
at any age.
I got delirious after a routine colonoscopy, a procedure to
screen for colon cancer and other pre-cancerous tumors that used to be
routinely recommended for those who reach 50. It was the worst 50th birthday
present a guy could ever get.
I was delirious probably because I got sedated with a
combination of Versed and Demerol. The worst part of the condition probably
lasted only a couple of hours at most following the procedure. But I was sure
wiped out the rest of the day.
I would have a tough time picking out the worst part of the
whole process, the bowel prep (guzzling a big jug of GoLytely which should be
called GoHeavily) or enduring the post-procedure delirium. It was probably the
latter.
I don’t remember much. My wife tells me that I kept
repeating something about not taking NSAIDs. I think there was something about
that in the informed consent and education materials that got sort of stuck in
one of my neurons. I kept sliding down in bed while I was in the recovery room,
which I was in for a little while longer than is usually expected.
Preventing delirium is a vital job for health care
professionals everywhere. We can’t prevent each and every case, but there are
definitely things we can do to mitigate the problem. One of the most important
goals is to try to minimize or avoid the use of certain offending drugs such as
anticholinergic and sedative-hypnotic agents.
It’s also good to remember that the population at highest
risk for getting delirious is the elderly and those who already may have
cognitive impairment.
Preventing delirium, based on current literature, means first implementing non-pharmacologic multicomponent interventions. These may require a large cadre of volunteers. The best example is the Hospital Elder Life Program (HELP) at Yale, which is copyrighted by Dr. Sharon Inouye. Six of the most important features to address:
–Normalizing electrolytes such as sodium and keeping
patients well-hydrated
–Mobilizing patients as much as possible, including getting
immobilizing devices such as foley catheters removed as early as you can
–Making sure sensory aids such as eyeglasses and hearing
aids are available
–Ensuring that medications are monitored so as to minimize exposure to drugs that are anticholinergic or sedating.
Anyway, working on preventing delirium and minimizing its
impact is an ongoing challenge. Keep the goal in mind: We want as many people
as possible to live well to 100.
Last year, we noticed a groundhog waking up and bulldozing
our back yard, even though snow was forecast that day. It’s pretty good at just
putting its head down and pushing through almost anything in its path including
leaves, sticks, small rocks, flowers, and so on.
Their single-minded digging has helped uncover bones and
pottery of old civilizations and aided medical researchers study a lot of
things including the role of viral hepatitis in liver cancer.
I can compare them to those who bury themselves in the
single-minded study of medicine in the transformative path to medical practice.
I can recall my medical school classmates and their clicker pens taking notes
in class. They weren’t called “gunners” for nothing. Call it the Groundhog
Effect.
Even if you weren’t a gunner, you had to apply yourself just
like a groundhog to your studies. It could lead to another characteristic
common among these creatures. They tend to be loners.
The analogy is far from perfect, of course. Groundhogs
aren’t lonely. People can be, which is why medical students and residents are
often advised to always remember H.A.L.T.
H.A.L.T. refers to trying to avoid letting oneself get too
hungry, angry, lonely, or tired. It’s probably a warning about incipient
burnout, a problem that affects at least half of physicians and which is the
hot topic these days.
I’m always a little puzzled that so many physician wellness
programs and meetings seem to devote a lot of time trying to teach doctors how
to improve their resilience. It’s as though we’re somehow to blame for getting
burned out.
I’m not saying learning things like mindfulness are not
important for promoting physician wellness. I have my own daily mindfulness
practice and it is certainly helpful.
It would also be nice to spend more time addressing the
systems issues contributing to physician burnout, such as very full clinic
schedules, overly complicated electronic health records requiring hours of data
input that create the need for “pajama time,” which is bringing your job home
with you, board certification busywork, managed care rules that marginalize
physicians, and so on.
This is a continuation of the hassle factors that can lead
to physicians just learning to put their heads down and dig through the
mess—sort of like the groundhog, and often in isolation from each other.
Transformative processes can also occur at the end of a
physician’s career. I’ve spent a long time learning to be a physician and now
that I’m in phased retirement, I’m finding out how hard that can be. It would
be helpful to know that others are passing through this stage as well, and that
I’m not alone.
Could it be that one way to counter the Groundhog Effect is
to come together and share this retirement experience? There will always be
those who work well into their nineties and that’s great. Statistically,
though, most of us will retire in our mid-sixties.
The graying out of the psychiatrist population is
contributing to the shortage, to be sure. But we could still be useful to the
next generation of doctors acting as role models for how to navigate the other
transformative process—reflecting on the task of becoming somebody other than a
physician. I think it would be easier if several doctors did this.
Animals do this. I saw this several years ago when we owned
a house with a fountain, which was frequented by more than a couple of species
of birds, including Bluebirds. They gradually arrived but were at first
tentative about immediately diving in. One would perch on the rim. Another
would come along and do the same, maybe drink a little water while watching the
other.
Eventually, one would dip its tail feathers in just for a
moment. Pretty soon, they would make like ducks.
I guess you could call it the Bathing Bluebird Effect.
The article is about how Black psychiatrists have struggled
to become a part of mainstream psychiatry, eventually forming the separate
organization Black Psychiatrists of America (BPA) in 1969.
Nowadays it’s difficult to imagine that the American Psychiatric Association (APA) discriminated against Blacks. As an aside, I’m noticing how I’m not using the usual term “African American” in this post. Instead, I’m using the term “Black,” which is what Dr. Griffith did.
This reminds me of a book review I wrote for the American Journal of Psychiatry almost 20 years ago (Amos, J. (2000). Being Black in America Today: A multi perspective review of the problem. Am J Psychiatry, 157(5), 845-846.).
The book was written by Norman Q Brill, M.D. It reminded me
of my experience at Huston-Tillotson College (now Huston-Tillotson University,
a private school, historically with largely Black enrollment) in Austin, Texas
back in the 1970s. I wrote:
“Dr. Brill’s appraisal of many black leaders in chapters
such as “Black Leaders in the Black Movement” and “Black Anti-Semitism” may be
refreshingly frank in the opinion of some. He tailors his prose so as not to
denounce openly those whom many would describe as demagogues. At the same time,
it is apparent that his underlying message is that a substantial number of them
are not only out of touch with mainstream black America but may even mislead
black people into adopting ideological positions that impede rather than foster
progress. Dr. Brill’s description of the issue reminded me of my own experience
with this phenomenon as a freshman in the mid-1970s at a college of
predominantly black enrollment in the southern United States. A guest lecturer
(who, as I recall, had also written a book about being black in America) told
us that the white man would never allow a black man to be a man in America. He
had only three choices: he could be a clown, an athlete, or a noble savage.
These corresponded to the prominent and often stereotyped roles that blacks
typically held in entertainment, sports, and black churches.”
I was taken aback by the speaker’s judgment and asked him what my choice should then be. He was equally taken aback, I suspect. He advised me to be a clown. I also remember being aware of why my department asked me to write the review. That leads me to reflect on the upcoming celebration of the 100 Year Anniversary of the Department of Psychiatry where I’ve been a faculty member. It’s in November 2019.
If you read through the web page describing the history of the department, you won’t find anything about Black psychiatrists. In fact, I could be the only Black psychiatrist who has ever been a faculty member here at The University of Iowa Hospitals and Clinics.
And if you look at The 2018 Greater Iowa African American Resource Guide available on the web, you’ll find only one other psychiatrist listed other than me. See Update below about this reference:
Update: I’ve discovered as of May 3, 2022 that the 2018 Greater Iowa African American Resource Guide cannot be found at the link above. There is a link to The 2019 Greater Iowa African American Resource Guide. I’m still listed as the only Black psychiatrist in Iowa City. There was a Black psychiatrist in Sioux City who was in the 2019 guide as well, Dr. Rodney J. Dean, MD at Dr Dean & Associates. I could not find any guides after 2019.
On the other hand, historically, some Blacks have done well in Iowa. George Washington Carver became a faculty member at Iowa State University in the 1890s. I graduated from Iowa State in the 1980s. After World War II, Black Iowans integrated The University of Iowa, Iowa State University, and Drake dormitories in 1946. Dr. Philip Hubbard was the University of Iowa’s first Black vice president.
I am not a clown, an athlete, or a noble savage. I am a man.
Addendum: I read the facts about George Washington Carver
and Dr. Philip Hubbard on an Iowa Public TV web page. However, to my dismay the
site is marked “Not secure” by Google. The source of the information there is
from a respectable reference:
Silag, B. (2001). Outside in: African-American
history in Iowa, 1838-2000. Des Moines: State Historical Society of Iowa.
Content information:
“A distinguished group of 36 writers (for no pay or
royalties), including community leaders as well as academic historians, has
created Outside In: African-American History in Iowa, 1838-2000, a book certain
to become the standard work on the African-American experience in Iowa. Each of
the book’s 20 chapters focuses on a particular aspect of that experience–legal
and political rights, business and professional leadership, clubs and community
organizations, churches and schools, and more–from Iowa’s territorial days to
the present. Hundreds of photographs (gathered from family albums and
scrapbooks, as well as historical archives) accompany the text, which is
documented with extensive references. A detailed index is also included. Three
themes tie together the enormous amount of historical information contained in
Outside In: *The struggle of black Iowans to claim their rights as citizens;
*The pursuit of individual opportunity in Iowa’s evolving economy over the
years; and *The creation of community institutions to help families and
individuals through good times and bad. Outside In provides the big picture and
the details of this proud story of African-American initiative in Iowa, from
the groundbreaking legal victories of pioneer Alexander Clark up through the
present day political triumphs of Preston Daniels and LaMetta Wynn.”
–Dust Cover, Front flap. Outside In is the result of a collective effort
spanning five years. It is the first in-depth study of the black experience in
Iowa in a half-century, and is expected to stand as the definitive work in its
field for some time to come. While much of the book’s contents recall hard-fought
struggles against prejudice, discrimination, and violence. Outside In also
points to proud traditions of understanding and cooperation among black and
white Iowans, traditions that go back to before the Civil War and remain vital
to this day. –Dust Cover, Back flap.
I’m coming up on my last 3 days for the academic year and
reflecting now that my favorite season is upon us. Spring does that to me,
especially now that I’ve been in the phased retirement contract for the last 2
years. I’ll be going into the 3rd and final year as of July.
I just found out that next week I’ll be among those faculty members selected to receive the Excellence in Clinical Coaching Award from the Gradual Medical Education Office at the Leadership Symposium.
I’ve received teaching awards from the residents at
graduation time (another sign of spring!) over the years and I’m always grateful
for their recognition. The Excellence in Clinical Coaching Award is recognition
from my department as a whole, the members of which put together a nomination
package including letters from department leaders as well as trainees.
I’m also humbled by
it because I’ve learned a lot from everyone with whom I’ve had the privilege of
working, but my favorites are the trainees, including medical students. In
fact, I learned from them again in the last week or so. Three talented medical
students gave outstanding presentations about issues relevant to all
physicians, not just psychiatrists.
They will be excellent physicians. They will teach others.
They will lead and it’s a good thing—medicine needs them.
I like the coach idea. I know one of the internal medicine residents thought of me as a mentor. I’m aware of the differences between mentors and coaches as well as the similarities.
Coaches spend relatively less time with learners and the
focus of the relationship is usually a set of specific skills which needs to be
passed on. Mentors tend to develop longer term relationships and guide learners
in broader ways in terms of career goals and more.
However, both mentors and coaches serve as role models,
something all teachers do—including trainees.
That’s partly why I feel less troubled about retiring as my
time to leave draws nearer. I trust the next generation of doctors and, just
like the Supremes song says, “You better make way for the young folks.” It’s my
time to leave. It’s their time to live.
I’m back in the saddle again after a brief hiatus according
to the terms of my phased retirement contract. During my time away, I thought
about what a short introduction to Consultation-Liaison (C-L) Psychiatry might
include to give medical students and other trainees a snapshot look at what CL
psychiatrists encounter in their work in a busy general hospital.
As I considered what to include, it occurred to me that
common consult questions typically could be classified into three basic groups:
Manage Crises:
This often involves assessment of medically ill patients for whom there are
concerns about suicide or violence toward others, including health care
professionals.
Manage Medications:
Frequently, I get questions about how to manage psychiatric medications, often
in patients who are being treated with multiple medications; or need
authorization for clozapine (an atypical antipsychotic which usually must be
authorized initially by a psychiatrist); or need adjustment of medications in
the setting of medical problems like cardiac disease or bowel resection (in
which absorption might be affected).
Manage Behavior:
This doesn’t always involve violent behavior but may include challenging and
potentially disruptive acting out in the setting of delirium, or associated
with patients who might have personality disorders or abnormal illness
affirming disorders.
These broad categories make up the biggest share of the concerns my colleagues in general medicine hospitalists and surgery have about a significant proportion of patients in a large hospital.
Short video illustrating the Dirty Dozen in broad overview.
I’m back on my soap box about Maintenance of Certification (MOC) again. Sidney Weissman, M.D. remarked in a letter to the editor of Psychiatric News (April 19, 2019 issue, Vol. 54, No. 8) on the rising numbers of graduating medical students who match in psychiatry residency slots. Many will graduate from these programs into private practice clinics which will emphasize seeing large numbers of patients primarily for medication management. Psychiatric hospitalists like me are uncommon, which tends to decelerate the movement toward integrating medical and psychiatric care and limits the application of psychotherapy which psychiatrists have historically done but which has been replaced by medication management.
While the match
numbers continue to grow in psychiatry, the dissatisfaction with regulatory
pressures from certification boards like the American Board of Psychiatry and
Neurology (ABPN) also continue to frustrate psychiatrists who are compelled to
oppose the Maintenance of Certification (MOC). Indeed, another prominent story
in the psychiatric news is the class action lawsuit against the ABPN filed by
two psychiatrists, alleging that the MOC requirements are illegal and
anticompetitive. See the story in the April issues of Clinical Psychiatry News
and Psychiatric News.
Along with the
increasing numbers of psychiatrists who are retiring (more than 60% of
psychiatrists are over the age of 55), and I interpret the increasing
Psychiatry match numbers with cautious optimism at best.
I have always
advocated for the principle of life-long learning for physicians and opposed
MOC because, in my opinion, it’s a drag on the progress of fulfilling the
principle. The reason is that there is very little evidence supporting the
certification boards’ assertions that MOC makes better physicians.
I have supported the position of Dr. Paul Teirstein, MD, one of the leading physicians spearheading the National Board of Physicians and Surgeons (NBPAS), and I’ve recommended that the University of Iowa Hospitals and Clinics (UIHC) consider accepting NBPAS as an alternative to the American Board of Medical Specialties (ABMS) MOC. Three Iowa hospitals already do so.
I’ve been in phased retirement and expect to be fully retired by 2020. Because of that, I decided not to seek continued certification through either NBPAS or ABMS. I chose not to pay the fee required by the American Board of Psychiatry and Neurology (ABPN) to sit for the recertification examination. Consequently, that resulted in my being identified as “Certified” although “Not Meeting MOC Requirements.” This was data about me as a physician which was readily available to the public and other organizations. I think it’s unfortunate that this practice tends to convey the impression some physicians are less qualified than others based on their certification status alone.
My current listing on the ABPN web site.
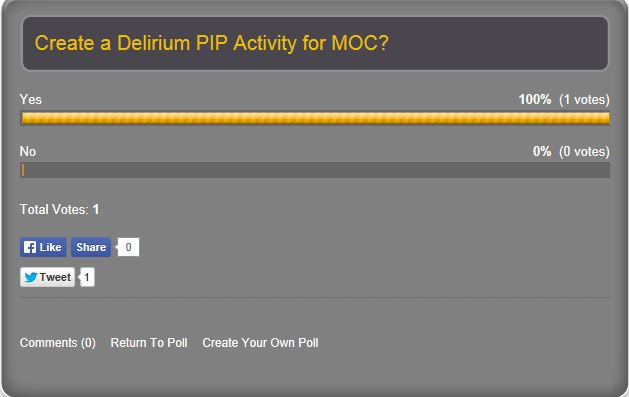
Now I’m listed on the ABPN as “Not Certified” of course. Ironically, my Performance in Practice (PIP) module on delirium, the Delirium Clinical Module is still there. You can find it just by typing the word “delirium” in the search field. In my previous blog, The Practical C-L Psychiatrist, there was virtually no interest in such a module, at least judging from my far from scientific poll about 6 years ago. Yet it’s one of the few modules available on the ABPN website that C-L psychiatrists would welcome.
Low interest in an ABPN MOC Delirium PIP activity in 2013
I’m aware that
declining to sit for what would have been the last MOC recertification
examination in my career might not be viewed as much of a protest, especially
since I’m retiring.
I’m also aware that
many physicians are not in a position to decline participation in MOC. Some
organizations and health insurers demand it, prompting several physicians and
state legislators to collaborate toward adopting or consider adopting laws to
discourage it.
To be fair, MOC is
often not the only criterion that organizations use to ensure patients are
getting the best health care available. And there are many who work diligently
to improve the MOC process and believe it works. Enhancing the motivation for
physicians to participate in MOC is complicated and we need to consider
different practice environments, physician burnout, and financial incentive
programs which have typically attracted few physicians overall.
It’s difficult to
find much information on PubMed about MOC, whether you search using the Most
Recent or the Best Match filter. In both, I found a paper by a doctor which
appeals to my sense of humor as well as to my sense of fair play. It was
written by a Singapore physician, for whom the dollar cost of recertification
was over $10,000. His nerves took a beating as well as his bank account.
Speaking of banking, here is the authors’ final observation:
Physicians
should be able to choose a programme that best fits their scope of practice.
However, it is likely that, besides the efforts put in by physicians themselves
as a commitment to professionalism, the economic price will be borne by
patients in the name of public assurance of medical competence and safety. If
the burden becomes too onerous, one can always become a banker. —
Teo, B. W. and S. Subramanian (2015). “Maintenance of certification: the
price of medical professionalism is $10,108.05, two weeks leave and five white
hairs.” Singapore Med J 56(4): 181-183.
I’m a very busy consultation-liaison
psychiatrist in a large academic medical center. I think there are alternatives
to MOC which don’t waste my time with modules and tests which typically are not
relevant to my practice.
For example, I have
followed the model of the practice-based learning and improvement competency at
the University of Iowa by using what Drs. William R. Yates and Terri Gerdes
called the “problem-based learning” case conference. The abstract for their
paper describes it:
“Problem-based
learning (PBL) is a method of instruction gaining increased attention and
implementation in medical education. In PBL there is increased emphasis on the
development of problem-solving skills, small group dynamics, and self-directed
methods of education. A weekly PBL conference was started by a university
consultation psychiatry team. One active consultation service problem was
identified each week for study. Multiple computerized and library resources
provided access to additional information for problem solving. After 1 year of
the PBL conference, an evaluation was performed to determine the effectiveness
of this approach. We reviewed the content of problems identified, and conducted
a survey of conference participants. The most common types of problem
categories identified for the conference were pharmacology of psychiatric and
medical drugs (28%), mental status effects of medical illnesses (28%),
consultation psychiatry process issues (20%), and diagnostic issues (13%).
Computerized literature searches provided significant assistance for some
problems and less for other problems. The PBL conference was ranked the highest
of all the psychiatry resident educational formats. PBL appears to be a
successful method for assisting in patient management and in resident and
medical student psychiatry education.”
This is now called the Clinical Problems in Consultation-Psychiatry (CPCP) and trainees from medical students to residents participate as presenters. The format is also used as a framework for the Consultation-Liaison Psychiatry Interest Group at Iowa. There are lively discussions at these meetings, to which colleagues from other medical specialty departments are invited. The model for this was adapted from that reported by Puri and colleagues.
Yet these and other
creative practice-based learning efforts which are relevant to our practices
are not on the approved product list for CME and Self-Assessment at the ABPN.
To be sure, one
Performance in Practice (PIP) clinical module (mentioned above) that I and one
of our residents submitted to ABPN was approved. This was the Delirium Clinical
Module, for which we received congratulations from leaders of the Academy of
Consultation-Liaison Psychiatry (ACLP). This is a clinically relevant exercise
which could be useful to many medical specialists, not just psychiatrists. It would
also be important for enhancing patient safety—which is the whole idea of
practice-based learning.
I have worked with the Iowa Medical Society (IMS) to get resolutions adopted as IMS Policy which support the principle of lifelong learning and which oppose both MOC and Maintenance of Licensure (MOL).
The idea that if doctors don’t develop a
system for monitoring continued competence in psychiatry, other groups will do
it for us likely comes from what are essentially cases of medical malpractice.
This was probably what was meant by the ABPN response to my criticisms of the
MOC process several years ago, which was that part of the reason for MOC was
the public’s demand for a way to hold physicians accountable for harming
patients.
One of the papers citing this problem was by
Shaw and colleagues. The authors mention “damaging high-profile cases” one
example of which triggered the Bristol Inquiry in the United Kingdom leading to
the “development of a compulsory integrated regulatory program with oversight
in all levels of medical care from hospital systems to the practice of
individual physicians.
This is the United Kingdom’s revalidation
program, which is similar to MOC or perhaps more properly, MOL.
The irony is that the
American Board of Medical Specialties (ABMS) and member specialty boards
including the ABPN claim the American version of MOC is a voluntary program and
that this is “self-regulation.” It’s not clear who else would “do it for us”
though—some government agency? It’s hardly necessary when, as Dr. Paul Mathews
reported recently, some private insurance payers require participation in MOC.
He’s a voluntary board member of the National Board of Physicians and Surgeons
(NBPAS), which is a newly established alternative to the ABMS which doesn’t
require MOC participation:
“WHAT DO PRIVATE PAYERS GAIN FROM REQUIRING
MOC?
As a volunteer board member of NBPAS (no
compensation or honorarium as opposed to the salaries of ABMS board members,
which can range from $300,000 to greater than $800,000), I have often wondered
why private payers require MOC when Medicare does not require board
certification or MOC. The answer is quite disturbing. Private payers actually
participate in certification, which is issued by the National Committee of Quality
Assurance (NCQA). Margaret E. O’Kane is the founder and president of the NCQA,
and she is also a member of the ABMS Board of Directors. The NCQA requires
private payers to require physicians to participate in MOC in order to be NCQA
certified. Thus, anyone contracting with a private payer will require MOC. In
the conflicted case of Ms. O’Kane, she profits from the NCQA requiring private
payers to require physicians to participate in MOC, and then she profits again
from her ABMS position when said physicians must pay to comply with MOC
requirements”
This raises another concern about MOC, which
is the ever-present cloud of suspicion the ABMS and some of the member
specialty boards are under, especially the American Board of Internal Medicine
(ABIM).
According to Charles
Cutler, M.D., M.A.C.P., in the winter 2016-17 issue of Philadelphia Medicine,
Philadelphia County Medical Society, in an issue entitled “Is The ABIM Too
Broken to Fix?” article “A Message to the ABIM: Reign in Spending and Stop
Turning Staff into Millionaires,” reforms should in fact include doing just
what the title says and much more.
Board executives, especially CEOs, make what
appear to be enormous six-figure incomes from the MOC programs, including Dr.
Larry Faulkner, M.D., the President and CEO of the ABPN who earned over
$900,000 in 2014 according to IRS Form 990.
Those with a low
opinion of the adage about “…the wise old doctor who improves with experience…”
should probably be shared with those board leaders who made the arbitrary
cutoff date for requiring participation in MOC, grandfathering physicians board
certified prior to 1994, thereby exempting them from the program.
Participation in MOC would make more sense if there were credible research evidence that it improves patient outcomes. However, the studies tend not to support this conclusion.
And MOC is not
supported by most physicians, according the results of a Mayo Clinic
Proceedings survey, indicating that “Dissatisfaction with current MOC programs
is pervasive and not localized to specific sectors or specialties. Unresolved
negative perceptions will impede optimal physician engagement in MOC.”
Finally, any
suggestion to sign up right away for MOC probably should be preceded by another
important action, which is to first check with your institution to see if MOC
participation or, indeed, board certification itself, is a condition of
employment. It may not be.
What are the
alternatives to the MOC approach? They depend on one’s level of attachment to
keeping some sort of certification status.
There is the
alternative National Board of Physicians and Surgeons (NBPAS), which was
launched in 2015 and offers board re-certification without MOC or
recertification examination requirements. There is a nominal fee and CME
requirement. A previous ABMS certification is also required, but if that has
lapsed one can still obtain certification by submitting a higher number of CME
credits.
NBPAS leaders are
very much aware that certain private insurance payers require MOC participation.
It was the top priority for NBPAS in 2017. See their website for full details
about their re-certification process.
Physicians could simply forgo MOC or alternative certifications, which would probably raise more anxiety. For example, if one simply stops sending money to the ABPN toward MOC requirements and declines to sit for the recertification examination, then after the general board expires one would be identified as “Certified-not meeting MOC requirements.” But after the examination date passes, you’re Not Certified. The prudent diplomate should first check with ABPN for clarification of specific details and should check their employer’s expectations and insurance payer rules about MOC.
In my opinion, there
ought to be a choice to participate in MOC or some other vehicle for fulfilling
the principle of lifelong learning. Those who want MOC should keep it. Those
who don’t should be allowed to continue using the method they’re most
comfortable with for maintaining their knowledge and clinical skills, including
CME and other creative methods for staying current with the medical literature.
Our patients deserve
at least this much.
“It is far better to light the candle than to curse the darkness”—attributed to William L. Watkinson in a 1907 sermon according to Quote Investigator.
William L. Watkinson
References:
Pato, M. T., et al. (2013). “Journal club
for faculty or residents: A model for lifelong learning and maintenance of
certification.” International Review of Psychiatry 25(3): 276-283.
Brooks, E. M., et al. (2017). “What
Family Physicians Really Think of Maintenance of Certification Part II
Activities.” J Contin Educ Health Prof 37(4): 223-229.
Tieder, J. S., et al. (2017). “A Survey
of Perceived Effectiveness of Part 4 Maintenance of Certification.” Hosp
Pediatr 7(11): 642-648.
Stoff, B. K., et al. (2018). “Maintenance
of Certification: A grandfatherly ethical analysis.” Journal of the
American Academy of Dermatology 78(3): 627-630.
Glover, M., et al. (2017). “Participation
and payments in the PQRS Maintenance of Certification Program: Implications for
future merit based payment programs.” Healthcare.
Teo, B. W. and S. Subramanian (2015).
“Maintenance of certification: the price of medical professionalism is
$10,108.05, two weeks leave and five white hairs.” Singapore Med J 56(4):
181-183.
More References:
1. Boland, R., MD, Maintenance
of Certification, in Psychiatric Times. 2017, UBM Medica.
2. Knoll, J.L., IV, MD;
Cotoman, Dan, MD, Maintenance of Certification and Self-Mortification, in
Psychiatric Times. 2017, UBM Medica.
3. Shanafelt, T.D., L.N.
Dyrbye, and C.P. West, Addressing physician burnout: The way forward. JAMA,
2017. 317(9): p. 901-902.
4. Bright, R.P. and L. Krahn,
Value-added education: enhancing learning on the psychiatry inpatient
consultation service. Acad Psychiatry, 2015. 39(2): p. 212-4.
5. Yates, W.R. and T.T.
Gerdes, Problem-based learning in consultation psychiatry. Gen Hosp Psychiatry,
1996. 18(3): p. 139-44.
6. Puri, N.V., P. Azzam, and
P. Gopalan, Introducing a psychosomatic medicine interest group for psychiatry
residents. Psychosomatics, 2015. 56(3): p. 268-73.
7. Shaw, K., et al., Shared
medical regulation in a time of increasing calls for accountability and
transparency: comparison of recertification in the United States, Canada, and
the United Kingdom. JAMA, 2009. 302(18): p. 2008-14.
8. Mathew, P., MD, MOC and
Physician Burnout: Treating the Cause, Not the Symptoms, in Practical
Neurology. 2016.
9. Cutler, C., MD, MACP, A
Message to the ABIM: Reign in Spending and Stop Turning Staff into Millionaires,
in Philadelphia Medicine: The Official Magazine of the Philadelphia County
Medical Society Philadelphia Medicine 2016, Hoffmann Publishing Group, Inc.
10. Gray, B.M., et al.,
Association between imposition of a Maintenance of Certification requirement
and ambulatory care-sensitive hospitalizations and health care costs. JAMA,
2014. 312(22): p. 2348-57.
11. Hayes, J., et al.,
Association between physician time-unlimited vs time-limited internal medicine
board certification and ambulatory patient care quality. JAMA, 2014. 312(22):
p. 2358-63.
12. Cook, D.A., et al.,
Physician Attitudes About Maintenance of Certification. Mayo Clinic
Proceedings, 2016. 91(10): p. 1336-1345.
About 15 years ago, I left my position at the University of Iowa to work somewhere else. The spiral notebook with a picture of someone crossing a bridge and the fine birdhouse in the picture above were going away gifts.
There were many touching messages in the little book. Friends wished me well and reminded me to “Keep up on all the birds in your new neighborhood.” I was a birdwatcher then and I’m reaching back for that now.
One of them said, “I hope you find your new position to be everything you want it to be.”
I did not. I returned and everything I left was somehow changed. But I was the same old Jim. And later I left again–and again returned. And now the third leave-taking is approaching–retirement. I will not return. Maybe then my spirit will not be nostalgic.