Transplantation psychiatry is a special setting for consultation-liaison psychiatrists. Mainly, they work in organ transplant centers. The democratization of health care over many years, along with the relative scarcity of transplantation psychiatrists, has led to many other professionals conducting the psychosocial assessments for evaluating organ transplant candidates.
It’s a complicated field with many stakeholders. The scarcity of organs often leads to great anxiety in patients and their supporters. Anxiety can complicate the assessment phase, the waiting phase, and the post-transplant phase as well.
The most frequent question that consultees from the transplant team ask is whether the candidate is a good risk for receiving an organ that is in short supply, which therefore must be allocated carefully, and of which the candidate must be prepared to be a good steward. Psychosocial screening is a feature of most transplant programs. Rather than seeing one’s self as a gatekeeper, most experts agree that the most useful part of the psychosocial screening process is to identify psychosocial factors that would interfere with the candidate’s successful adaptation to life posttransplant, and to develop a plan for managing them using available resources.
Occasionally, despite my being in phased retirement, I get a
reminder that my colleagues may need some advice about an issue for which I might
be a useful source of institutional memory.
One of them is the psychiatric consultation for assessment of candidates for organ transplant. I have a slide set and a YouTube video that are still useful as long as viewers remember that some of the slides and the text are dated.
For example, the video refers to my former blog The
Practical Psychosomaticist (which l later renamed the Practical C-L
Psychiatrist), and which I cancelled June 1, 2018. The references are also old,
but much of the information is still useful.
I’ve included both the video and the slides for the Dirty Dozen on Psychosocial Assessments for Organ Transplant. You can view the slides and just listen to the audio like a voice over in the video. That way you don’t have to giggle at the back of my head and my camera comically reflected in the office window behind me. Turn on the video, click in the slide set to open it, and listen to my prompts for which slide I’m on.
Use this as a voice over for slide set below
The most frequent question that
consultees from the transplant team ask is whether the candidate is a good risk
for receiving an organ that is in short supply, which therefore must be
allocated carefully, and of which the candidate must be prepared to be a good
steward. Psychosocial screening is a feature of most transplant programs.
Rather than seeing ones self as a gatekeeper, most experts agree that the most
useful part of the psychosocial screening process is to identify psychosocial
factors that would interfere with the candidate’s successful adaptation to life
posttransplant, and to develop a plan for managing them using available
resources.
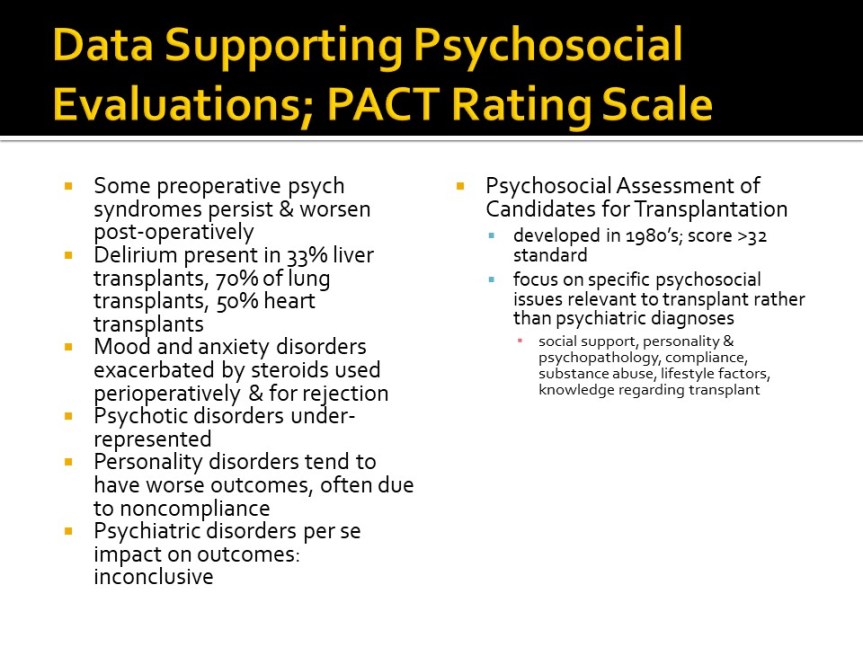
The evaluation phase is critical to diagnosis of major psychiatric problems and to treatment planning for evidence-based interventions. However, providing follow-up through the other phases of transplant allow optimizing the development of a therapeutic alliance to foster adherence to both psychiatric and medical treatment and further evaluation of psychosocial challenges as well. The waiting phase is a very stressful time and often the candidate must tolerate deteriorating health while watching others transplanted sooner. In the post-transplant period, about 20% of patients develop any psychiatric disorder, most notably depression and PTSD.
There’s a triple advocacy role for evaluators conducting organ
transplant assessments: advocacy for the patient; for the persons on the
waiting list; and for society in general in terms of husbanding allocation of
scarce resource (“organ stewardship”).
That makes it critically important to examine the nature of the
therapeutic alliance.
Transactional/Adversarial or Transformational?
Transactional/Adversarial:
Atmosphere is typically highly charged emotionally, with
a sense of urgency.
Interrogation mode rather than exploration of motivations
and feelings. Focus is on past rather than future, exclusive approach with
emphasis on utilitarian paradigm and wait list advocacy. Methodically and
meticulously confrontive; blaming. Team asks “Who else could we help?” Little
or no interpersonal room to witness the patient make sense of impending death.
Withholding,
rejecting, paternal, authoritarian (rather than shared) experience.
Win/Lose or
Lose/Win.
Transformational:
Atmosphere
of created space for calmer review and listening for understanding.
More likely
to have focus on future rather than past, and an inclusive approach with
emphasis on medical necessity paradigm and patient advocacy. Affirming and
supportive of change. The team asks, “What would we need to do in order to
help?” May be a better opportunity to be a witness to coming to terms with
imminent death.
Shared
experience, with both participants on a more level playing field.
Win/Win.
This is a very complex and challenging aspect of Consultation-Liaison Psychiatry and, probably in part because we’re in short supply in many areas, many transplant centers rely on written assessment batteries or checklists. It’s hard to do justice to the topic in a blog post. I hope it’s helpful.
References:
1. Anne
M. Larson, J.P.R.J.F.T.J.D.E.L.L.S.H.J.S.R.F.V.S.G.O.A.O.S.W., Acetaminophen-induced
acute liver failure: Results of a United States multicenter,
prospective study. Hepatology, 2005. 42(6): p. 1364-1372.
2. DiMartini,
A.F., M.D.,, M.A. Dew, M.D.,, and P.T. Trzepacz, M.D.,, Organ
Transplantation, in Textbook of Psychosomatic Medicine, J.L.M.D.
Levenson, Editor. 2005, American Psychiatric Publishing, Inc.: Washington, DC.
p. 675-700.
3. Huffman,
J.C., M.K. Popkin, and T.A. Stern, Psychiatric considerations in the patient
receiving organ transplantation: a clinical case conference. General
Hospital Psychiatry, 2003. 25(6): p. 484-491.
4. Klapheke,
M.M., The Role of the Psychiatrist in Organ Transplantation. Bulletin of
the Menninger Clinic, 1999. 63(1): p. 13-39.
5. Novack,
V., et al., Deliberate self-poisoning with acetaminophen: A comparison with
other medications. European Journal of Internal Medicine, 2005. 16(8):
p. 585-589.
6. Turjanski,
N. and G.G. LLoyd, Transplantation, in Psychosomatic Medicine,
M.J. Blumenfield, M.D. and J.J. Strain, M.D., Editors. 2006, Lippincott
Williams & Wilkins: New York.
p. 389-399.