I missed the recent notice in the last couple of days that the CDC ACIP meeting was postponed for today and tomorrow. Me and more than a couple dozen people were kept waiting for a half hour before I got suspicious and looked it up. There’s a CIDRAP story posted yesterday that explains the “delay.”
There was a federal district judge ruling two days ago “…temporarily blocks every major vaccine policy change made by President Trump’s administration over the past year. The ruling came in response to the ongoing lawsuit filed by the American Academy of Pediatrics (AAP) and five other major medical organizations against Health and Human Services (HHS) Secretary Robert F. Kennedy Jr.”
There is no message on the CDC ACIP webcast site about this and at the moment I’m writing this, there are still 41 people waiting for the YouTube webcast. I figured they were just getting coffee and bagels. There should have been an announcement by the CDC ACIP.
It’s been a while since the last CDC ACIP meeting. It’s scheduled for March 18, 2026, 8 AM to 5 PM EST and March 19, 2026, 8 AM to 5 PM EST, according the notice on the Federal Register.
There are over 1500 comments and the one I thought was the best was by the Vaccinate Your Family (VFY) organization, which you can read on their website.
According to the notice: “The agenda will include updates on ACIP Workgroups and discussions on COVID-19 vaccine injuries and Long-COVID and ACIP recommendation methodology. Recommendation votes may be scheduled for COVID-19 vaccine injuries and Long-COVID and ACIP recommendation methodology. Agenda items are subject to change as priorities dictate. For more information on the meeting agenda, visit https://www.cdc.gov/acip/meetings/index.html.
Meeting Information: The meeting will be webcast live via the World Wide Web.”
I’ve been comparing the Iowa legislature bills on allowing ivermectin to be available over-the-counter in pharmacies. There were two of them and then there was one.
In the first bill, HF 2056, the language in it seemed to strongly direct pharmacists to make ivermectin available by using the word “shall”:
” The medical director of the department shall establish a standing order authorizing the dispensing of hydroxychloroquine and ivermectin by a pharmacist.
Notwithstanding any provision of law to the contrary, a pharmacist shall dispense hydroxychloroquine or ivermectin to a patient who is at least eighteen years of age, upon the request of a patient, pursuant to a standing order established by the medical director of the department in accordance with this section.”
The bill goes to say that “A pharmacist shall be immune from criminal and civil liability arising from any damages caused by the dispensing or use of…” these agents.
In Governor Reynolds version of the bill (included in HF 2676, successor to HSB 964), at least today, uses the word “may”:
“Sec. 17. NEW SECTION. 126.24 Ivermectin—prescription drug order not required.
A pharmacist or pharmacy may distribute ivermectin for human consumption as an over-the-counter medicine.
A pharmacist or pharmacy shall not be subject to professional discipline or civil or criminal penalties for the distribution of ivermectin pursuant to this section.”
I think the word “may” in Governor Reynolds’s bill implies a pharmacist can distribute ivermectin, but is not necessarily required to do so. In the HF 2056 bill (which died in the first funnel) the word “shall” implies the pharmacist must do so. Hydroxychloroquine is not mentioned in the governor’s version of the bill.
Although neither of these bills mentioned why the ivermectin bill is being introduced, I think it’s clear that some people think it could be an alternative to vaccines for Covid-19. Because research shows ivermectin is ineffective for treating Covid-19 and because they’re not FDA approved for that, I doubt any pharmacist would choose to do what the bill says.
This seems to be turning into a weird game of “Captain, May I?” I think the majority of pharmacists would rather not play.
I saw a story in the Iowa Capital Dispatch by Robin Opsahl today that there’s a bill in the Iowa legislature which seeks to make the drugs ivermectin and hydroxychloroquine over-the-counter (OTC) in Iowa. It doesn’t actually specify the reason why but it’s probably because some Iowans want the drugs available to treat Covid-19. I think the motivation sounds similar to the bills introduced in March of 2025 which were designed to make it illegal to get mRNA vaccines for Covid-19 in Iowa. They both died in funnel week last year.
The bill was discussed yesterday and, while there were 3 commenters in favor of it, there are several reasons to be suspicious of whether it would be a good thing for Iowans. Both ivermectin and hydroxychloroquine were studied for evidence of efficacy for Covid-19 and the studies failed to show that.
However, the Iowa bill HF 2056 seeks to make both available OTC and require pharmacies not only make it available but protect the pharmacist from legal or criminal liability for any harms that might result from its use.
While you can find news stories saying simply that 4 states (Tennessee, Idaho, Arkansas, and Idaho) have adopted similar laws, there is at least one recent follow up news story indicating that the pharmacists still have some reservations.
A Boise, Idaho pharmacist says he’ll dispense ivermectin to callers—as long as they have a doctor’s note. Most callers don’t have a parasitic infection. The pharmacist points out that, while the Idaho law says he can dispense ivermectin without a prescription, the FDA hasn’t approved it to be used this way. “It’s not designed or packaged for retail sale,” according to the pharmacist. It’s not made for OTC use.
There’s also a hitch when it comes to health insurance coverage for OTC drugs, implying you might have to pay out of pocket. Arkansas and Tennessee pharmacists say that, despite the law change allowing OTC sale of ivermectin in their states, they won’t sell it that way.
I hope their example will be followed by the other states who seem to be going the same way as Iowa. On the other hand, I’m pretty sure there might be plenty of conscientious objectors in Iowa who might slow down the legal push to get either hydroxychloroquine or ivermectin OTC.
Just because lawmakers put in a lot of language in a bill in an effort to persuade pharmacists that they won’t get sued or go to jail if they always give the customers what they want doesn’t mean they’ll obey a law based on misinformation and which makes them disobey their principles. I don’t understand how the legislative machinery works but I’m hoping the fate for this bill will be the same as what happened to those from last year.
There was a lot to digest in today’s CDC ACIP meeting on Covid-19 vaccines. I missed the morning sessions but managed to see a few of the afternoon presentations.
The presentation by Dr. Retsef Levi, PhD, MIT, ACIP Work Group Chair, the Covid -19 Vaccine Discussion Framing Work Group (WG) was basically pretty critical of the Covid-19 vaccines in general.
The opposing reply to this (favorable to vaccines) was put together by University of Iowa’s Dr. Stanley Perlman, Dr. H. Bernstein, and Dr. M. Miglis, Additional Workgroup Considerations in Covid-19 Vaccination Policy and Practice.
For a change, I listened to the Public Comment section. I usually have not paid attention to them because most of the speakers were opposed to vaccines. Today was different. All of them were strongly supportive of vaccines.
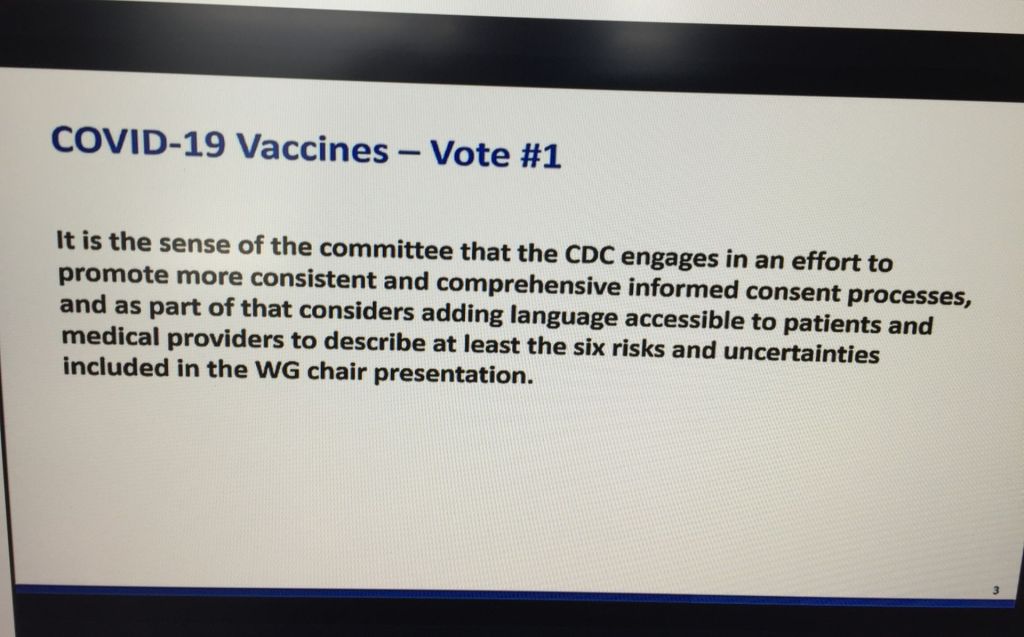
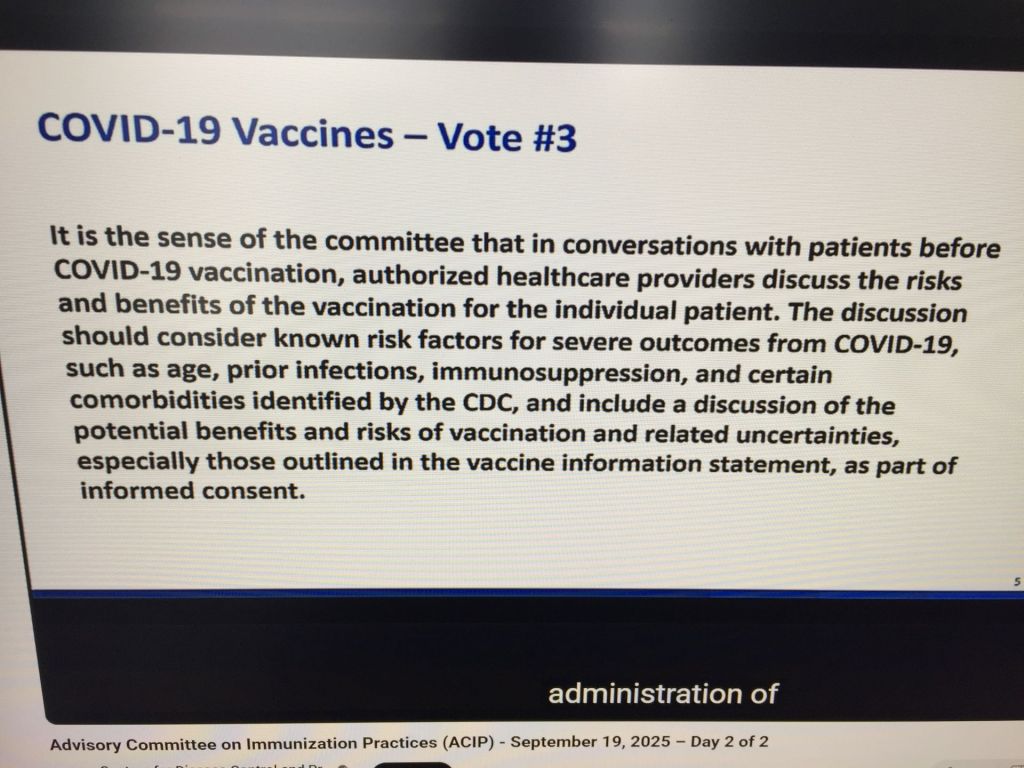
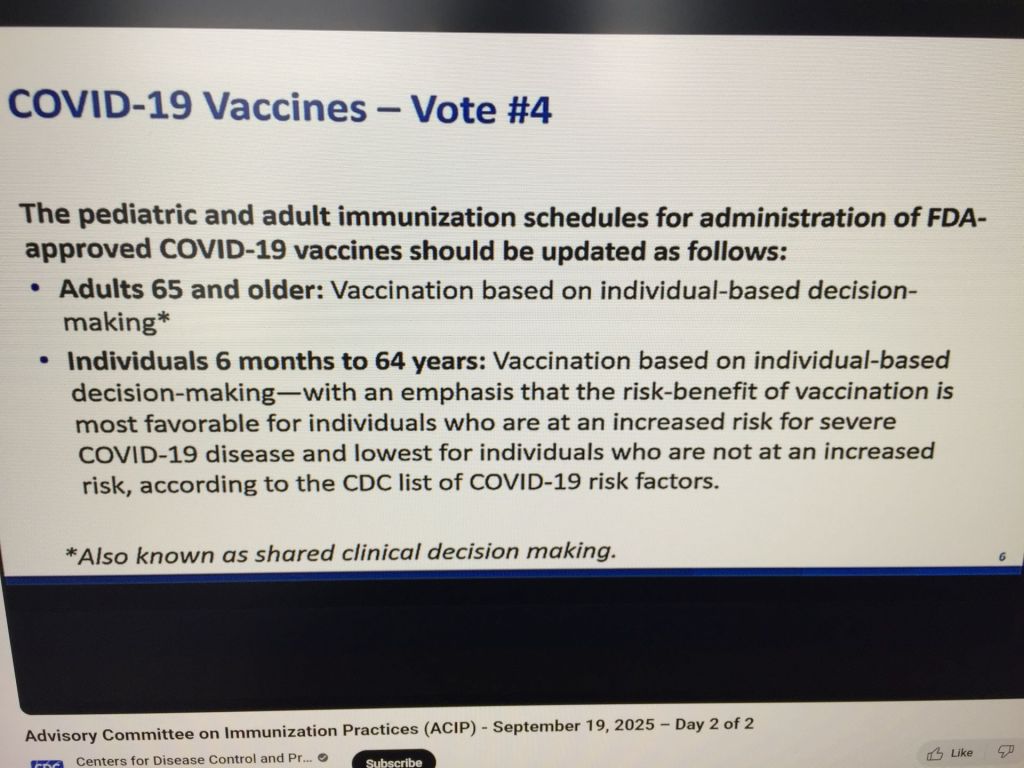
There is a bottom line to this. I watched the voting session, which was very interesting. There were 4 voting questions. I had to take pictures of them because they were not included in the on-line schedule. It was easily the most interesting session of the afternoon, at least for me.
Voting question 1: all but one member voted “yes,” the committee chair Kulldorff voted “no.”
Voting question 2: one member suggested striking this one, but they voted anyway. What’s worrisome is that it was split between the yes and no votes; only the chair, Kulldorff, could break it and he voted “no.” Looks like common sense won; otherwise it would have made access very difficult.
Voting question 3: The video lost audio for a long time, but eventually it turned out that the votes were “yes” unanimously on the assumption that pharmacists counted as “health care providers.”
Voting question 4: The votes were all “yes,” mainly because they decided that pharmacists could make this work. One member questioned the wording which suggested that you needed to talk to your doctor about getting the vaccine because of the wording “shared clinical decision-making.” They glossed over it.
It looks like access to the Covid-19 vaccine will remain mostly open for now.
I have just noticed that there are over 5,000 comments posted on the comments section of regulations.gov in the section entitled Meeting of the Advisory Committee on Immunization Practices-September 2025.
The link to the comment section is on the CDC ACIP meeting announcement web page, “Written Public Comments.”
This is the first time I’ve seen a written comment section like this for the meetings. I think it gives people a sense of what health care professionals and others think about how things are going with the current approach to preventive medicine at the CDC.
The upcoming meeting on the MMVR and Covid-19 vaccines will include voting on the MMVR and Covid-19 vaccines. Usually, the committee posts the actual voting questions, which so far I have not seen on the meeting agenda. I’ll be looking for them in the next couple of days.
Here is the linkto the Center for Infectious Disease and Policy (CIDRAP) at the University of Minnesota article which bears directly on the meeting topics.
I just noticed that the CDC ACIP draft agenda for upcoming meeting on September 18th and 19th has been posted. There will be votes on the MMRV, Hepatitis B, and Covid-19 vaccines.
Sena and I got our latest updated seasonal Covid-19 and flu vaccines today. Manpower was low at Walgreens so we ended up sitting for about an hour, but otherwise this was a routine trip. We’re thankful.
We noticed there were a few people waiting—mostly our age. No word up yet on the CDC ACIP site about the Sept. 18-19 meeting as far as an agenda, speakers, or slides.